

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Several randomized controlled trials have demonstrated that transradial access (TRA), compared to transfemoral access (TFA), offers similar procedural success rates while reducing vascular complications and mortality, particularly in patients with acute coronary syndrome.123 Current guidelines recommend TRA over TFA for patients with acute coronary syndrome and endorse TRA for patients with stable ischemic heart disease.45
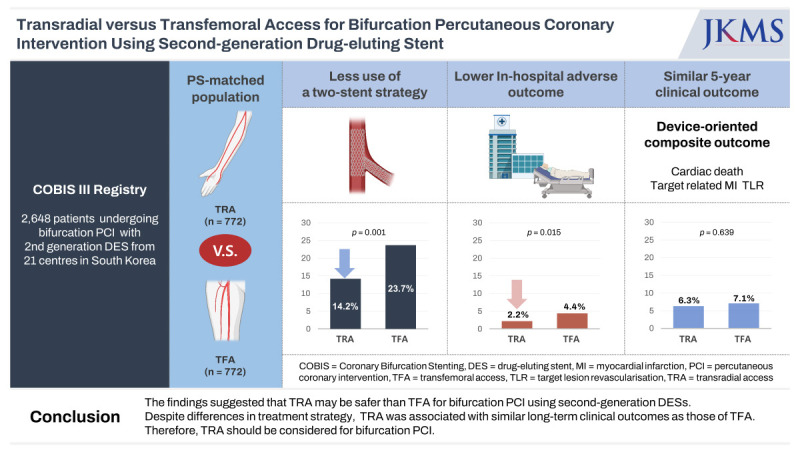
Recent technological advances in percutaneous coronary intervention (PCI) devices have made TRA the default route for treating complex coronary artery diseases. However, several operators advocate TFA over TRA during complex PCIs, likely because of the greater backup support with a large-bore guiding catheter and the availability of larger devices. Furthermore, no clear evidence or guidelines exist regarding the clinical benefits of TRA over TFA for complex PCI, such as bifurcation PCI, which accounts for approximately 15% of all PCI cases.67 TRA is a feasible alternative, even for left main (LM) bifurcation treatment, in previous Coronary Bifurcation Stenting (COBIS) registries.89 However, these registries involved first-generation drug-eluting stents (DESs). This study compared the procedural differences and in-hospital and long-term outcomes of TRA and TFA for bifurcation PCI using second-generation DESs.
METHODS
Study population
The COBIS III Registry, a multicenter, observational, real-world registry, includes 2,648 patients treated for bifurcation lesions using second-generation DESs between January 2010 and December 2014 at 21 PCI centers in South Korea. Patients were categorized into two groups based on the vascular access: TRA, 1,507 (56.9%) patients; TFA, 1,141 (43.1%) patients.
The major inclusion criteria were any bifurcation lesions treated solely with second-generation DESs; a main vessel diameter ≥ 2.5 mm; and a side branch diameter ≥ 2.0 mm, confirmed with core laboratory quantitative coronary angiography analysis. The major exclusion criteria were cardiogenic shock, cardiac arrest with successful resuscitation during hospitalization, protected LM disease, and severe left ventricular dysfunction (i.e., ejection fraction < 30%). The COBIS III Registry has been previously described.10
Procedural details
PCI procedures were performed using current standard guidelines and conventional techniques. All patients received a loading dose of aspirin (300 mg) and P2Y12 inhibitors (clopidogrel [300–600 mg], prasugrel [60 mg], or ticagrelor 180 mg]) at least 12 hours before PCI.45 The vascular access route was selected by the attending physicians. Stenting techniques, including one- or two-stent strategies, final kissing balloon (FKB), proximal optimization technique (POT), or re-POT, and the DES were selected at the operators’ discretion. Intravascular ultrasound-guided intervention was recommended to obtain optimal stent expansion and apposition. The type, dose, and duration of dual antiplatelet therapy and cardiovascular medications were decided by the physician.
Data collection and quantitative coronary angiography analysis
A web-based reporting system collected data on the patients’ demographics, medications, laboratory findings, and angiographic and procedure details. Follow-up outcomes were collected from medical records or telephone interviews in cases of follow-up loss. An angiographic core laboratory (Heart Vascular Stroke Institute in Samsung Medical Center, Seoul, Korea) quantitatively analyzed baseline and procedural coronary angiograms using an automated edge-detection system (Centricity CA 1000; GE Healthcare, Waukesha, WI, USA).10 Bifurcation lesions were divided into three segments; proximal main vessel, distal main vessel, and side branch. Those with Medina Classifications11 of 1.1.1, 1.0.1, and 0.1.1 were considered true bifurcations.
Study endpoints
The primary endpoint was the incidence of device-oriented composite outcome (DOCO), defined as the composite of cardiac death, target vessel-related myocardial infarction (MI), and target lesion revascularization. The secondary endpoints included the individual components of the DOCO, patient-oriented composite outcome (i.e., a composite of death from any cause, any MI, and any revascularization), and target vessel revascularization. In-hospital outcomes were evaluated based on periprocedural complications, which included access site complications, periprocedural MI, emergent repeat procedures, cardiogenic shock, and acute heart failure. All clinical events were verified by an independent clinical event adjudicating committee composed of interventional cardiology experts not involved in patient enrolment, as previously described.10
Statistical analysis
Data are presented as number (%) or mean ± standard deviation. Continuous variables were compared using Student’s t-tests. Categorical variables were compared using χ2 or Fisher’s exact tests. The cumulative events of clinical outcomes were assessed using Kaplan–Meier estimates and compared with log-rank tests. All clinical endpoints were analyzed until the date of an endpoint event, loss to follow-up, or up to 5 years after the index procedure.
Propensity scores were estimated using multivariate logistic regression analyses on all covariates listed in Tables 1 and 2. Nearest-neighbor matching with a caliper of 0.005 was used and considered satisfactory when the standardized mean differences were < 10% (Supplementary Fig. 1). The propensity scores yielded a C-statistic of 0.714, which indicated a good ability to differentiate between both groups. In subgroup analysis, adjusted hazard rates were calculated by means of multivariate Cox regression with clinical and lesion characteristics among propensity scores-matched populations.
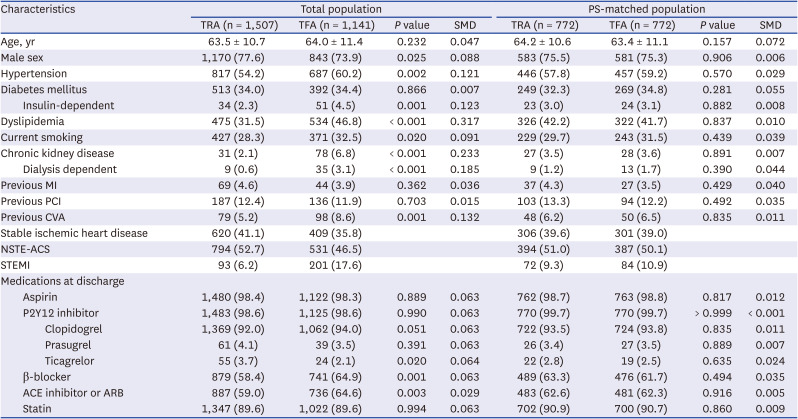
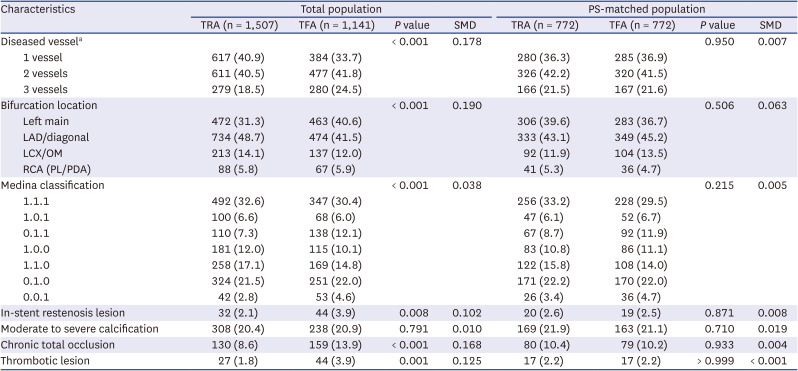
Table 1
Baseline characteristics
Data are presented as number (%) or mean ± standard deviation.
TRA = transradial access, TFA = transfemoral access, SMD = standardized mean difference, PS = propensity score, MI = myocardial infarction, PCI = percutaneous coronary intervention, CVA = cerebrovascular attack, NSTE-ACS = non-ST-segment-elevation-acute coronary syndrome, STEMI = ST-segment-elevation myocardial infarction, ACE = angiotensin converting enzyme, ARB = angiotensin II receptor blocker.
![]()
Table 2
Lesion characteristics
Data are presented as number (%).
TRA = transradial access, TFA = transfemoral access, SMD = standardized mean difference, PS = propensity score, LAD = left anterior descending artery, LCX = left circumflex artery, OM = obtuse marginal artery, RCA = right coronary artery, PL = posterolateral artery, PDA = posterior descending artery.
aA diseased vessel was defined as a vessel with at least 50% stenosis.
![]()
Statistical analyses were conducted using SPSS version 26.0 (IBM Corp., Armonk, NY, USA) and R Statistical Software version 4.2.2 (R Foundation for Statistical Computing, Vienna, Austria). P values < 0.05 was considered statistically significant.
RESULTS
Baseline characteristics
In the total study population, patients in the TRA group were more likely to be male than those in the TFA group, and less likely to have a history of cardiovascular risk factors such as hypertension, insulin-dependent diabetes, dyslipidemia, chronic kidney disease, and previous cerebrovascular accident (Table 1). In addition, patients with ST-segment elevation MI were less likely to be treated via TRA. After conducting propensity score matching (PSM), no statistical differences existed between the two groups with respect to baseline clinical variables, clinical presentation, and medications at discharge.
Lesion characteristics
In the total study population, the prevalence of complex lesions was lower in the TRA group than in the TFA group (Table 2). Specifically, the TRA group had a lower incidence of multivessel disease, LM bifurcation lesions, in-stent restenosis lesions, chronic total occlusion, and thrombotic lesions. However, after PSM, all lesion characteristics were similar between the two groups.
Procedural characteristics and in-hospital adverse outcomes
In the total study population, patients in the TRA were more likely to be treated with the one-stent strategy, whereas patients in the TFA were more likely to be treated with the two-stent strategy (Table 3). Thus, the TRA group had a significantly lower number of stents used, less use of FKB inflation, and greater use of POT or re-POT than the TFA group. After PSM, differences remained with regard to the proportion of patients being treated with the two-stent strategy in the TRA group versus the TFA group (14.2% vs. 23.7%, P < 0.001), number of stents used (1.8 ± 0.9 vs. 1.9 ± 1.1, P < 0.001), and use of FKB (27.5% vs. 36.5%, P < 0.001).
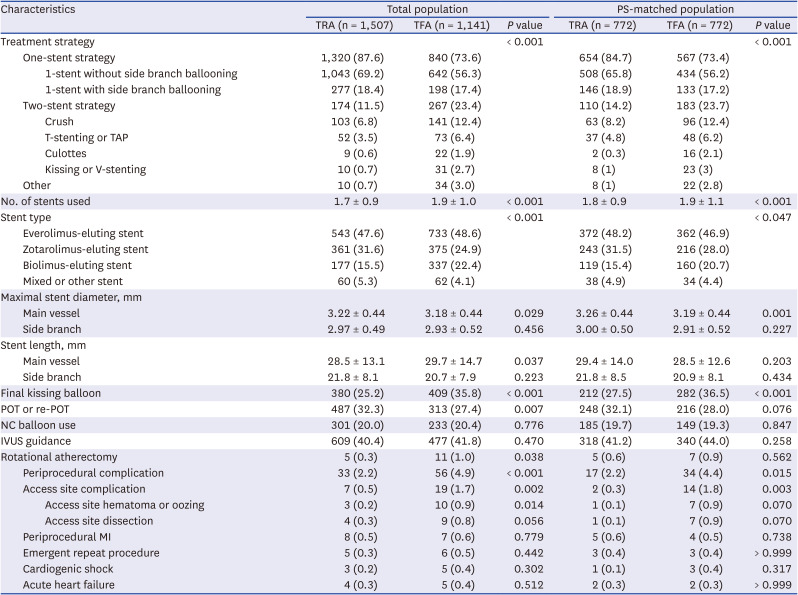
Table 3
Procedural characteristics and in-hospital adverse outcomes
Data are presented as number (%) or mean ± standard deviation.
TRA = transradial access, TFA = transfemoral access, PS = propensity score, TAP = T and small protrusion, POT = proximal optimization technique, NC = noncompliant, IVUS = intravascular ultrasound, MI = myocardial infarction.
![]()
In the total study population, the TRA group, compared to the TFA group, had significantly lower rates of periprocedural complications (2.2% vs. 4.9%, P < 0.001), primarily driven by the lower rate of access site complications (0.5% vs. 1.7%, P = 0.002). These differences were maintained after PSM, with access site complications of 0.3% and 1.8% (P = 0.003) in the TRA and TFA groups, respectively. However, no significant differences existed between the TRA and TFA groups in other adverse events such as periprocedural MI, emergent repeat procedures, cardiogenic shock, and acute heart failure.
In addition, a temporal trend of increased use of TRA for bifurcation PCI was observed (Supplementary Fig. 2). The percentage of TRA procedures increased from 46.6% to 70.7% over the study period.
Long-term clinical outcomes
The median follow-up duration was 53 months. In the total population, the incidence of DOCO, the primary outcome, was significantly lower in the TRA group than in the TFA group (Table 4, Fig. 1A). In addition, the secondary outcomes patient-oriented composite outcome, target lesion revascularization, and target vessel revascularization were lower in the TRA group. However, the incidence of all adverse clinical events was similar between the two groups after PSM (Fig. 1B). The incidence of DOCO was not different between the TRA and TFA groups (6.3% vs. 7.1%, P = 0.639). Fig. 2 illustrates the results of the subgroup analysis of DOCO, based on vascular access, among the propensity score-matched population. There were no significant differences between access sites in the various subgroups. Furthermore, detailed subgroup analysis also revealed no significant differences between access sites based on bifurcation location, medina classification, and whether intravascular ultrasound was used (Supplementary Fig. 3).
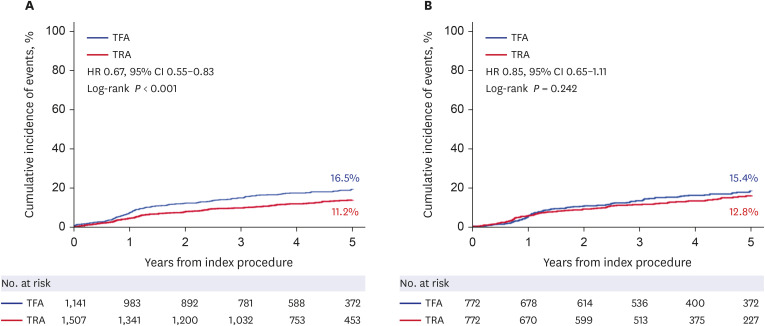
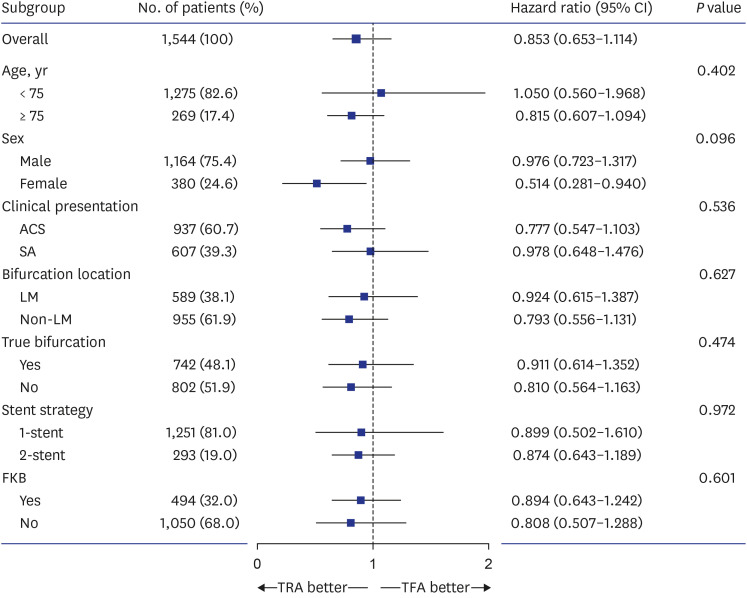
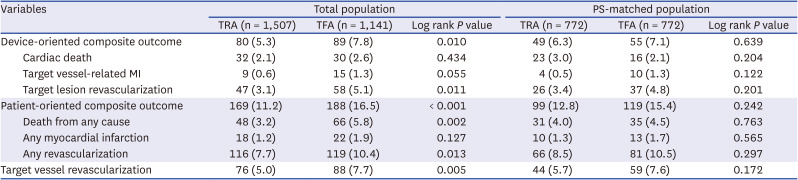
Fig. 1
Patient-oriented composite outcome based on vascular access in the total (A) and propensity score-matched populations (B).
HR = hazard ratio, CI = confidence interval, TFA = transfemoral access, TRA = transradial access.
![]()
Fig. 2
Subgroup analysis of device-oriented composite outcome.
CI = confidence interval, ACS = acute coronary syndrome, SA = stable angina, LM = left main, TRA = transradial access, TFA = transfemoral access.
![]()
Table 4
Cumulative incidence of adverse events at 5 years
Data are presented as number (%).
TRA = transradial access, TFA = transfemoral access, PS = propensity score, MI = myocardial infarction.
![]()
DISCUSSION
We evaluated procedural differences, in-hospital adverse outcomes, and long-term clinical outcomes during a 5-year follow-up between TRA and TFA for bifurcation PCI by using multicenter, observational, real-world registry data in the second-generation DES era. The major study findings were: 1) compared to TFA, TRA was associated with a simple strategy involving less use of the two-stent and FKB techniques; 2) TRA was associated with lower in-hospital adverse outcomes, especially access site complications; 3) TRA and TFA had similar long-term clinical outcomes, despite differences in treatment strategy; and 4) an increasing trend was noted for using TRA for bifurcation PCI.
Previous large-scale randomized trials have revealed that TRA is superior to TFA in terms of access site bleeding, which ultimately reduced cardiac mortality, especially for patients with acute coronary syndrome.123 To reduce bleeding complications, TRA is recommended as a default strategy across the whole spectrum of ischemic heart disease.1213 A recent meta-analysis14 of LM PCI also demonstrated that TRA was associated with reduced bleeding and lower access site or vascular complications compared with TFA. This is consistent with our findings.
Recent technological advances in PCI devices have allowed TRA to be used in complex coronary artery diseases. The preference for TRA over TFA in PCI is growing. However, many operators hesitate to use TRA, especially during a complex procedure, likely because of poor backup support and the limited availability of larger devices. Regarding the radial artery diameter, most patients can be treated with a conventional 6 French guide during TRA.15 Nevertheless, the use of the two-stent strategy with a 6 French guide is limited, especially when two stents with larger diameters are inserted simultaneously. However, this limitation could be overcome by using a sheathless guide system or large-bore sheath, which provides a larger inner diameter without increasing the outer diameter.1617 Current guidelines recommend a one-stenting strategy with provisional side branch stenting as the initial approach for treating bifurcation lesions; the limitation of selecting the two-stent strategy should not affect clinical outcomes.18 In this study, use of the two-stent strategy was significantly lower in the TRA group, followed by FKB, even after adjusting for baseline clinical and angiographic characteristics. Despite the limitations of the two-stent strategy during TRA, the clinical outcomes were similar between the two groups. These findings suggest that TRA operators tend to prefer simple procedures that do not result in poor clinical outcomes.
Previous studies have evaluated the clinical benefits of using TRA versus TFA for bifurcation PCI.89 The COBIS I registry, which enrolled patients from 2004 to 2006, revealed no significant differences between TRA and TFA for non-LM lesions in procedural success rates or in long-term safety and efficacy.8 The COBIS II Registry, which enrolled patients from 2003 to 2009 with LM and non-LM lesions, similarly demonstrated that TRA was superior to TFA in reducing bleeding complications and had comparable long-term clinical outcomes.9 However, these studies used first-generation DESs and may therefore have limited applicability. Our study confirmed that TRA was superior to TFA in reducing vascular complications and had similar clinical outcomes to bifurcation PCI with second-generation DESs. In addition, the rate of TRA was 30.2% in the COBIS I registry, 24.9% in COBIS II, and 56.9% in this study, highlighting a growing preference for TRA in bifurcation PCI.
Our study had several limitations. First, this was a non-randomized, retrospective, observational study; therefore, the potential for selection bias exists. Thus, PSM was conducted to adjust for confounding variables. This registry did not have detailed information about sheath size or the use of a sheathless guide on TRA due to its retrospective nature. Second, the choice of access site was largely determined by operator preference or hospital policy, which led to differences in baseline clinical and angiographic variables between the TRA and TFA groups. Despite conducting PSM, residual confounding factors could have affected the results. Third, the COBIS III Registry does not provide data on the rate of crossover from TRA to TFA or vice versa during bifurcation PCI. It was possible to change access sites from TRA to TFA during bifurcation PCI due to unpredictable complications. Accordingly, future prospective studies might be required which include vascular access and the rate of crossover during bifurcation procedure. Fourth, data on non-access site bleeding were unavailable. Finally, the registry did not include data on physiology-guided PCI, which may have an impact on clinical outcomes.
In conclusion, TRA showed similar long-term clinical outcomes compared to TFA for bifurcation PCI using second-generation DESs. Furthermore, our study also suggested that TRA enables operators to execute a simple strategy with fewer procedural complications compared to TFA. The use of TRA in bifurcation PCI is increasing. Nonetheless, further large randomized controlled studies are needed to confirm these findings. Overall, the results provide important clinical evidence to support the default use of TRA for bifurcation PCI.
 XML Download
XML Download