

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Infertility is defined as a failure to achieve a clinical pregnancy after 12 months or more with regular unprotected sexual intercourse,1 and the World Health Organization has identified infertility as a significant global health problem with an increasing prevalence. The prevalence of infertility was estimated at 13.5% in the Korean population,2 but the prevalence varies among countries.3
Infertility is divided into primary and secondary infertility on the basis of the presence or absence of a previous pregnancy. Male infertility may be caused by abnormal sperm function or blockages, which prevent the delivery of sperm and lead to low sperm production.4 The common causes of female infertility are anovulation, endometriosis, uterine abnormalities, obstructed fallopian tubes, and pelvic adhesions.5 In addition, there is a wide range of risk factors of infertility, from maternal health and lifestyle, to reproductive history.6 Other non-modifiable risk factors influencing infertility include age and genetic factors.7
A wide range of risk factors may be associated with infertility; however, these factors may differ among countries or ethnicities. For example, a nationwide representative survey in 2014 revealed that the prevalence of overweight/obesity was 45.3% in Korea, while it was over 60% in the U.S.8 Therefore, the association between risk factors and infertility should be investigated in diverse ethnic groups, but this association has not been well documented in the Korean population.
We aimed to investigate the association of risk factors such as body mass index (BMI), smoking status, alcohol consumption, hypertension, diabetes, and thyroid disease, with infertility in the Korean female population through a cross-sectional survey of infertile women and a nationwide survey of fertile controls. Additionally, in this study, we analyzed risk factors according to primary and secondary infertility.
Go to : 
METHODS
Study participants
A total of 986 infertility female patients were recruited from the 6 major hospitals located in Seoul and its suburban area in Korea from April to December 2014. These centers accounted for over 20% of in vitro fertilization (IVF) in Korea. The infertile study participants were 20–45 years old and could not conceive after 12 months or more with regular unprotected sexual intercourse.
For comparison, fertile controls were selected from two nationally representative cohorts. First, the information on fertile women aged 20–46 years was obtained from the 2009 & 2012 National Survey on Fertility, Korea Institute for Health and Social Affairs (KIHASA) in Korea. This national survey has been operated by KIHASA every three years since the early 1970s. Second, we gathered information on fertile women through the 2008–2012 Korean Genome and Epidemiology Study (KoGES), conducted by the National Institute of Health in Korea. As part of the KoGES Consortium, our study specifically incorporated the KoGES health examinee (HEXA) data, focusing on participants residing in metropolitan areas aged 35–46 years. We matched each case with controls based on age (± 3 years). The ratio of cases to controls was 1:4 in KIHASA, and 1:3 in KoGES, respectively. Finally, we matched 986 cases and 3,944 controls from the 2009 & 2012 KIHASA and matched 517 cases and 1,551 controls from 2008–2012 KoGES-HEXA (Fig. 1).

Women’s fertility history
The fertility of women aged 20–46 was assessed through the question “Have you ever attempted to become pregnant?” Women who responded “Yes” were considered fertile women. In this study, women who had experienced pregnancy were used as the control group in both KIHASA and KoGES-HEXA. Women who were unmarried, divorced, or widowed based on the question about marital status were excluded from the control group study population.
Data sources
The infertile participants were asked to complete the questionnaire, and it took about 10 minutes to complete the instruments. Demographic information, including age and education level, was obtained from all participants through the questionnaire. Reproductive history, including the history of abortion and the number of deliveries, was based on self-report. Primary infertility was defined if a woman who has never conceived, and secondary infertility was determined if a woman experienced at least one episode of conception previously.
Smoking behavior, alcohol consumption, and disease history were obtained by self-report. Smoking status was categorized into three groups: never-smokers, former smokers, and current smokers. Never-smokers were defined as participants who had not smoked or < 100 cigarettes in their lifetime. Former smokers had smoked ≥ 100 cigarettes but did not smoke at the time of the interview. Current smokers were participants who had smoked ≥ 100 cigarettes and smoked at the time of the interview. Participants were also requested to provide information on whether someone smoked at home or in the workplace in the past year. Alcohol intake was classified as non-drinker and drinker. Respondents who drank at least 1 alcoholic drink a month was defined as a drinker. Drinkers were further categorized into “light drinkers” ≤ 4 glasses, “moderate drinkers” 5–6 glasses, and “heavy drinkers” ≥ 7 glasses at a time. Regarding chronic disease status, whether they had hypertension, diabetes mellitus, or thyroid disease was asked.
The information from KIHASA included BMI, and education level, whereas the questionnaire of KoGES-HEXA included questions regarding smoking behavior, alcohol consumption, and disease history.
Statistical analysis
To compare the baseline characteristics of infertile women and matched fertile controls, we conducted the chi-square test for categorical variables and paired t-test for continuous variables. To estimate the odds ratios (ORs) and 95% confidence intervals (95% CIs) of infertility, we used multivariate conditional logistic regression adjusting for BMI, education level, and occupation. Multiple regression imputation was performed for missing values of BMI.9 We also assessed the collinearity between independent variables using the variance inflation factor and Pearson’s correlation coefficient.
All statistical analyses were performed using SAS version 9.4 (SAS Institute Inc., Cary, NC, USA).
Ethics statement
All participants provided written informed consent to participate, and the study protocols were approved by the Institutional Review Board (IRB) of Seoul National University Hospital (IRB No. H-1408-018-601).
Go to :
RESULTS
The general characteristics of the participants are presented in Table 1. There was no significant age difference observed between the Infertility and Non-infertility groups in both KIHASA and KoGES-HEXA. Regarding body measurements (height, weight, BMI), significant differences were found between the Infertility and Non-infertility groups in KIHASA. On the other hand, in KoGES-HEXA, there was a significant difference in height between the infertility and non-infertility groups, but there were no significant differences in BMI and weight between the groups. Additionally, clinical and lifestyle factors such as cigarette smoking, alcohol consumption, hypertension, diabetes, and thyroid disease showed significant differences between the two groups in KoGES-HEXA.

Table 1
Baseline characteristics of the study population
Data are shown as mean ± standard deviation or number (%).
BMI = body mass index, KIHASA = Korea Institute for Health and Social Affairs, KoGES-HEXA = Korean Genome and Epidemiology-health examinee.
aFertile matched control was selected from women aged 20–46 who participated in the National Survey on Fertility and Family Health and Welfare in 2009 and 2012, in the KIHASA.
bFertile matched control was selected from women aged 35–46 who participated in KoGES-HEXA data in the Korea Disease Control and Prevention Agency.
cThe KIHASA data did not include information on smoking, alcohol consumption, hypertension, diabetes, and thyroid disease.
dStatistically significant (P < 0.05) for group difference between cases and controls using t-test for continuous variables and χ2 or Fisher’s exact test for categorical variables.
![]()
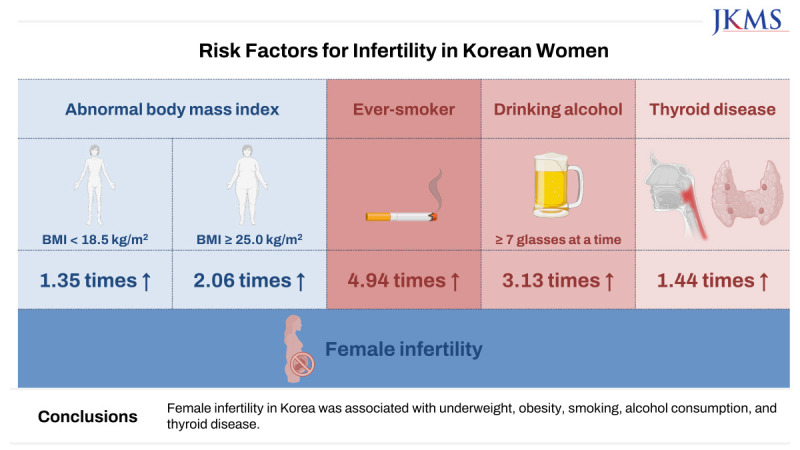
Women with BMI < 18.5 kg/m2 had 1.35 times higher OR for infertility (95% CI, 1.03–1.77), and women with BMI ≥ 25.0 kg/m2 also showed 2.06 times higher OR for infertility (95% CI, 1.61–2.64) compared to women with normal BMI (Table 2). In subgroup analyses according to the previous history of the conception, the OR for infertility was still significantly higher in women with BMI ≥ 25.0 kg/m2 compared to women with normal BMI (OR, 2.26; 95% CI, 1.70–3.01 in women with primary infertility and OR, 1.77; 95% CI, 1.22–2.58 in women with secondary infertility, respectively).

Table 2
Association between BMI and infertility in women aged 20–46 years
BMI = body mass index, OR = odds ratio, CI = confidence interval.
aFertile matched control was selected from women aged 20–46 who participated in the National Survey on Fertility and Family Health and Welfare in 2009 & 2012 in the Korea Institute for Health and Social Affairs.
bOR was calculated using stratified age group, and adjusted for education in conditional logistic regression model.
![]()
In Table 3, the association of infertility with smoking, alcohol, and current chronic diseases was demonstrated. Ever-smokers showed 4.94 times higher odds for infertility compared to never-smokers (95% CI, 3.45–8.85), and this association was not substantially changed in subgroup analysis according to the previous history of conception. In addition, secondhand smoking showed a significantly higher association with infertility (OR, 26.53; 95% CI, 18.53–37.19 in women who reported secondhand smoke exposure in the workplace and OR, 1.67; 95% CI, 1.17–2.14 in women who reported secondhand smoke exposure at home).
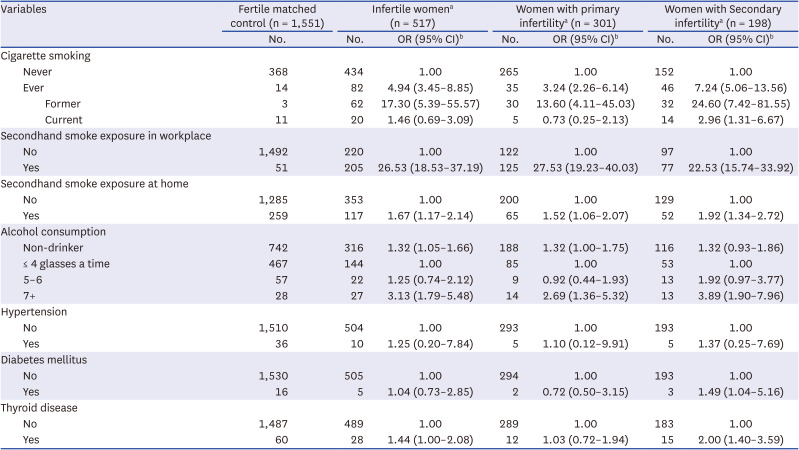
Table 3
Association between smoking, alcohol consumption, and chronic diseases and infertility in women aged 35–46 years
OR = odds ratio, CI = confidence interval.
aFertile matched control was selected from women aged 35–46 who the Korean Genome and Epidemiology-health examinee study in the Korea Disease Control and Prevention Agency.
bOR was calculated using stratified age group, and adjusted for education, and BMI in conditional logistic regression model.
![]()
Regarding alcohol consumption, women drinking ≥ 7 glasses at a time demonstrated 3.13 times significantly higher odds of being infertile than women drinking ≤ 4 glasses at a time (95% CI, 1.79–5.48). Furthermore, the association was not different according to the previous conception history.
Among current chronic diseases, only thyroid disease was found to be associated with infertility. Women with thyroid disease demonstrated 1.44 times higher odds for being infertile compared to women without thyroid disease (95% CI, 1.00–2.08), and this association was significant in women with secondary infertility (OR, 2.00; 95% CI, 1.40–3.59).
Go to :
DISCUSSION
The present study included about a thousand infertile women who visited large fertility centers in Korea. We found that infertile women were more likely to be underweight, obese, ever-smokers, high-risk alcohol users, or have thyroid diseases after matching and adjustment for covariates. To our knowledge, this is the largest study conducted in Korea to investigate the association of risk factors with infertility compared with nationally representative cohorts.
In the present study, BMI demonstrated a bidirectional relationship with infertility, which means that underweight women (BMI < 18.5 kg/m2) and obese women (BMI ≥ 25.0 kg/m2) had a higher OR for infertility compared to women with normal BMI. This finding is in accordance with the study by Hassan and Killick,10 which reported that both underweight and obese women have a longer time to pregnancy than women with normal BMI. A previous study reported that women with a BMI of 20–21.9 kg/m2 have a 1.3-fold increased relative risk of infertility, and those with a BMI of 30 kg/m2or higher have an increased risk of up to 3.7-fold compared to those with a BMI of 24–25.9 kg/m2.11 Another European population study showed that underweight or obese women need a long time to become pregnant, especially if they are smokers.12
A study of all IVF clinics in the Netherlands showed a 33% reduction in the success pregnancy rate of the first cycle for women with a BMI of 27 kg/m2 or higher,13 and a Norwegian study found that women with a BMI of 30 kg/m2 or higher who received IVF or intracytoplasmic sperm injection three times had a lower cumulative pregnancy rate of 41.4% compared to women with normal BMI due to spontaneous abortion.14
BMI can influence infertility. Deviations in a woman's weight or body fat beyond a certain range can impact reproductive function.15 According to a study in the United States, female college graduates were found to have, on average, 20% fewer children than high school graduates.16 Additionally, recent research suggests that higher education levels are associated with a higher rate of experiencing infertility treatments.17 There is a gradual increase in the utilization of infertility treatments as educational levels rise. This is why educational level is considered a significant confounding variable in the association between infertility and BMI, and further research on this topic is warranted.
The bidirectional relationship of infertility according to BMI might be ovulatory dysfunction in underweight women and obese women. Excessive leanness may lead to hypothalamic dysfunction followed by anovulatory menstrual cycles,1819 whereas obesity may cause anovulation by insulin resistance and subsequent increase of androgen.2021 Indeed, in a prospective cohort study including 116,671 women, the estimated relative risk of ovulatory infertility showed a U-shaped association according to BMI.22 Therefore, maintenance of optimal BMI may be helpful for the enhancement of fecundity.
Several previous studies reported the adverse impact of smoking on female fecundity.2324 In our study, similar findings were observed. Ever-smokers showed 4.94 times higher odds for infertility than never-smokers, and the results were not substantially changed when stratified into women with primary and secondary infertility.
A previous study reported that women undergoing IVF who are also smokers had a 34% reduction in the chances of pregnancy as compared to the non-smokers, and smokers required twice as many IVF procedures to become pregnant.25 It has also been reported that smokers have a 28% live birth rate and passive smokers have a halved pregnancy rate. Smoking has been reported to have adverse effects on male fertility. It can affect the sperm count, motility, and shape and alter the concentration of luteinizing hormone, and toxic cotinine and cadmium can be detected in follicular fluid.2426
A previous study found that menopause can occur one to four years earlier in smokers,27 and recent studies have shown that the thickness of the zona pellucida may increase, making sperm penetration difficult.28
In subgroup analyses, significantly higher odds for infertility were observed only in former smokers, not current smokers. This finding may be explained in part by smoking duration, although the information on smoking duration was not available in our study. In a prospective cohort in Denmark, only a smoking duration of ≥ 10 years among current smokers has a negative impact on fecundability,29 although decreased fecundability does not always mean infertility. Furthermore, in our study, the number of former smokers in fertile matched control was quite small (n = 3), and the wide CI suggests that this finding is likely to have arisen by chance.
Regarding secondhand smoking, secondhand smoking exposure in the workplace or at home demonstrated an equally strong association with infertility regardless of subgroup analyses of primary and secondary infertility. However, previous studies investigating the association between passive smoking and fertility have yielded inconsistent results. In one study, women exposed to secondhand smoking were associated with decreased fecundability within 6 months,30 whereas other studies did not find any significant relationship between passive smoking and fecundability.2931 The discrepancy between our study and other studies may be due to different study designs, i.e., cohort study and cross-sectional study. Furthermore, short-term fecundability was defined as a study outcome in previous studies, while infertility was used in our study, and mean duration of time to diagnosis of infertility was one and a half years.
Alcohol affects steroidogenesis, especially increases estrogen levels, and has been reported to be associated with irregular menstrual cycles or ovulatory dysfunction.32 In the present study, we found a U-shaped relationship between alcohol consumption and infertility, with increased risks in the non-drinker and the higher intake groups. Similarly, Juhl et al.33 reported a non-linear J-shaped association between drinking and waiting time to pregnancy; however, this association was only observed in spirits drinking in their study. In contrast, any significant effect on fertility was not demonstrated as less than 14 servings of alcohol per week.34 In addition, alcohol consumption was not associated with ovulatory infertility.35 These controversies regarding the effect of alcohol consumption on female fertility may be due to non-standardized assessment of alcohol consumption, such as heterogenous classification, different study designs, and different proxies of alcohol exposures. Despite these discrepancies about fertility or time to pregnancy, previous studies have reported a negative impact of alcohol consumption on the outcomes of assisted reproduction technologies (ART).3637
The changes in lifestyle can influence the association with infertility. In the case of Korea, risk factors such as Westernized dietary habits and increasing maternal health are investigated for their impact on infertility.38 Particularly, infertility is recognized as a direct medical cause of low birth rates, leading Korea to have the lowest fertility rate among Organisation for Economic Co-operation and Development countries.39 In Western countries, Westernized dietary habits, stress, and environmental pollution have been reported to affect reproductive function.40 Lifestyle changes, including alcohol consumption and smoking status may exert intricate effects, potentially contributing to the increasing prevalence of infertility. Understanding these factors is crucial for developing preventive and therapeutic strategies.
Our study showed increased odds of infertility, especially secondary infertility, in women with thyroid disease. A previous study reported that thyroid abnormalities affect sex steroids and that women may suffer from difficulties in pregnancy due to amenorrhea and irregular menstruation.41 Another study also found that one in five women with spontaneous abortion or infertility experience had subclinical hypothyroidism.42 It has been suggested that high TSH levels may affect fertility, even within the normal range, and lowering TSH levels might help women with infertility. However, in our study, detailed information about thyroid disease, i.e., hyperthyroidism and hypothyroidism, was unavailable.
Several limitations should be considered in the present study. First, women with and without infertility were recruited from different populations with discordant characteristics such as demographics and social status. For example, infertile women were recruited from institutions in metropolitan areas. However, fertility clinics are not present in rural areas in Korea, and patients from all over the country visit fertility clinics in urban areas, although study participants do not represent the general population. Second, information on risk factors was collected by self-reported questionnaires both in infertile women and fertile matched control; therefore, recall bias may be suspected. Furthermore, women might have underestimated their smoking or alcohol consumption due to social stigmatization. Third, only female risk factors were available through questionnaires. Because infertility can be classified as male and female infertility, information about male partners can provide another insight into the association between risk factors and infertility. Fourth, the women in the KoGES-HEXA control group are limited to individuals aged 35 to 46. Consequently, the investigation on alcohol consumption, smoking, and other factors presented in Table 3 could not encompass the age group of 25 to 34. Considering this limitation, it is recommended to interpret the results with caution. Fifth, in this study, although we matched for age, we were unable to match for various other risk factors for infertility (e.g., age at first marriage or working status). However, we adjusted for education level and BMI as confounding factors.
Sixth, our result should be interpreted with caution as a case-control study design, and the association of risk factors and infertility does not mean a causal relationship. Finally, infertile women included women who were preparing for their first attempt at ART and women who had already experienced previous ART cycles. In addition, fertile matched controls may have included women who had their offspring through ART practice.
In spite of the limitations mentioned above, there are several strengths of this study. The present study is the largest study including infertile Korean women. Furthermore, infertility was diagnosed and documented by experts in this field. Regarding fertile matched control, they were recruited from nationally representative surveys, i.e., KIHASA and KoGES-HEXA. These complex surveys have proven for accuracy and representativeness,4344 and research findings can be found elsewhere.4546 Finally, we performed conditional logistic regression to adjust for age, the most important confounding for ovarian reserve.
In conclusion, our study reveals associations between female infertility and factors such as being underweight, obesity, smoking (including secondhand smoke), alcohol consumption, and thyroid diseases. The study results are expected to be particularly helpful in regulating and preventing modifiable risk factors as potential causes of infertility. Furthermore, understanding the association between risk factors and infertility enables healthcare professionals to provide personalized health monitoring for infertility patients. Lastly, infertility poses not only individual and couple-related challenges but also societal and economic burdens. The findings from this study could enhance the understanding of infertility among policymakers and elevate national attention to infertility prevention.
Go to :
 XML Download
XML Download