

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Since the first report of laparoscopic distal pancreatectomy with splenectomy in the 1990s, the procedure has been increasingly performed to treat lesions of the distal pancreas [12]. However, splenectomy is associated with a lifetime risk of developing an overwhelming post-splenectomy infection (OPSI), and OPSIs are associated with a mortality of 50% to 70% [3]. Therefore, patients are required to receive preoperative prophylactic vaccinations and make a lifelong commitment to antibiotic treatment for preventing sepsis [456].
Currently, laparoscopic techniques for spleen-preserving distal pancreatectomy have significantly improved, and laparoscopic spleen-preserving distal pancreatectomy (LSPDP) is the preferred approach for treating benign conditions and low-malignancy potential diseases [78910]. In comparison to traditional distal pancreatectomy with splenectomy, LSPDP provides numerous benefits, and LSPDP has gained popularity as a standard treatment for benign neoplasms of the body and tail of the pancreas, and various surgical techniques have been reported [11121314].
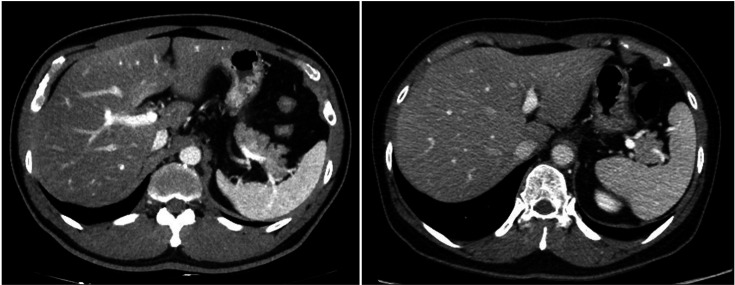
Nevertheless, sometimes, an anatomically challenging patient is encountered where the pancreatic tail tip is located deep inside the splenic hilum, and it can be challenging to perform spleen-preserving distal pancreatectomy without damaging the splenic vessels (Fig. 1). To avoid these risks, alternative surgical techniques, such as central pancreatectomy with pancreaticoenteric anastomosis or partial pancreatic resection, may be considered. Wayne et al. [15] performed a central pancreatectomy without anastomosis of the distal remnant pancreas. In that case series, the authors concluded that central pancreatectomy without pancreaticoenteric anastomosis for lesions in the neck and proximal pancreas was a safe and effective procedure. In addition, no significant complications were noted in their review on central pancreatectomy without pancreaticoenteric anastomosis.
However, the study mentioned earlier, enrolled patients with chronic pancreatitis. This is a crucial point to consider since chronic pancreatitis can lead to changes in the exocrine function of the pancreas, which can make it challenging to apply the study’s findings to patients without chronic pancreatitis. As a result, further research is required to assess the safety and feasibility of leaving a part of the normal pancreas without anastomosis in patients without chronic pancreatitis who require LSPDP.
It is not yet known whether performing a splenectomy to remove the entire pancreas or preserving the spleen and leaving a part of the pancreatic tail is more beneficial, and there have been no studies on leaving the tail of a normal pancreas without anastomosis. Therefore, in the present case series, we investigated whether it was safe and feasible to leave a part of the normal pancreas in anatomically challenging patients undergoing LSPDP.
METHODS
Ethics statement
Every step of the study was carried out after the approval of the Institutional Review Board of Samsung Medical Center (No. SMC 2021-08-145), and all methods were conducted in accordance with the relevant guidelines and regulations. This study was carried out in compliance with the Declaration of Helsinki and the need for written informed consent was waived due to its retrospective nature.
Study population
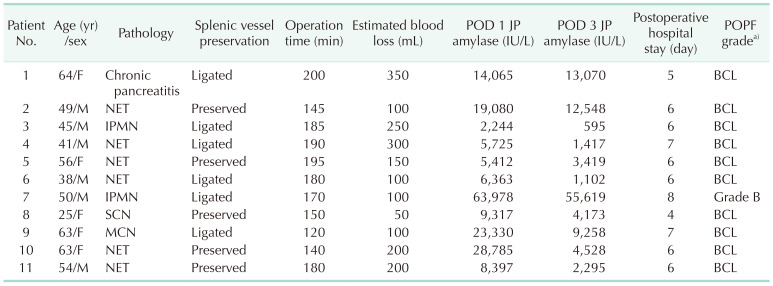
From November 2019 through August 2021, 11 patients underwent LSPDP with remnant pancreatic tails at Samsung Medical Center in Seoul, Korea (Table 1). Each patient in the study was asymptomatic and the lesions were identified incidentally by CT scans or ultrasonography. The medical records of the patients, including the clinical, pathological, and surgical outcomes, were retrospectively reviewed.
Surgical laparoscopic spleen-preserving distal pancreatectomy procedure
There are 2 main LSPDP techniques, depending on whether the splenic vessels are preserved or ligated [1216]. In our institute, we try to preserve the splenic vessels as much as possible; however, in some cases, ligating the splenic vessels is required. Each operation is initiated by exposure of the lower border of the pancreas, followed by dissection from the posterior aspect toward the superior border of the pancreas. After securing a sufficient margin from the mass and transecting the pancreas using a surgical stapling device, the pancreatic dissection proceeds laterally from the medial area, with or without splenic vessels. When it is confirmed that the vascular structure of the spleen is complex and the pancreatic tail is deep inside the splenic hilum, the disease-free pancreas tail is transected using a surgical stapling device or a vessel sealing device, and the remnant pancreas is left at the splenic hilum. A routine frozen section was performed, and negative margins were secured in almost all cases. However, in a few cases, a frozen section was not performed when the characteristics of the tumor showed benign solitary on imaging and operative findings. After applying fibrin glue to both pancreatic stumps, 1 Jackson-Pratt (JP) surgical drain is left in the posterior area of the stomach near the stump.
Definition of postoperative outcomes and clinical strategy
Postoperative morbidity and mortality were noted during hospital admission and 30 days after discharge. Sips of water were attempted by every patient on the morning of postoperative day 1, regardless of what kind of LSPDP was performed. Enteral feeding with a liquid and soft diet was initiated as soon as possible after the patients were hemodynamically stable. A routine postoperative CT scan was performed 5 days after surgery during the hospitalization and a follow-up CT scan was performed about 3 months after surgery to evaluate fluid collection.
Amylase concentrations in the drain fluid were measured daily until removed. In our institution, referring to the enhanced recovery protocol after pancreatic surgery, if the postoperative day 1 amylase drainage concentration was less than 5,000 IU/L, we tried to remove the drain on postoperative day 3 [17]. The criteria for the removal of JP drains predominantly considered monitoring a declining trend in JP amylase levels. However, the actual timing of drain removal was determined by the surgeon’s preference, and the drain of all the patients in this study cohort was removed on postoperative day 3. Postoperative pancreatic fistula (POPF) was graded according to the International Study Group of Pancreatic Fistula definition and grading system [18].
RESULTS
The mean age of the patients was 49.8 ± 12.1 years (range, 34–77 years), and there were 6 male and 5 female patients in the study (Table 1). The pathological outcomes of patients included 2 patients with intraductal papillary mucinous neoplasms, 6 with neuroendocrine tumors, 2 with cystic neoplasms, and 1 with chronic pancreatitis. The mean operative time was 168.6 ± 26.0 minutes, the estimated blood loss was 172.7 ± 95.8 mL, and the postoperative length of stay was 6.1 ± 1.0 days (range, 4–8 days). The mean postoperative day 1 JP amylase concentration in the patients was 16,972.4 ± 17,675.3 IU/L (range, 2,244–63,978 IU/L), and the postoperative day 3 JP amylase concentration was 9,820.4 ± 15,827.4 IU/L (range, 595–55,619 IU/L). Splenic vessels were ligated in 6 cases and preserved in 5 cases. Splenic artery ligated patients had splenic infarction, however, some splenic arterial flow was identified in the short gastric vessel or surrounding collateral vessels. There were no patients who developed clinical symptoms related to splenic artery ligation. The pancreas tail was transected using an energy device in 4 cases, while a surgical stapling device was used in the remaining cases.
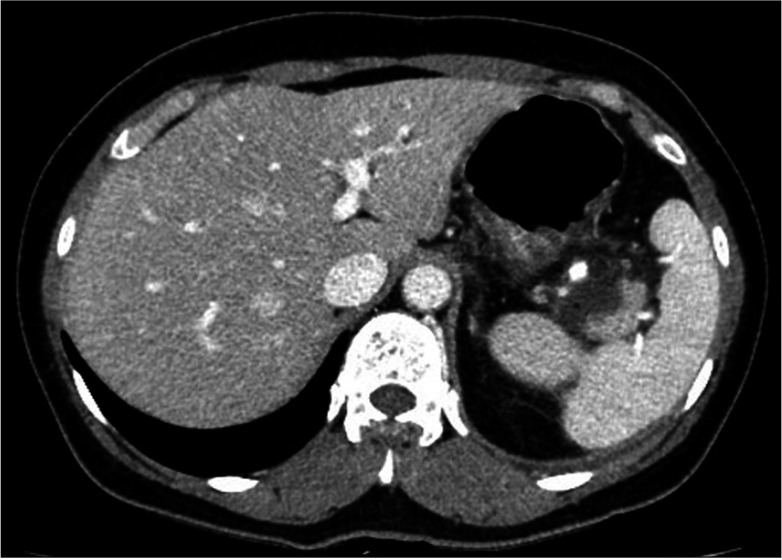
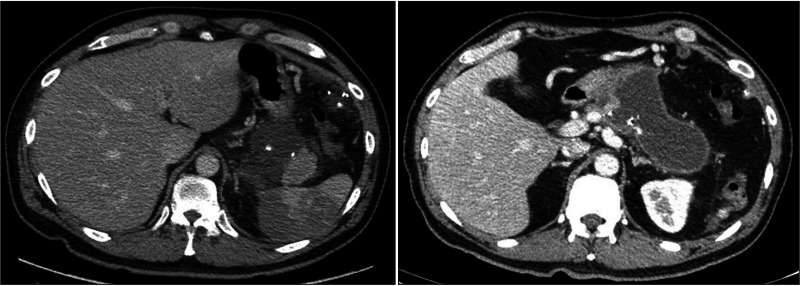
Regarding POPF, in 10 of the 11 patients, only the pancreatic tail was left on the splenic hilum inside the distal portion of the splenic vessel (Fig. 2). Intraabdominal fluid had collected, which was naturally resolved. However, another patient with a remnant pancreatic tail above the hilar vessels was readmitted due to grade B POPF with fever and underwent gastrocystostomy (Fig. 3).
DISCUSSION
Preservation of the spleen provides numerous advantages, including reduced risk of postoperative complications, such as infections, and improved immune function. In fact, splenectomy performed during other major abdominal surgeries has been found to be associated with increased postoperative complications, including infections [7919]. In addition, the risk of OPSI and concerns about potential sepsis-related hospitalization after splenectomy have further emphasized the importance of spleen preservation [2021]. The platelet count may be elevated after splenectomy and was reported to increase the risk for thromboembolic complications [22]. Additional advantages of spleen preservation were observed as less fatigue and better general condition and quality of life. Therefore, spleen-preserving techniques have gained more attention, especially in surgeries such as distal pancreatectomy, where spleen preservation is possible without compromising oncological principles.
To elaborate further, the preservation of splenic blood flow during spleen-preserving distal pancreatectomy is a crucial step to ensure the functionality and viability of the spleen. There are 2 main surgical techniques used to achieve this: the splenic vessel preserving technique (also known as the Kimura technique) and the Warshaw technique [1216]. The splenic vessel preserving technique involves the dissection of both the splenic artery and vein from the pancreas while preserving their integrity. This technique allows for the preservation of normal blood flow to the spleen, which is important for its function and viability. The Kimura technique was first described by Kimura et al. [23] in 1996 and has since become a widely used method for spleen-preserving distal pancreatectomy. In contrast, the Warshaw technique involves the resection of the splenic artery and vein along with the body and tail of the pancreas, leaving the spleen dependent on the short gastric and left gastroepiploic vessels for perfusion. This technique is particularly useful in cases where the splenic vessels cannot be preserved due to anatomic variations or technical difficulties. However, it carries a higher risk of spleen infarction or ischemia if the blood supply through the short gastric and left gastroepiploic vessels is inadequate. In general, the Warshaw technique can be advantageous for LSPDP because it is a relatively simple procedure. However, both techniques have advantages and disadvantages, and the choice of technique depends on the individual patient’s anatomy and the surgeon’s experience and preference. Proper preservation of splenic blood flow is crucial for a successful spleen-preserving distal pancreatectomy and a positive surgical outcome [2425].
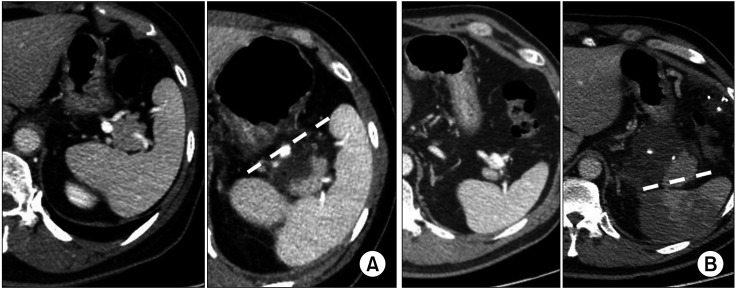
We perform surgery using both techniques described above. However, sometimes, a pancreatic tail deep in the splenic hilum is surrounded by splenic vessels, and it is difficult to treat the vascular structures. Under such circumstances, there is a high risk of vascular injury, making it difficult to preserve the spleen using the previously mentioned surgical techniques. When a vascular injury occurs, the operation must be converted to a laparotomy or unintended splenectomy may occur, which could have serious consequences. The method of remnant pancreas formation is a relatively alternative technique that is used as a method of spleen preservation in anatomically challenging patients. The technique involves leaving a small portion of the pancreatic tail transected within the splenic hilum while preserving the integrity of the splenic vessels. This approach is particularly useful in cases where the splenic vessels cannot be preserved due to anatomical variations or technical difficulties, making it difficult to perform spleen-preserving distal pancreatectomy without damaging the splenic vessels. The outcomes of this technique have shown promising results, as it has been found to be relatively safe and feasible. Of course, it is always preferable to remove the entire pancreatic tail if possible, but in challenging vascular situations, leaving a small remnant tail in the splenic hilum may be a viable option to consider, especially if it can avoid the need for conversion to open surgery or unintended splenectomy. As the standard for resection, the remnant pancreatic tail is formed in the spleen hilum, and this imaginary line can be suggested as an at least acceptable resection line (Fig. 4).
In this study, it was noted that the enrolled patients did not exhibit any signs of abnormal exocrine function during perioperative examination or clinical features, and the pancreas appeared to have a normal texture during surgery. Despite the high concentrations of drainage amylase, the drain was removed on postoperative day 3, which may be considered a relatively early removal. However, it is important to note that the patients were clinically asymptomatic, and it is possible that the elevated drain amylase levels reflected concentrated fluid. The decision to remove the drain early was based on the recommendations of guidelines and concerns regarding infectious complications that may arise from long-term drain insertion [17]. In POPF, it is unclear whether the leak is proximal or in the distal remnant pancreas. The etiology of pancreatic fistula is multifactorial, including patient-related factors, such as age, comorbidities, and pancreatic gland texture, as well as surgical factors, such as the technique used for pancreatic transection and the experience of the surgeon [17]. Nevertheless, in the case of the patients in our study, there were no significant complications related to pancreatic fistula. Although it is unclear whether the leak was proximal or in the distal remnant pancreas, the patients were well managed with conservative treatment such as internal drainage and antibiotics. This indicates that remnant pancreas formation may be a safe and effective method for spleen preservation during distal pancreatectomy in patients with challenging vascular anatomy.
Despite the positive outcomes of this study, there were some limitations that should be considered. First, it was a retrospective study that only involved a single center and a relatively small cohort. Therefore, there may be some selection bias and the generalizability of the results may be limited. Second, it may be difficult to conduct a prospective study because it is not ethical to intentionally leave the pancreas during surgery. However, a larger prospective study with longer follow-up periods could help to validate the effectiveness and safety of this technique. Another limitation is that the study only followed patients for 1 to 3 years, which may not be sufficient to evaluate the long-term clinical features and complications of a remnant pancreas. Therefore, more studies with longer follow-up periods are needed to assess the long-term outcomes of this technique. However, to our knowledge, this was the first case series study to report remnant pancreas formation with LSPDP in patients with a normal pancreas. Despite these limitations, this study is significant in that it provides evidence that remnant pancreas formation with LSPDP can be a safe and feasible method for spleen preservation, especially in cases where there are complicated vascular structures of the pancreatic tail and splenic hilum. This technique could be considered an alternative approach to spleen preservation in patients with anatomical challenges. Further research is needed to determine the long-term outcomes of this technique and to identify the optimal patient selection criteria.
In conclusion, remnant pancreas formation during LSPDP can be considered a feasible and safe method for spleen preservation in patients with complicated vascular structures of the pancreatic tail and splenic hilum. With the growing awareness of the importance of preserving organ function and improving patient outcomes, the development of new techniques for organ preservation is essential. The remnant pancreas formation technique may be an important step towards increasing spleen preservation and improving patient prognosis. By carefully evaluating patients and determining the appropriate candidates for this technique, surgeons can provide patients with the best possible surgical outcomes. Despite limitations such as its retrospective nature and small sample size, the findings are significant and offer a promising approach for anatomically challenging patients. Further research with larger patient populations and longer follow-up periods is needed to fully evaluate the long-term consequences of this approach.
 XML Download
XML Download