

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Root canal therapy is widely employed to remove infectious material, effectively treat periapical pathologies, and prevent their recurrence. This is accomplished through thorough cleaning, precise shaping, and optimal obturation with core filling materials and sealers [12]. Root canal sealers are luting agents used in endodontic procedures to ensure a tight seal between the filling material and the prepared dentinal walls. They are essential for the success of root canal obturation, providing physicochemical properties that enable 3-dimensional, impervious adhesion. In addition to creating an airtight seal to prevent microleakage, based on the findings of several studies [13], Gasner and Brizuela [4] highlighted 7 ideal properties of a sealer: biocompatibility, resistance to shrinkage upon setting, insolubility in tissue fluids, antimicrobial activities, non-irritating to periapical tissues, non-staining, and radiopacity.
Sealers vary based on their composition, encompassing 5 main types. Zinc oxide eugenol, commonly used in primary teeth, exhibits anti-inflammatory and antibacterial effects. However, it undergoes a deterioration process upon setting, resulting in a brittle material that is prone to higher microleakage rates compared to other sealers [5].
Resin-based sealers are the most commonly used type of sealers and are categorized into 2 groups: epoxy resin-based sealers, such as AH Plus—which is considered the “gold standard”—known for their low solubility rates, strong adhesion, and stability; and methacrylate resin-based sealers, which adhere to the filling material and the dentin walls as a single unit, an approach known as the Monoblock concept. This improves the mechanical strength of vulnerable roots. However, the shrinkage stresses associated with methacrylate resin-based sealers can compromise their effectiveness, leading to increased risks of microleakage, mutagenicity, and allergic reactions [6].
The third type, bio-ceramic sealers (such as mineral trioxide aggregate [MTA]) comprises hydrophilic, bio-active sealers based on calcium silicate or calcium phosphate components. This type demonstrates regenerative abilities, fostering a finer biological status and promoting apical healing [7]. Due to their excellent adhesion, re-treatment therapy is considered more challenging than after conventional root canal treatment [8]. Calcium hydroxide sealers, another type, generate reparative and remineralization effects due to their alkalinity [9]. They exhibit lower cytotoxicity than other sealers but present a disadvantage with their high solubility [5]. Glass ionomer-based sealers, the final type, establish robust dentin bonding, which overall enhances apical sealing and resistance to root fracture. However, their strong dentine bonding complicates re-treatment procedures [10]. It is important to note that no sealer type has completely eliminated leakage or met all the ideal characteristics outlined by Gasner and Brizuela [4]. Clinical trials play a pivotal role in improving medical treatments, offering an opportunity to discover more reliable treatments for future outcomes. Notably, approximately 9% of all related root canal sealer studies published on PubMed since the date of this paper, are clinical trials [1112]. Therefore, the aim of this study is to present comprehensive results and analyses of clinical trials, providing updates on the diverse functions of root canal sealers.
MATERIALS AND METHODS
Search protocol and the selection criteria
The ClinicalTrials.gov site, provided by the U.S. National Library of Medicine (https://clinicaltrials.gov), is a dynamic global database that meticulously collects clinical studies from around the world and receives regular updates weekly [12]. All submitted trials in this database must provide comprehensive information about the trial's history and the registration protocol [13].
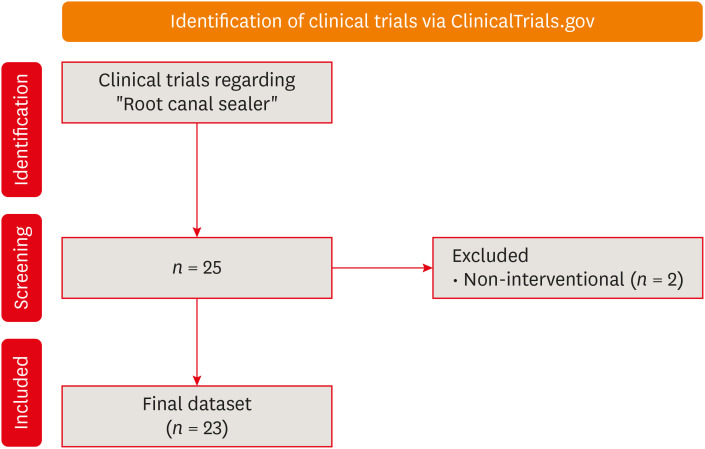
In June 2023, we conducted a search on ClinicalTrials.gov for all clinical trials related to root canal sealers. We did not impose any limitations and used the term “alveolar bone grafting” in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Protocols (PRISMA-P) [14]. By utilizing the advanced search feature and employing Boolean operators AND, OR, NOT within the ClinicalTrials.gov registry, our search terms included “root canal sealer,” “MTA,” “mineral trioxide aggregate,” “bio ceramic sealer,” “resin-based sealers,” “zinc oxide eugenol,” “glass ionomer-based sealer,” and “calcium-hydroxide sealers.” The search yielded a total of 25 trials, covering a comprehensive spectrum. Our selection criteria led to the inclusion of only interventional, non-observational trials related to root canal sealers. We subsequently excluded 2 non-interventional trials, resulting in a total of 23 trials for this study (Figure 1). Several studies employed the same methodologies [151617]. The PICO framework followed was P (population): patients undergoing root canal treatment, I (intervention): sealers, C (comparison): different types of sealers, O (outcome): histopathologic findings, post-operative pain, and sealing capacity.
Trial collection and related publications
Using the ClinicalTrials.gov site, we collected data on all related trials, noting their phases, trial status, primary endpoints, selection criteria, sample size, study design, experimental interventions, sealer type, number of visits, trial locations, results disclosure, and any associated publications. For trial publications, we conducted a comprehensive search of the PubMed/MEDLINE and Scopus databases using the NCT ID of each trial. The findings are presented in Table 1. The search was conducted by 2 inspectors (A.A.M. and Y.E.M.) to minimize the possibility of mistakes and errors.
Table 1
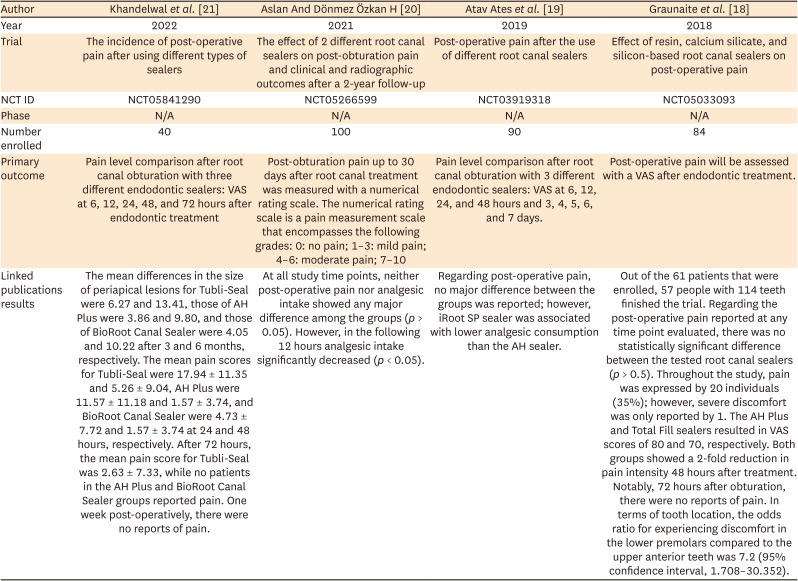
Clinical findings of published trials regarding post-operative pain associated with different types of sealers, as of June 2, 2023 (n = 4)
| Author | Khandelwal et al. [21] | Aslan And Dönmez Özkan H [20] | Atav Ates et al. [19] | Graunaite et al. [18] |
|---|---|---|---|---|
| Year | 2022 | 2021 | 2019 | 2018 |
| Trial | The incidence of post-operative pain after using different types of sealers | The effect of 2 different root canal sealers on post-obturation pain and clinical and radiographic outcomes after a 2-year follow-up | Post-operative pain after the use of different root canal sealers | Effect of resin, calcium silicate, and silicon-based root canal sealers on post-operative pain |
| NCT ID | NCT05841290 | NCT05266599 | NCT03919318 | NCT05033093 |
| Phase | N/A | N/A | N/A | N/A |
| Number enrolled | 40 | 100 | 90 | 84 |
| Primary outcome | Pain level comparison after root canal obturation with three different endodontic sealers: VAS at 6, 12, 24, 48, and 72 hours after endodontic treatment | Post-obturation pain up to 30 days after root canal treatment was measured with a numerical rating scale. The numerical rating scale is a pain measurement scale that encompasses the following grades: 0: no pain; 1–3: mild pain; 4–6: moderate pain; 7–10 | Pain level comparison after root canal obturation with 3 different endodontic sealers: VAS at 6, 12, 24, and 48 hours and 3, 4, 5, 6, and 7 days. | Post-operative pain will be assessed with a VAS after endodontic treatment. |
| Linked publications results | The mean differences in the size of periapical lesions for Tubli-Seal were 6.27 and 13.41, those of AH Plus were 3.86 and 9.80, and those of BioRoot Canal Sealer were 4.05 and 10.22 after 3 and 6 months, respectively. The mean pain scores for Tubli-Seal were 17.94 ± 11.35 and 5.26 ± 9.04, AH Plus were 11.57 ± 11.18 and 1.57 ± 3.74, and BioRoot Canal Sealer were 4.73 ± 7.72 and 1.57 ± 3.74 at 24 and 48 hours, respectively. After 72 hours, the mean pain score for Tubli-Seal was 2.63 ± 7.33, while no patients in the AH Plus and BioRoot Canal Sealer groups reported pain. One week post-operatively, there were no reports of pain. | At all study time points, neither post-operative pain nor analgesic intake showed any major difference among the groups (p > 0.05). However, in the following 12 hours analgesic intake significantly decreased (p < 0.05). | Regarding post-operative pain, no major difference between the groups was reported; however, iRoot SP sealer was associated with lower analgesic consumption than the AH sealer. | Out of the 61 patients that were enrolled, 57 people with 114 teeth finished the trial. Regarding the post-operative pain reported at any time point evaluated, there was no statistically significant difference between the tested root canal sealers (p > 0.5). Throughout the study, pain was expressed by 20 individuals (35%); however, severe discomfort was only reported by 1. The AH Plus and Total Fill sealers resulted in VAS scores of 80 and 70, respectively. Both groups showed a 2-fold reduction in pain intensity 48 hours after treatment. Notably, 72 hours after obturation, there were no reports of pain. In terms of tooth location, the odds ratio for experiencing discomfort in the lower premolars compared to the upper anterior teeth was 7.2 (95% confidence interval, 1.708–30.352). |
RESULTS
Trial characteristics
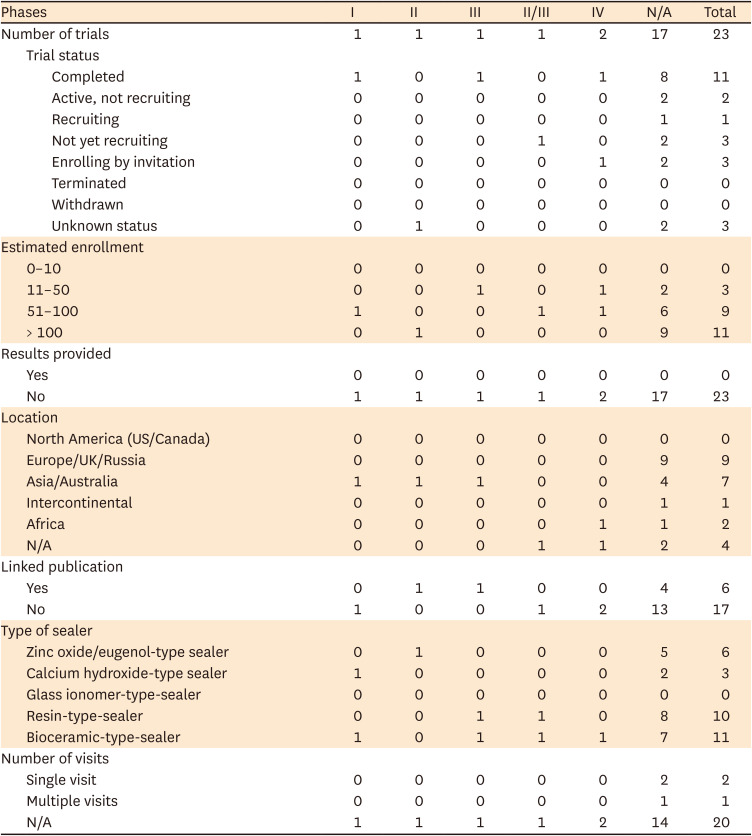
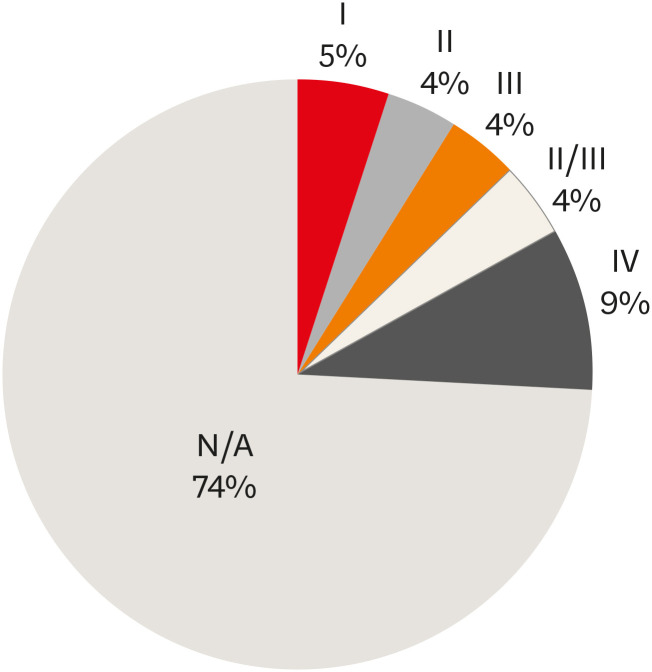
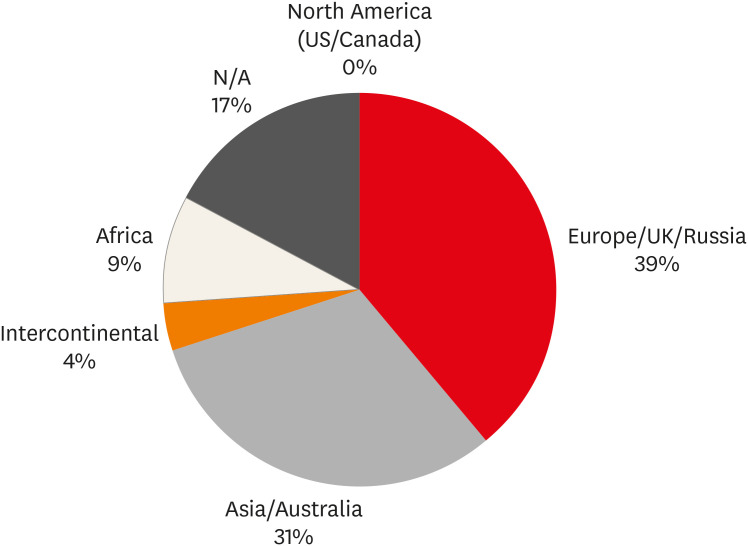
The predefined standards were met by 23 clinical trials. Table 2 presents the results of these trials, categorized by trial phase, status, number of enrolled patients, sealer type, number of visits, results provided, trial location, and associated publications. Notably, 11 of the 23 trials were successfully completed, with none being terminated or withdrawn. Each trial included at least 10 participants, with 11 trials enrolling over 100 participants. However, none of the trials provided outcomes, and the majority (17 out of 23) lacked associated publications, resulting in a dearth of valuable trial results and published data. Regarding the types of sealers used in the trials, zinc oxide/eugenol sealers were used in 6 trials, calcium hydroxide in 4, resin-based sealers in 10, and bioceramic in 11. Notably, none employed glass ionomer sealers. Only 1 visit was required for treatment in 2 of the trials studied, while multiple visits were necessary for just 1 trial. Concerningly, for the remainder, the treatment duration was not clearly defined. The majority of trials did not specify their phase, with 17 out of 23 trials, or 74%, falling into this category. Phase 4 trials were conducted in 2 instances, while the remaining trials were evenly distributed among phases I, II, III, and II/III (Figure 2). Of the 2,978 participants involved, 2,512 were part of trials with an unspecified phase, with the rest distributed among the other phases (Figure 2). The trials were conducted across various regions, with Europe/UK/Russia hosting the majority at 9 trials. North America (US/Canada) was an exception, with no trials conducted there. The remaining trials were spread across Asia/Australia, intercontinental locations, Africa, and some were unidentified (Figure 3).
Table 2
Clinical trials on root canal sealers as found on ClinicalTrials.gov as of June 2, 2023 (n = 23)
Phase I trials: Only 1 phase I trial has been completed, involving 80 participants. This trial took place in Asia/Australia, but neither the results nor the associated publication have been provided. It utilized a combination of a calcium hydroxide-type sealer and a bioceramic type. There was no expected time frame for healing associated with this trial.
Phase II trials: Only one trial with unknown status in phase II, involved 200 participants across Asia and Australia. Although the results were not disclosed, associated publications were linked to the study. This trial employed a zinc oxide/eugenol-type sealer and did not specify a recommended healing period.
Phase III trials: A completed phase III trial was conducted in Asia and Australia with 42 participants. Although it did not yield definitive results, there were some associated publications. This trial utilized a resin-type sealer and did not recommend a specific treatment duration.
Phase II/III trials: Only 1 phase II/III trial, which has not yet begun recruiting, is being conducted in an unspecified region. This study is planned to include 60 participants, but as of now, there are no available results or associated publications. Both a resin-type sealer and a bioceramic type are being utilized in this trial. The study does not propose a specific recovery time.
Phase IV trials: Two phase IV trials conducted in Africa, which involved 84 participants, have been completed. However, they yielded no significant findings and did not result in any associated publications. These trials utilized a bioceramic-type sealer and were unable to determine a specific number of visits required for healing.
Unknown phase trials: There were 17 trials of an unknown phase, with 8 completed, and none terminated or withdrawn. These trials spanned various nations, with North America (US/Canada) not included. Most trials enrolled over 100 participants, cumulatively totaling 2,512 individuals. However, none reported outcomes, and most lacked associated publications. A diverse range of sealers was employed in these trials, with the exception of the glass ionomer variety. While some of the 17 trials indicated a single or multiple visits for treatment, the majority did not define a specific timeframe.
Qualitative analysis
The linked publications of clinical trials were related to the usage of different types of root canal sealers concerning post-operative pain (Table 1).
Effect of resin, calcium silicate, and silicon-based root canal sealers on post-operative pain
To assess the impact of resin, calcium silicate, and silicon-based root canal sealers on post-operative pain, we analyzed a sample of 84 participants with mandibular molar teeth diagnosed with symptomatic irreversible pulpitis. These individuals underwent endodontic treatment and their pain levels were subsequently measured using a visual analog scale (VAS). The VAS consisted of a 100-mm ruler, marked at 10-mm intervals, with a scale ranging from zero to 10 to quantify pain intensity. Out of the 61 patients who completed the trial, no significant difference in post-operative pain was observed between the different root canal sealers at any of the time points assessed (p > 0.05). Only 20 of the 84 participants (approximately 24%) reported experiencing pain, with one individual describing it as severe. Specifically, the AH Plus (Dentsply Maillefer, Ballaigues, Switzerland) and Total Fill (FKG Dentaire SA, La Chaux-de-Fonds, Switzerland) sealers resulted in VAS scores of 80 and 70, respectively. Both groups showed a 2-fold reduction in pain intensity 48 hours after treatment. Notably, 72 hours after obturation, there were no reports of pain. In terms of tooth location, the odds ratio for experiencing discomfort in the lower premolars compared to the upper anterior teeth was 7.2 (95% confidence interval, 1.708–30.352) [18].
Post-operative pain after the use of different root canal sealers.
A VAS was recorded at 6, 12, 24, and 48 hours, as well as 3, 4, 5, 6, and 7 days after obturation. The purpose of this measurement was to compare the level of discomfort experienced after root canal obturation using 3 different endodontic sealers. In the analysis of post-operative pain incidence between the 2 calcium silicate-based root canal sealers and the epoxy resin sealer group, no significant differences were observed. Among the 90 patients included in the study, who were aged 18 to 60 years, demonstrated good oral hygiene, had not taken analgesics in the last 24 hours or antibiotics in the previous week, and were diagnosed with asymptomatic irreversible pulpitis, the iRoot SP sealer was associated with a lower analgesic intake than the AH Plus sealer [19].
The effect of 2 different root canal sealers on post-obturation pain and 2-year clinical and radiographical outcome
To analyze the impact of 2 different root canal sealers on post-obturation pain, 100 patients over the age of 18 were tested using resin-based and mineral trioxide aggregate-based sealers. These individuals were in good oral health, had asymptomatic irreversible pulpitis in the mandibular region, and had not previously undergone endodontic or restorative treatment. After cavity preparation, the patients showed significant pulpal exposure and exhibited delayed responses to cold and electrical pulp testing. A numerical rating scale was employed to assess post-obturation discomfort over a 30-day period following root canal treatment. The scale ranged from 0, indicating no pain, to 1–3 for mild discomfort, 4–6 for moderate discomfort, and 7–10 for severe pain. The use of this pain scale indicated a significant difference in post-operative pain and analgesic consumption (p > 0.05). Notably, a marked decrease in pain levels was observed only after 12 hours had elapsed [20].
The incidence of post-operative pain after using different types of sealers
To track the occurrence of post-operative pain following various types of sealers, we enrolled 40 individuals aged between 18 and 50 years with symptomatic irreversible pulpitis in the study. Pain was quantified using a VAS. Participants recorded their pain levels on a 10-cm line with a single handwritten mark: a zero on the left end indicated no pain, while a 10 on the right signified the most severe discomfort. Each assessment time point was represented by a single outcome. Based on this rating scale, the mean differences in the size of periapical lesions for Tubli-Seal were 6.27 and 13.41, those of AH Plus were 3.86 and 9.80, and those of BioRoot Canal Sealer were 4.05 and 10.22 after 3 and 6 months, respectively. The mean pain scores for Tubli-Seal were 17.94 ± 11.35 and 5.26 ± 9.04, AH Plus were 11.57 ± 11.18 and 1.57 ± 3.74, and BioRoot Canal Sealer were 4.73 ± 7.72 and 1.57 ± 3.74 at 24 and 48 hours, respectively. After 72 hours, the mean pain score for Tubli-Seal was 2.63 ± 7.33, while no patients in the AH Plus and BioRoot Canal Sealer groups reported pain. One week post-operatively, there were no reports of pain [21].
DISCUSSION
The present paper offers a thorough review of the current state of clinical trials related to root canal sealers. Sealers are essential in endodontic procedures, and thus, an updated review of clinical trials is important to provide fresh perspectives on root sealers and the latest techniques. This is aimed at improving the therapeutic outcomes of endodontic treatments.
Limited geographic territory
Our results indicate that regions with the highest rates of root canal treatment also exhibit the most active root canal sealer clinical trial activity. Notably, 39% of these clinical trials were conducted in European facilities, with France accounting for half of these trials. This substantial European contribution is consistent with the findings of León-López et al. [22], which reported that 59.6% of the European population had at least 1 root-filled tooth. Additionally, Asian facilities accounted for 31% of clinical trials, reflecting the high rate of root canal treatment in the region, where 58.8% of the population had at least 1 root-filled tooth [22]. This surpassed the activity in the USA and Canada, which, according to the PubMed database, had no trials and no papers related to root canal sealers originating from these countries [11].
Trials’ phase status and the number of published results
The reliability of many trials is questionable because their phase status is unknown. Moreover, a significant number of patients have been enrolled in studies whose phases are not disclosed [23]. Therefore, future trials should be conducted with clearly defined phase statuses to ensure the generation of more reliable data.
In addition, none of the 23 trials presented their results and only 6 trials presented related published results; this finding is in accordance with similar studies [1516]. The majority of publications concentrated on post-operative pain, with none addressing the ideal characteristics outlined by Gasner and Brizuela [4]. Additionally, several studies have discussed why few trials have provided their results or published their outcomes. According to Anderson et al. [24], the low number of published data may be due to negative outcomes obtained or authors' lack of inclination to publish. This lack of results may affect dental practitioners and patients [242526].
Type of sealers and number of visits
Root canal sealers are divided into 5 main groups according to their composition: zinc oxide eugenol-based, calcium hydroxide-based, glass ionomer-based, resin-based, and bioceramic sealers [4]. Several studies have highlighted the differences between these main groups, regarding physical and chemical properties. Silveira et al. [27] reported that resin-based sealers provide better sealing and exhibit lower solubility than MTA and bioceramic sealers. From a histopathological perspective, calcium hydroxide-based sealers are associated with the least inflammatory response compared to their resin-based counterparts. Regarding the number of treatment visits, Mergoni et al. [28] found that there was no significant difference in post-operative pain control or complications between single and multiple visit protocols. However, the single visit approach did show a marginal improvement in post-operative pain management.
Therapeutic benefit
Root canal sealers play a crucial role in endodontic treatments and have broader implications for dental procedures. There is a growing global concern about the prevalence of periapical lesions, which affect 52% of the population, highlighting the need for effective treatment and sealing [29]. In root canal treatment, after thorough cleaning and shaping of the canal system, the goal is to maintain this complex system in a histologically stable, sterile, and sealed state using various types of root canal sealers [4]. Several studies have linked pulpal infection and the formation of periradicular lesions to systemic conditions such as cardiovascular disease, diabetes mellitus, pregnancy outcomes, and metastasis infection [303132]. Therefore, it is essential to provide adequate root canal treatment and maintain its stability with an impervious sealed obturation to prevent bacteremia and septicemia [33]. Furthermore, several studies have reported the effects of root canal sealer on biocompatibility, genotoxicity, pain reduction post-treatment, and sealing properties [318192134]. In addition, Parirokh et al. [35] reported that adequately sealed root canal treatments show no significant difference when compared with tooth extraction and the placement of dental implants. In terms of quality of life, Hamasha and Hatiwsh [36] found that 90% of participants in their study reported improvements in taste ability, pain control, food ingestion, and self-esteem following adequate root canal treatment.
The primary limitation of this study lies in relying solely on data from ClinicalTrials.gov, potentially limiting new information due to small trial pools or registration errors. Thus, multiple precautions were taken to minimize errors during the data collection process.
CONCLUSIONS
This study comprehensively describes the current landscape of clinical trials focusing on root canal sealers. It underscores the limited geographic diversity of trial locations, the non-reporting of results, and the dearth of clinical trials examining the physicochemical properties of various sealer types. The primary outcomes reported in related publications were predominantly concerned with the effect of sealers on post-operative pain. Moreover, no significant differences were observed in terms of post-operative pain management. Therefore, additional research is warranted to investigate the advantages of incorporating emerging technologies with different root canal sealers to achieve enhanced and more efficacious therapeutic results.
 XML Download
XML Download