

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
Group A streptococcus (GAS) causes a wide spectrum of diseases, ranging from mild infections of the throat and skin, such as pharyngitis and impetigo, to severe infections including necrotizing fasciitis, bacteremia, and toxic shock-like syndrome. The mortality rate due to toxic shock-like syndrome and necrotizing fasciitis has reached 15-25% [1-3]. In addition, it involves the immune mediated sequelae, such as acute rheumatic fever, rheumatic heart disease and post streptococcal glomerulonephritis [4,5]. Annually, about 600 million patients are infected by GAS and over 500,000 die of GAS infections or sequelae [4,6].
Because of high GAS disease burden, epidemiologic surveillance is important to detect changes in the disease pattern in various region or population. A safe and effective vaccine has not been available at the medical field yet [7]. Recently, molecular genetic methods have been used for the epidemiological investigation of GAS infections [8,9]. Many epidemiological studies have focused on GAS characteristics by emm types and clusters [10]. The emm gene of GAS, which is approximately 500-1500 bp in size, encodes the M protein [10]. The M protein of GAS is the major virulence factor that has anti-phagocytic effects towards white blood cells and anti-complement effects to the immune system [11,12]. Classical serotyping methods based on the different surface antigens of M protein have been replaced by sequence typing of the genetically variable N-terminal part of the emm gene [13,14]. emm genotyping is most widely used for epidemiological surveillance of GAS pharyngitis or invasive disease of GAS [15-17]. As emm types are too diverse and complex, emm cluster typing system has been proposed [18,19]. This system classifies most of the 250 different emm types into 48 functional clusters, containing closely related M proteins that share their structural properties [10,18]. The advantage of emm cluster system is that they help to predict the virulence potential and vaccine efficacy by ascribing M protein binding attributes to emm types belonging to the same cluster [18].
In this study, we performed the molecular genetic analysis on GAS isolated from the patients of pharyngitis. Additionally, this study aimed to identify the temporal changes in the emm genotype and cluster, and to investigate the microbiological characteristics and antibiotic resistance of GAS isolated.
MATERIALS AND METHODS
1. Study subjects
A total of 372 patients who showed pharyngitis symptoms or signs from August 2018 to December 2019 in five pediatric clinics in Changwon, were recruited for this study.
2. Research ethics and consent
Prior to proceeding, the study was approved by the Institutional Review Board (IRB) of Gyeongsang National University Changwon Hospital (IRB No. 2018-01-008).
3. Bacteria isolation
Both tonsils were rubbed with a sterilized cotton swab to ensure that bacteria were sufficiently adhering to the cotton swabs. The swab was immediately placed in the transport media (Asan Pharmaceutical, Giheung, Korea), stored at room temperature, and transported to Gyeongsang National University Changwon Hospital for culture. Cotton swabs were inoculated on a blood agar plate (BAP, Asan Pharmaceutical), placed in a general incubator, and incubated for 16-18 hours at 35°C. The next day, small, grayish-white colonies showing complete hemolysis were retrieved from the BAP and identified by bacitracin disk (0.04 U), latex agglutination test (Seroiden Strepto Kit, Eiken, Tokyo, Japan), and/or VITEK mass spectrometry (bioMerieux, Marcy-l'Étoile, France).
4. Antimicrobial susceptibility test
Susceptibility tests were performed for all isolates by disk diffusion method according to the guidelines and interpretative criteria of the Clinical Laboratory and Standards Institute (CLSI) [20]. The following antimicrobial disks of BD BBL Sensi-Disk (Becton-Dickinson Microbiology Systems, Cockeysville, MD, USA) were used: erythromycin (ERY; 15 μg), clindamycin (CLI; 2 μg), tetracycline (TET; 30 μg), and ofloxacin (OFX; 5 μg). Streptococcus pneumoniae ATCC 49619 was used as the control strain. Three resistance phenotypes, such as cMLSB , iMLSB , and M phenotypes, and three resistance genes, such as mefA, ermA, and ermB genes were investigated.
5. Genetic analysis of emm gene
1) emm gene amplification
DNA was directly isolated from colonies grown on BAP using DNase Blood & Tissue Kits (Qiagen, Hilden, Germany). The base sequence of the forward primer was 5'-TAT TCG CTT AGA AAA TTA A-3' and that of the reverse primer was 5'-GCA AGT TCT TCA GCT TGT TT-3'. All protocols and assignments of emm types and subtypes were as described for the GAS database (http://www.cdc.gov/streplab/groupastrep/emm-typing-protocol.htm).
2) Sequencing
Direct sequencing was performed using the amplified emm gene product at Macrogen (Seoul, Korea). Gene sequencing was performed using an ABI PRISM BigDye Terminator cycle sequencing kit (Applied Biosystems, Foster city, CA, USA) and MJ Research PTC-225 Peltier Thermal cycler (MJ Research Inc., Hercules, CA, USA). Bidirectional sequencing was performed and a MOPC (Macrogen Oligonucleotide Purification Cartridge, Macrogen) purified primer (5'-TAT TCG CTT AGA AAA TTA AAA ACA GG-3') and emmseq2 (5'-TAT TCG CTT AGA AAA TTA AAA ACA GG-3'). The fluorescently labeled fragment was purified by the BigDye XTerminator Purification Kit (Thermo Fisher Scientific, Waltham, MA, USA), then loaded into an ABI PRISM 3730XL Analyzer (Applied Biosystems). The nucleotide sequence was compared with the database (https://www2.cdc.gov/vaccines/biotech/strepblast.asp) of the National Center for Biotechnology Information (NCBI) and was determined as the corresponding genotype of the homology was at least 95% . The size of the analyzed nucleotide sequence was approximately 150-200 bp. emm cluster was obtained at the same website above of the NCBI together with emm genotype.
RESULTS
1. Bacterial culture
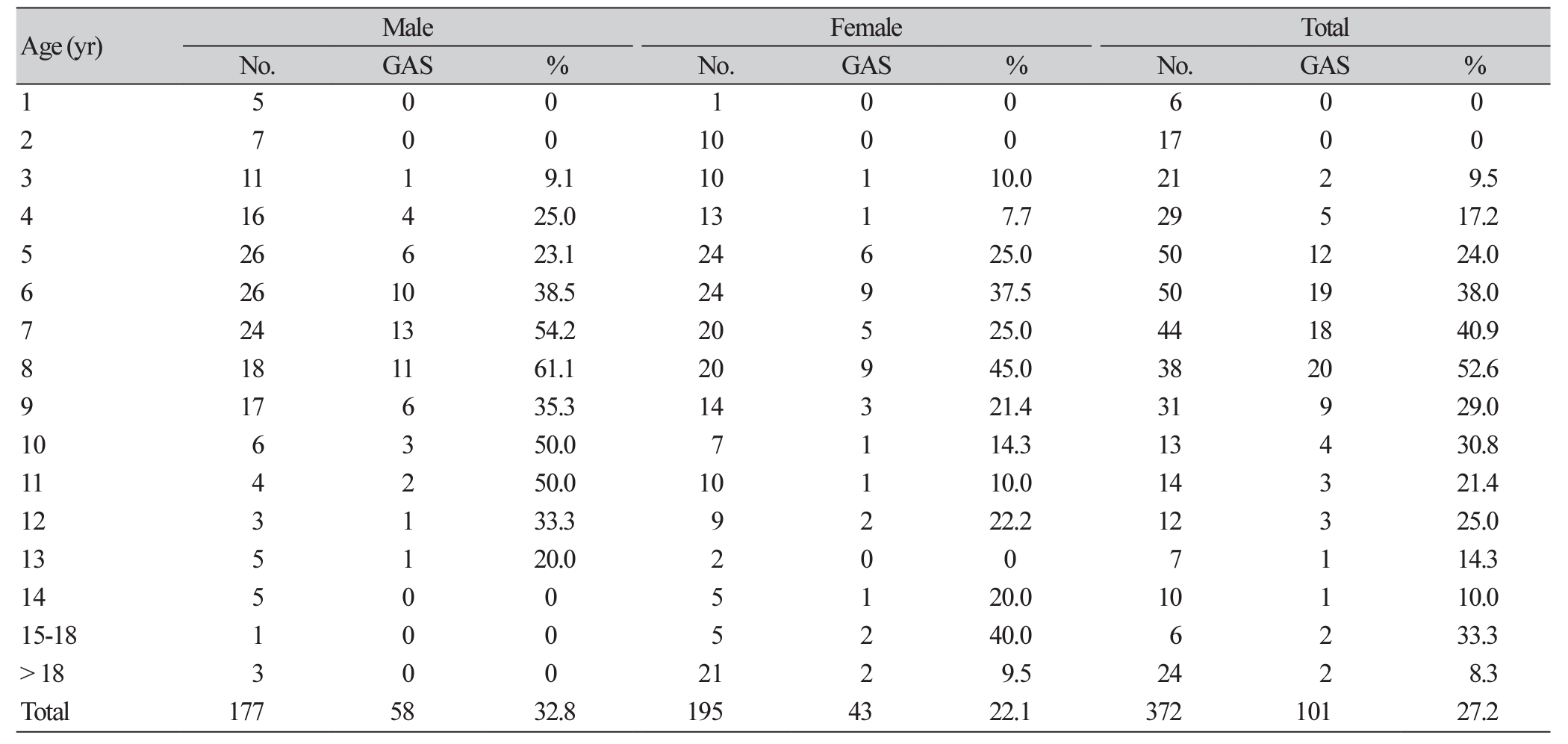
Of 372 patients of acute pharyngitis, GAS was isolated from 101 patients (27.2%), with 57.4% being male. The age distribution of the patients ranged from 1 to 61 years, with an average age of 9.9 years (95% confidence interval [CI], 8.5-11.2 years). The distribution of positive rates by the sex and age is shown in Table 1. In terms of age, six to eight-year-old showed the highest positive rates. Patients under two years of age did not grow GAS.
2. Antibiotic resistance and its mechanism
The results of the antimicrobial susceptibility test showed that only one (1.7%) of 59 GAS, successfully grown in subculture, was resistant to ERY, CLI, and OFX, at the same time. All isolates were susceptible to TET. One isolate resistant to ERY possessed the ermB gene with the cMLSB phenotype.
3. Molecular typing
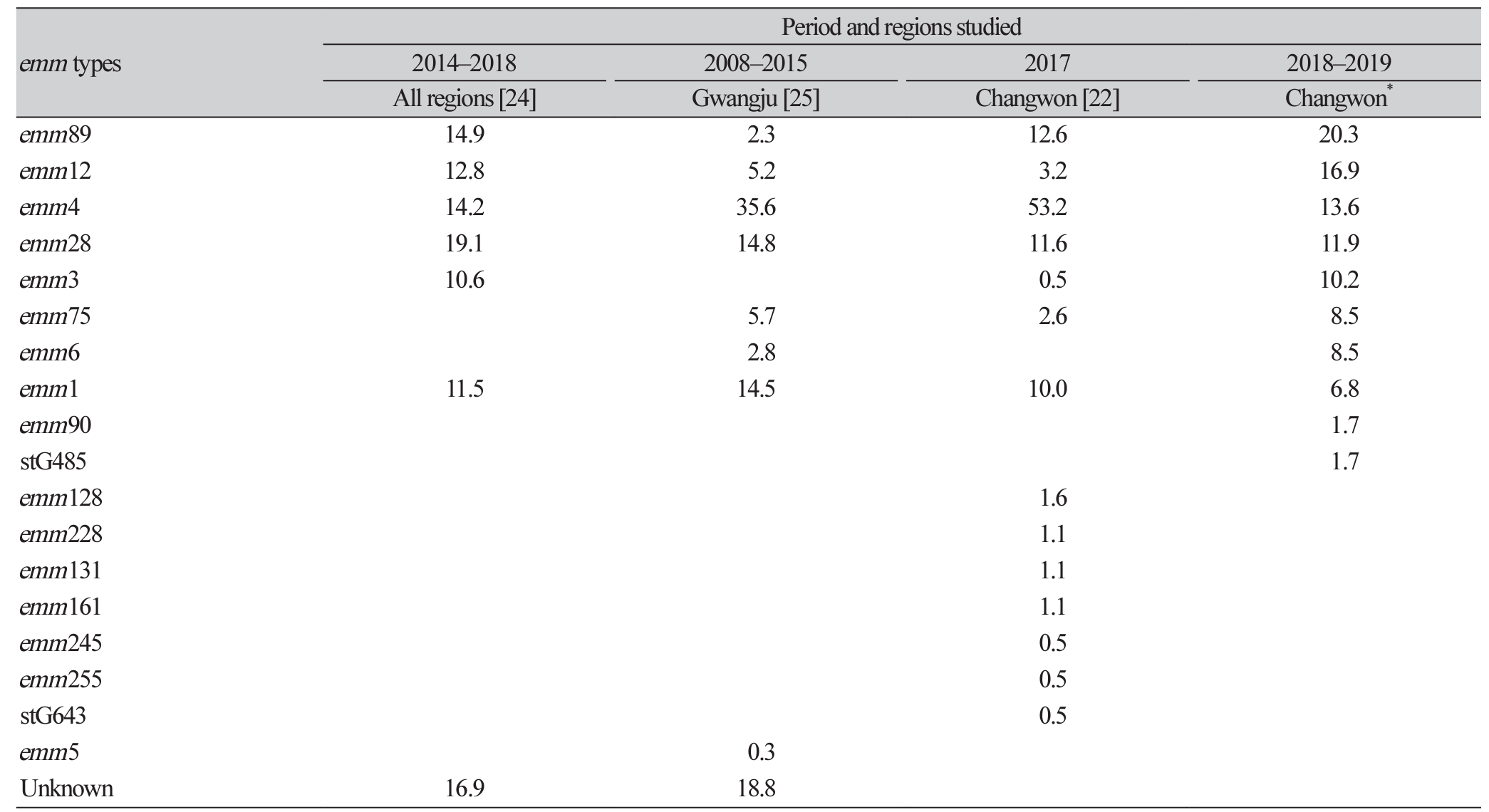
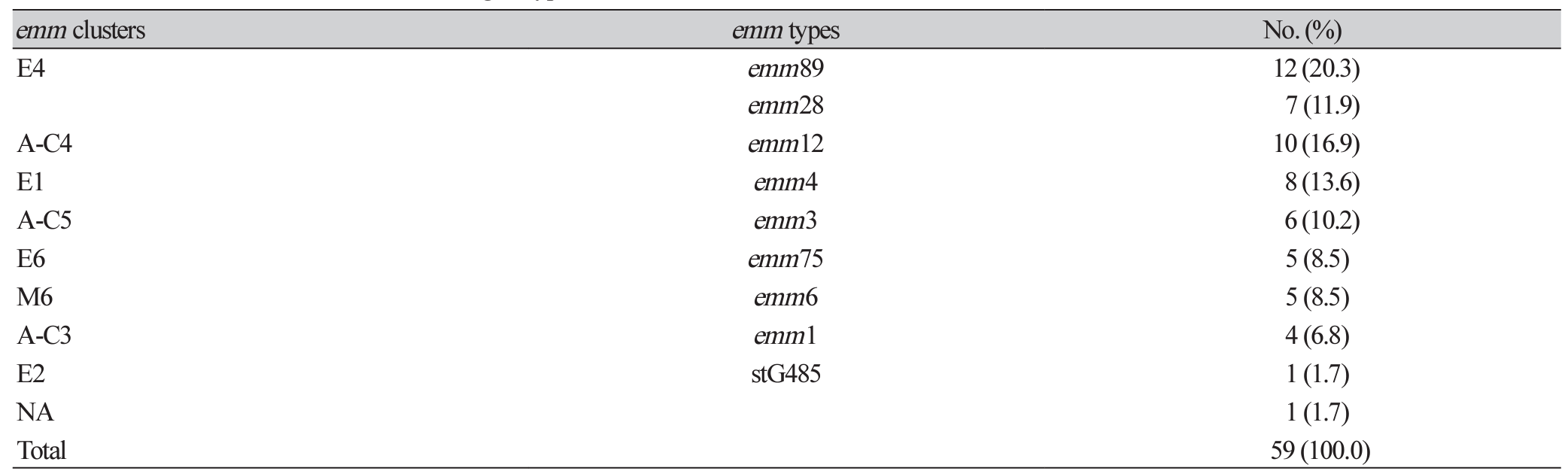
DNA was extracted for the emm genotyping of 59 GAS, successfully grown in subculture. Among the 59 isolates, the most common emm genotypes were emm89 (20.3 %), followed by emm12 (16.9 %), emm4 (13.6 %), emm28 (11.9 %), emm3 (10.2 %) and emm75/6 (8.5/8.5 %) (Table 2). The most common emm clusters were E4 (emm89/28, 32.2%), followed by A-C4 (emm12, 16.9%), E1 (emm4, 13.6%), A-C5 (emm3, 10.2%), E6 (emm75, 8.5 %) and M6 (emm6, 8.5 %). One strain (1.7 %) did not belong to any of the above clusters (Table 3).
DISCUSSION
We isolated GAS from 27.2% for patients with acute pharyngitis who visited a small-to-medium-sized pediatric clinics in Changwon in 2018-2019. In the antimicrobial susceptibility test of 59 isolates, one strain (1.7%) was resistant to each of the ERY, CLI, and OFX. That is lower resistance rate compared to 3.2% ERY, 2.6% CLI, 1.1% TET and 2.6% OFX in Changwon a year ago [21], and is much lower than 10.3% ERY, in Seoul reported in 2015 [22]. The difference in GAS resistance rate might be due to the different subjects, disease severity, antibiotic consumption and circulating strains. Judging from this low resistant rate result, ERY may be useful to treat pharyngitis at least in our region.
From the analysis of emm genotypes, emm89 (20.3%) was the most prevalent, followed by emm12 (16.9%) and emm4 (13.6%). The data collected in 2014-2018 reported by the Korea Centers for Disease Control and Prevention (KCDC), common emm genotypes were emm28 (19.1%), emm89 (14.9%), emm4 (14.2%), emm12 (12.8%), emm1 (11.5%) and emm3 (10.6%) [23]. The investigation of Jinju region nearby Changwon analyzing the emm genotype of GAS five times from 1995 to 2009 showed the change in emm types over a few decades. Previously, emm12, emm22, and emm44/61 were prevalent, but recently, emm4 and emm89 being more common [21]. By analyzing four representative papers that studied emm genotypes in Korea, temporal changes are observed [24] (Table 2). Also, the cluster shows more pronounced change, with a high level change from E1 to E4 [25,26]. Fluctuation in emm type and cluster distribution have been attributed to change of circulating emm type strains. It is known that the emm cluster A-C originated from pharyngeal samples, emm cluster D from skin samples, and emm cluster E from both pharyngeal and skin samples [12], which is in line with our results of pharyngeal strains. It is important to know the association between the emm types and the diverse GAS infections. Recently the data on the emm type distribution of population-based GAS surveillance have been proposed for the development of GAS vaccine [27].
Limitations of this study include low numbers of isolates analyzed for emm genotypes. In addition, we included only GAS isolated from pharynx, not from invasive diseases.
In conclusion, we found a continuation of very low antibiotic resistance level of GAS and a marked fluctuation of emm types even during a short period of time in Changwon.
 XML Download
XML Download