

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Pulmonary nocardiosis is the most common form of Nocardia infection, mainly affecting immunocompromised patients and those with chronic lung disease.1 While the incidence of pulmonary nocardiosis is low, it is increasing due to the growing population of immunocompromised patients (e.g., organ transplantation recipients and cancer patients) and their improved survival rates.23 Nocardiosis is characterized by a high mortality rate, with one-year mortality ranging from 15.8% to 24.5% depending on the disease type and the immune status of the patients.345 Furthermore, it increases the risk of mortality by approximately tenfold in immunocompromised patients, such as solid organ recipients.6
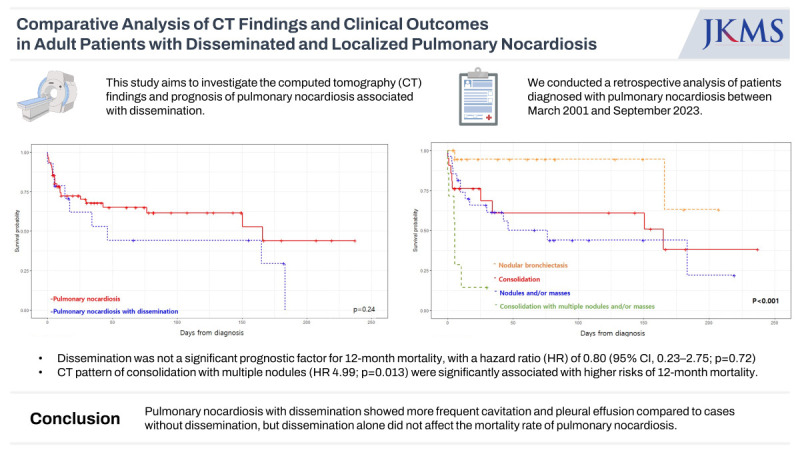
Risk factors associated with poor outcomes in nocardiosis include disseminated infection, severe immune suppression, high-dose steroids, and greater disease severity.1378 Among them, disseminated infections have been considered to be an important prognostic factor and also to have significant implications for treatment decisions, such as the selection of combination therapy and treatment duration.489 However, two recent studies have questioned whether dissemination is a direct risk factor for mortality, suggesting that infection sites and advanced infection may be more relevant than dissemination itself.35
Pulmonary nocardiosis can disseminate from the lungs to other sites, such as the brain, skin, and musculoskeletal system, through hematogenous spread.1 Chest computed tomography (CT) plays a crucial role in diagnosing and assessing the severity of pulmonary nocardiosis,10 which can show various CT findings, including lobar consolidation, solitary or multiple nodules, and peribronchial consolidation or centrilobular nodules, particularly in individuals with pre-existing structural lung disease.101112
Distinguishing the differences in CT findings between localized and disseminated pulmonary nocardiosis could provide valuable information for further evaluation and treatment decisions. Furthermore, due to its low incidence, little is known about factors associated with the prognosis of pulmonary nocardiosis, including its dissemination. Therefore, we compared chest CT findings between localized and disseminated pulmonary nocardiosis and investigated clinical and radiologic factors associated with the prognosis.
Go to : 
METHODS
Patient population
We reviewed the medical records of our hospital to identify patients with a positive Nocardia spp. culture in any type of samples gathered between June 2001 and April 2023. We also collected the records of patients with pathological results from percutaneous needle biopsy (PCNB) that indicated the presence of Nocardia and/or positive tissue cultures. Pulmonary nocardiosis was defined by the presence of clinical and/or imaging findings, along with the isolation of Nocardia spp. from cultures and/or lung biopsy. Cases with positive cultures only from sources other than respiratory samples without lung involvement were excluded from this study. Isolations from respiratory samples without any clinical or imaging evidence of active disease were categorized as colonization cases and were subsequently excluded. We also excluded patients who did not undergo a chest CT within 2 weeks after the diagnosis of pulmonary nocardiosis.
The following patient characteristics were collected: demographics, diagnosis information, underlying chronic pulmonary diseases (e.g., bronchiectasis, chronic obstructive pulmonary disease, and interstitial lung disease), immunocompromised status, presence of graft-versus-host disease, presence of neutropenia or lymphopenia, identified Nocardia spp., presence of coinfection, site of dissemination, treatment information, and clinical outcomes, specifically the overall 12-month mortality rate from the initial diagnosis of pulmonary nocardiosis.
Definitions
Disseminated pulmonary nocardiosis was defined as the simultaneous involvement of the lungs and a non-contiguous organ, or lung involvement with positive blood cultures. Immunocompromised patients were defined as individuals who had undergone solid organ transplantation, hematopoietic stem cell transplantation, those who had a malignancy and received chemotherapy or radiation therapy within the past 6 months, autoimmune diseases, those who were taking daily corticosteroids (at least 5 mg/day of prednisone or an equivalent drug), and individuals who tested positive for human immunodeficiency virus (HIV) infection.413 Coinfection was defined as the detection of other respiratory pathogens within 15 days before or after the nocardiosis infection. Neutropenia was defined as an absolute neutrophil count < 1,000/mL, and lymphopenia was defined as an absolute lymphocyte count < 500/mL.1415
Chest CT review
CT findings were reviewed in consensus by two chest radiologists, LHN and KEY, who have 9 and 11 years of experience in chest imaging, respectively. Parenchymal abnormalities were assessed for the presence of consolidation, nodules or masses, cavities, centrilobular nodules, and ground glass opacity. Pleural effusion and lymph node enlargement in the thorax were also evaluated. All glossary terms were defined according to the Fleishner Society.16 Then, we categorized the CT findings into the following groups: 1) consolidation, 2) solitary or multiple nodules and/or masses, 3) consolidation with multiple nodules (and/or masses), 4) peribronchial consolidation and/or centrilobular nodules in patients with underlying chronic lung disease such as bronchiectasis (nodular bronchiectasis or bronchopneumonia pattern). This categorization was done based on the dominant CT findings (Fig. 1). When it was not possible to determine the dominant CT findings between consolidation and nodules, we defined it as consolidation with multiple nodules. The total extent of pneumonia was assessed by assigning scores on a scale of 0–5 for each of the five lung lobes: 0 = no involvement; 1 = less than 5%; 2 = 5% to less than 25%; 3 = 25% to less than 50%; 4 = 50% to less than 75%; and 5 = more than 75%. The total CT score was determined as the sum of the individual scores and ranged from 0 to 25.17
 | Fig. 1Four representative patterns of pulmonary nocardiosis. (A) Consolidation: CT scan of a 51-year-old woman with underlying breast cancer. Segmental consolidation with internal necrotic change is evident in the right lower lobe. (B) Nodules and/or masses: CT scan of a 75-year-old woman with a post-transplantation state of the liver. Two large cavitary masses are evident in both upper lobes and several nodules in the right lung. (C) Consolidation with multiple nodules: CT scan of a 68-year-old man taking steroid medication. Segmental consolidation is shown in the right lower lobe and several nodules are noted in the right middle lobe and both lower lobes (arrows). (D) Nodular bronchiectasis: CT scan of a 47-year-old woman with a nodular bronchiectasis pattern. Multiple centrilobular nodules and bronchiectasis are noted in the right middle lobe and both lower lobes.CT = computed tomography.
|
Statistical analysis
The baseline characteristics and CT image findings were compared between the localized and disseminated groups of pulmonary nocardiosis using Fisher’s exact or χ2 test for categorical variables and Student's t-test for continuous variables. The Kaplan-Meier survival curves were plotted for the localized and disseminated groups of pulmonary nocardiosis, as well as for the CT category, and compared using the log-rank test. Univariate and multivariate analyses were performed using Cox regression to evaluate the association between variants and the 12-month overall survival outcomes. All variables with P values less than 0.05 in the univariate analysis were included in the multivariate analysis. The odds ratios and 95% confidence intervals (CIs) were then calculated based on the results. P values less than 0.05 were considered significant. All statistical calculations were performed using STATA (version 9.4; SAS Institute, Cary, NC, USA) and R (version 4.2.2; The R Foundation for Statistical Computing, Vienna, Austria).
Ethics statement
This retrospective study was reviewed and approved by the Institutional Review Board of Seoul Asan Medical Center (approval number: 2023-0653). Informed consent was waived due to the retrospective nature of the study.
Go to :
RESULTS
Patient characteristics
We initially identified 120 patients with positive Nocardia cultures in specimens or pathological results of Nocardia from PCNB. Among them, 25 patients exhibited positive cultures from sources other than respiratory samples, but did not demonstrate any signs of lung involvement. Six patients were categorized as colonization cases. Subsequently, 14 patients who did not undergo chest CT within 2 weeks after the diagnosis of nocardiosis were excluded. Finally, 75 patients were included in this study (Fig. 2). The average age was 61.2 ± 13.8 years, and 57 patients (76.0%) were male. Out of the total number of cases, 37 (49.3%) individuals had an immunocompromised state, including 10 (13.3%) with solid organ transplantations, 6 (8.0%) with hematopoietic cell transplantations, 4 (5.3%) with malignancy that were treated with chemotherapy or radiotherapy within the past 6 months, 5 (6.7%) with autoimmune disease, 12 (16.0%) with steroid use, and 1 (1.3%) with HIV infection (Table 1). Out of 10 patients who underwent solid organ transplantations, 7 (70.0%) developed Nocardia infection more than 6 months after transplantation. Among 6 patients who underwent hematopoietic cell transplantation, 4 (66.7%) had Nocardia infection during the late post-engraftment period. Among these, 4 out of 6 patients had graft-versus-host disease.
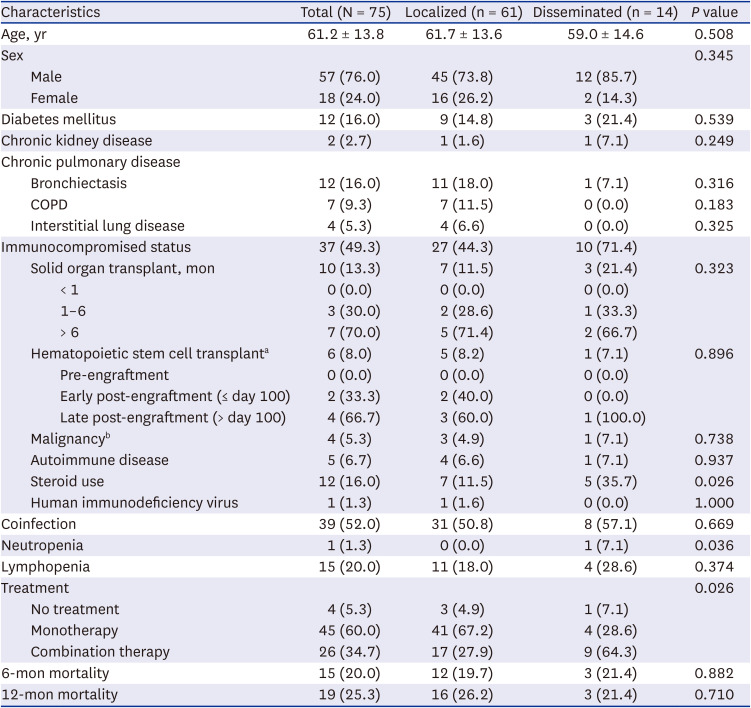

Table 1
Clinical characteristics of subjected patients
Values are presented as number (%) or mean ± standard deviation.
COPD = chronic obstructive pulmonary disease.
aFour of 6 patients had graft-versus-host disease.
bPatients who had a malignancy and received chemotherapy or radiation therapy within the past 6 months.
![]()
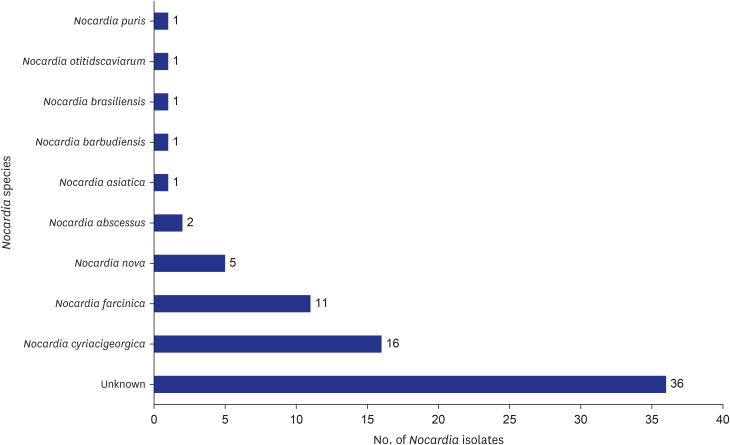
Positive cultures of Nocardia spp. were detected in various respiratory specimens: sputum specimens in 38 patients (50.7%), bronchoalveolar lavage in 17 patients (22.7%), and pleural fluid in 1 patient (1.3%). Among the 20 patients (26.7%) diagnosed through PCNB only, positive tissue culture was obtained in 8 patients, organisms were seen on histologic stains in 9 patients, and both identification of organisms and positive tissue cultures were found in 3 patients. The most common Nocardia species isolated were Nocardia cyriacigeorgica (n = 16) and Nocardia farcinica (n = 11). Thirty-six isolates’ species were unidentified (Fig. 3).
Fourteen patients (18.7%) were found to have disseminated pulmonary nocardiosis. Among these cases, the brain was the most common site of dissemination in 9 patients (64.3%), followed by musculoskeletal involvement in 3 patients (21.4%), and positive blood culture in 3 patients (21.4%). One of the patients with disseminated infection showed involvement in multiple organs, including the lungs, brain, and skin with positive blood culture.
Coinfection was identified in 39 patients (52.0%), with nontuberculous mycobacteria (NTM) detected in 10 patients (13.3%), bacterial infection in 17 patients (22.7%), fungal infection in 12 patients (16.0%), and viral infection in 11 patients (14.7%).
Chest CT findings and comparison between localized and disseminated nocardiosis
The most common CT findings were nodules (66.7%), followed by consolidation (56.0%) and cavitation (38.7%). Mediastinal lymph node enlargement was found in 13 out of 75 patients (17.3%). The most common CT pattern was solitary or multiple nodules and/or masses (36.0%), followed by consolidation (28.0%), nodular bronchiectasis (26.7%), and consolidation with multiple nodules (9.3%) (Table 2).
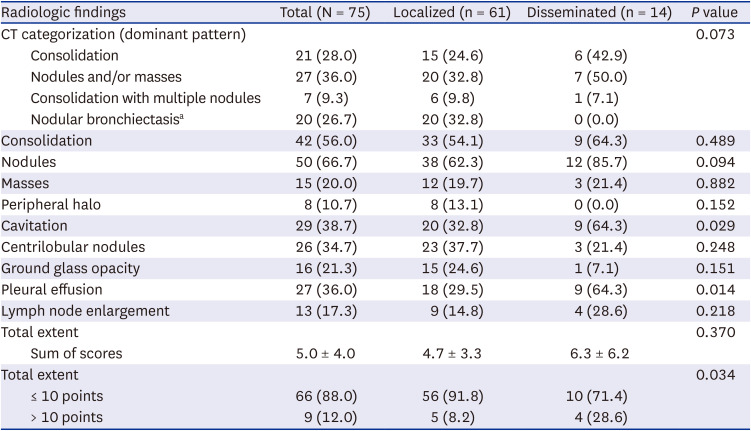
Table 2
Radiologic findings of patients with nocardiosis
Values are number (%) or mean ± standard deviation.
CT = computed tomography.
aThree of 20 patients had co-infection with nontuberculous mycobacteria.
![]()
When comparing CT findings between localized and disseminated infections, pulmonary nocardiosis with dissemination showed a higher frequency of cavitation (disseminated, 64.3% vs. localized, 32.8%, P = 0.029) and pleural effusion (disseminated, 64.3% vs. localized, 29.5%, P = 0.014). When divided into two groups based on a total extent score of 10, disseminated pulmonary nocardiosis showed a higher frequency of cases with a total extent score greater than 10 (disseminated, 28.6% vs. localized, 8.2%, P = 0.034); in contrast, the total extent scores were not significantly different between the two groups (disseminated, 6.3 ± 6.2 vs. localized, 4.7 ± 3.3, P = 0.370). Other image findings were not significantly different between the two groups.
Survival analysis
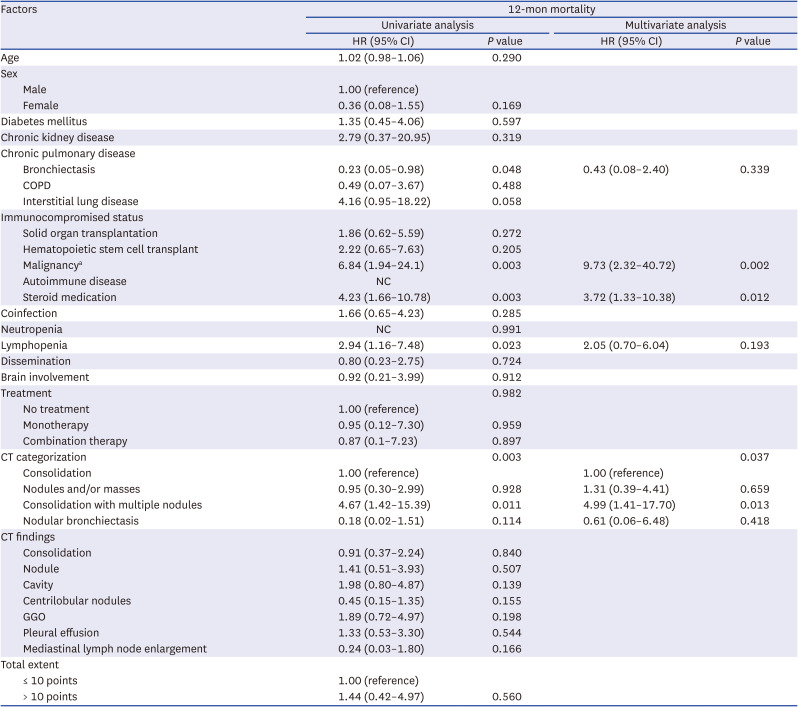
In total, 19 patients (25.3%) died within 12-month of diagnosis. The 12-month mortality rates were 21.4% (3/14) for pulmonary nocardiosis with dissemination and 22.2% (2/9) for pulmonary nocardiosis with brain involvement. The median time to death was 3.71 months (interquartile range [IQR], 1.05–5.54). Of the remaining 56 patients, 46 completed the 12-month follow-up and 10 patients were followed up for a median duration of 6.70 months (IQR, 5.24–9.30). Kaplan-Meier curves of survival are shown in Fig. 4. There was no significant difference in mortality between localized and disseminated pulmonary nocardiosis (P = 0.240, log-rank test). The presence of consolidation and multiple nodules and/or masses were found to be significantly associated with worse survival compared to the other CT categories (P < 0.001, log-rank test). Table 3 presents the factors associated with 12-month survival as determined by Cox regression analysis. In the univariate analysis, malignancy, steroid use, lymphopenia, and CT pattern of consolidation with multiple nodules were significantly associated with 12-month mortality, while disseminated infection did not show a significant association (hazard ratio [HR], 0.80; 95% CI, 0.23–2.75; P = 0.724). In multivariate analysis, malignancy (HR, 9.73; 95% CI, 2.32–40.72; P = 0.002), steroid use (HR, 3.72; 95% CI, 1.33–10.38; P = 0.012), and CT pattern of consolidation with nodules/masses (HR, 4.99; 95% CI, 1.41–17.70; P = 0.013) were identified as risk factors associated with 12-month mortality.
 | Fig. 4Kaplan-Meier curves for overall survival. (A) Overall survival according to localized and disseminated pulmonary nocardiosis. (B) Overall survival according to computed tomography pattern.
|
Table 3
Univariable and multivariable Cox regression analysis of 12-month mortality after diagnosis of pulmonary nocardiosis
HR = hazard ratio, CI = confidential interval, COPD = chronic obstructive pulmonary disease, GGO = ground glass opacity, NC = not calculated.
aPatients who had a malignancy and received chemotherapy or radiation therapy within the past 6 months.
![]()
Go to :
DISCUSSION
In this study, we compared CT findings between localized and disseminated pulmonary nocardiosis and identified the clinical and radiologic prognostic factors, including dissemination. We observed that the presence of a cavity and pleural effusion was associated with disseminated pulmonary nocardiosis. While dissemination itself was not associated with mortality for pulmonary nocardiosis. Patients with underlying malignancy and those taking steroid medication exhibited higher mortality rates. Additionally, CT findings of consolidation with multiple nodules were also associated with a poor outcome.
Previous studies have compared the clinical outcomes of localized and disseminated nocardiosis, and reported that disseminated infections have a worse prognosis compared to localized infection; however, these studies included various sites of Nocardia infection, including the skin, soft tissue, eyes, and as well as the lungs.418 Primary cutaneous infection of nocardiosis typically has a better outcome,119 while lung infection has a high mortality rate ranging from 16% to 25%, regardless of dissemination.20212223 Therefore, when considering the prognosis of pulmonary nocardiosis, it appears that the severity of the infection itself is more critical than its dissemination status. Our findings are consistent with another study, which stated that advanced infection, rather than dissemination alone, was a risk factor associated with worse 1-year mortality.23
The presence of cavitation has been associated with higher mortality in other studies,32021 but not in the present study. We thought that cavitation could serve as an indicator of the severity of the infection, such as disseminated infection, but it did not necessarily correlate with higher mortality. This discrepancy may be attributed to variations in the site of infection and the characteristics of the patients. Furthermore, it could be due to the improved control of pulmonary nocardiosis with cavitation, thanks to advances in medical care.
Whereas the presence of both consolidation and multiple nodules on CT scans was associated with a worse prognosis. This combination of findings likely indicates advanced pulmonary nocardiosis infection, with spread from one lung to another and increased disease involvement. In cases that exhibit both consolidation and multiple nodules, it is advisable to consider more aggressive treatment such as combination therapy and an extended treatment duration.124
Patients with underlying structural diseases such as bronchiectasis can show subacute manifestations of pulmonary nocardiosis. A few studies have reported that a nodular bronchiectatic pattern can be observed on chest CT scans, resembling NTM.2526 Although there are some cases of co-infection with NTM, it is worth noting that the nodular bronchiectatic pattern in pulmonary nocardiosis can occur independently of NTM co-infection, which can be resolved with medication specifically targeting nocardiosis. It suggests that this condition may not be solely attributed to NTM infection. In our study, some of the patients with a nodular bronchiectasis pattern may have represented subacute pulmonary nocardiosis, and only 3 of the 20 patients had co-infection with NTM. Further studies with larger sample sizes are needed for the diagnosis and treatment of subacute pulmonary nocardiosis.
PCNB in patients with a high suspicion of infection can occasionally provide useful information that can lead to significant changes in patient management.27 The role of PCNB was particularly critical in the diagnosis of pulmonary nocardiosis in this study. Patients diagnosed solely with PCNB accounted for as much as 26.7% (20/75) of the total patients. A previous study reported that 44% of cases of pulmonary nocardiosis required an invasive procedure for diagnosis in order to obtain adequate specimens.28 Pulmonary nocardiosis is often initially misdiagnosed as TB or cancer based on CT findings. Once pulmonary nocardiosis is diagnosed, specific antimicrobial therapy, such as trimethoprim-sulfamethoxazole, can be initiated,29 and additional procedures, such as a brain MRI, are often performed to confirm dissemination.30 Therefore, if an imaging finding indicates possible pulmonary nocardiosis without evidence of a positive culture, PCNB may be helpful for diagnosis and treatment.
Immunocompromised state is associated with higher mortality rate in patients with nocardiosis.1 Patients with malignancy have a mortality rate greater than 60%.31 In our study, three of four patients with underlying malignancy died within 12 months. Among them, two patients died due to nocardiosis, while one experienced mortality attributed to cancer aggravation. Our data set has limitations when it comes to interpreting mortality in the cancer population, as we analyzed all-cause mortality in a small sample. Therefore, further study is needed to examine whether pulmonary Nocardia infection affected mortality in cancer patients.
There are several limitations to this study. First, it was a retrospective study with a relatively small sample size. Second, patients received different management such as combination therapy or not, possibly based on disease severity, which may have influenced the clinical outcome. Third, not all patients had brain imaging, which may have resulted in an underdiagnosis of disseminated infection. Lastly, we analyzed all-cause mortality, which may include patients who died from other causes.
In conclusion, this study revealed that pulmonary nocardiosis with dissemination often showed more frequent cavitation and pleural effusion compared to cases without dissemination. However, dissemination alone did not affect the mortality rate of pulmonary nocardiosis. Instead, patients with underlying malignancy, steroid use, and CT findings of consolidation with multiple nodules were associated with a worse prognosis of pulmonary nocardiosis. Therefore, this study emphasizes the importance of considering these factors when managing pulmonary nocardiosis.
Go to :
 XML Download
XML Download