

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Blood pressure (BP) is a key biomarker that reflects the risk of vascular disease. Regular BP monitoring has proven effective in reducing the risk of cardiovascular diseases (CVDs).1)2) However, BP follows a circadian rhythm,3) shows significant inter-individual variability,4) and these distinct patterns are associated with varying CVD risks.5)
Ambulatory BP monitoring (ABPM), conducted outside the traditional medical setting, has demonstrated greater diagnostic value compared to conventional in-office measurements.6)7) This has led to an increased emphasis on 24-hour BP monitoring in healthcare. However, the nature of cuff inflations poses challenges for continuous BP monitoring. The primary issue with cuff inflation is patient’s discomfort during the monitoring period, especially while sleeping. This discomfort not only has the potential to compromise the accuracy of the monitoring but also poses challenges for repeated data collection sessions, particularly those extending beyond a single instance (e.g., 48 hours).8)9)10) To address these limitations, cuffless BP monitoring devices have been developed, enabling prolonged and uninterrupted BP monitoring. In contrast to traditional cuff-based measurement devices, CART-I operates uniquely by conducting BP measurements without the patient’s awareness. It autonomously gathers BP data at regular intervals without applying pressure.11) The ring-type device is more comfortable for patients, potentially enhancing adherence to BP monitoring protocols and more reliable long-term data collection.
The potential of photoplethysmography (PPG) for BP estimation has gained increasing attention and various non-parametric learning methods have been widely used in this field.12)13) Moreover, advances in machine learning and artificial intelligence14)15) have been instrumental in identifying BP-related features from PPG waveforms. However, for cuffless BP measurement devices to be considered suitable for clinical practice, including hypertension screening, diagnosis, treatment, and monitoring, standardized validation tests are essential.16) Nevertheless, the effectiveness of cuffless devices in comparison to a conventional ABPM device for continuous BP monitoring has not been fully evaluated yet. We conducted this study to assess the feasibility and accuracy of a ring-type cuffless BP measurement device, following the recommendation from the European Society of Hypertension. We compared BP values derived from PPG signals to cuff-based 24-hour ABPM.
METHODS
Ethical statement
The study protocol was approved by the Institutional Review Board of Seoul National University Hospital (E-2305-064-1431), and all patients provided written informed consent. Information about the study’s objectives, design, and study population was registered on ClinicalTrial.gov (NCT06084065), adhering to the principles outlined in the Declaration of Helsinki (2013).
Participants and data collection
A total of 40 patients were enrolled in this study, and 33 patients were included in the final analysis. This exclusion was due to protocol violations (2 participants), consent withdrawal (1 participant), technical issues (2 participants), and calibration errors (2 participants).
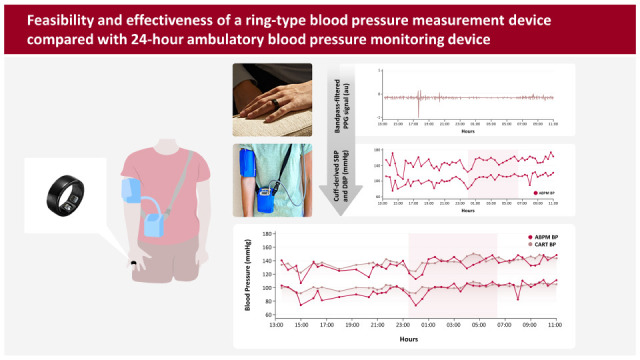
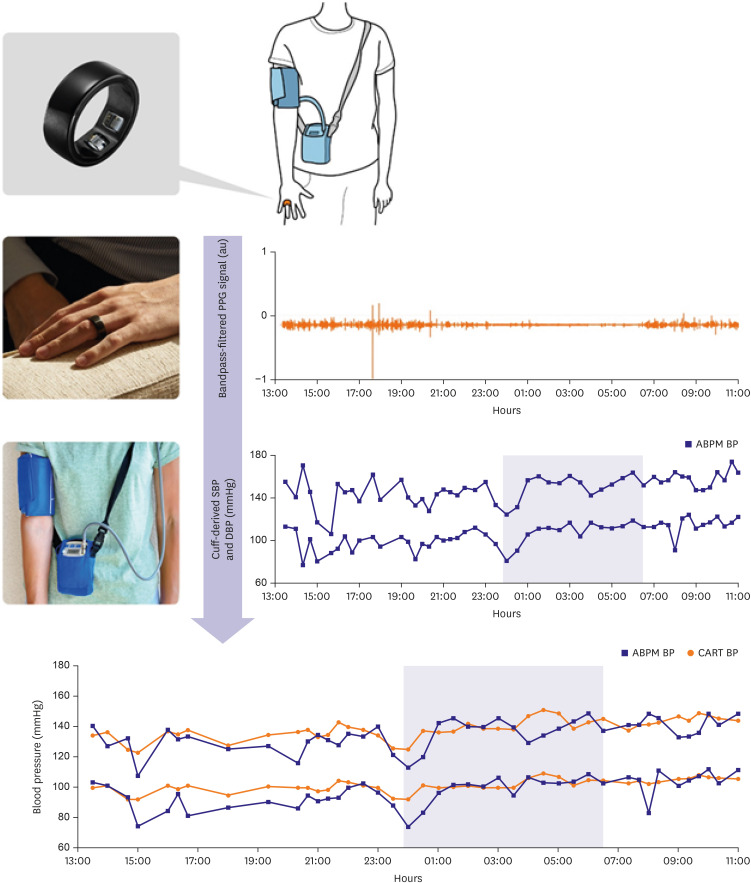
As illustrated in Figure 1, Supplementary Figures 1 and 2, each subject wore both a finger-worn type cuffless BP measurement device, the CART-I Plus (Sky Labs Inc. Gunpo, Korea), and ABPM devices on the same arm, which was their non-dominant arm, for approximately 24 hours. The CART-I Plus recorded 15-second PPG signals at 1-minute intervals, while the ABPM measured BP at 20-minute intervals during the day and 30-minute intervals at night. BP estimates from CART-I Plus were aligned with the corresponding ABPM measurements.
Data preprocessing
During data preprocessing, the 15-second PPG signals from CART-I Plus were transformed into 10-second signals, with noise eliminated through filtering. These refined signals were evaluated using a signal quality algorithm. If deemed valid by the algorithm, they were used to estimate BP values through a BP algorithm.17) A corresponding BP value was generated for each ABPM reading, enabling comparison with the ABPM device.
In our study, both the CART-I Plus and ABPM devices were worn on the same arm, specifically the non-dominant arm. Obtaining a simultaneous BP estimate from CART-I Plus at the exact time point of the ABPM device is unattainable, because cuff inflation occluded blood flow to the PPG detection point. This challenge arises due to the inherent differences in measurement intervals and timing between ABPM and CART-I Plus, compounded by the cuff inflation/deflation of the cuff during BP measurements. Thus, we derived a representative BP value from CART-I Plus estimates gathered at 1-minute intervals within a 15-minute time frame surrounding each ABPM readings.
It is recognized that cuff inflation on the arm can lead to an instantaneous rise in BP.18) Specifically, in hypertensive patients, cuff inflation triggers a reactive increase in BP.18) To mitigate the impact of these instantaneous rises, the third quartile value was utilized as the representative metric. Data with fewer than three BP estimates from CART-I Plus within the 15-minute timeframe were excluded from the analysis. This exclusion criterion applied to 26% of the total readings (520 out of 2,004). For daytime data, 31% (485 out of 1,548) were excluded, and for nighttime data, 8% (35 out of 456) were excluded. The higher exclusion rate during daytime data is attributed to increased motion, leading to a greater number of exclusions based on poor signal quality.
Calibration
Ambulatory blood pressure monitoring calibration
To address potential measurement inconsistencies among devices, our analysis relied on BP values calibrated with ABPM. This approach involved pairing each participant’s 24-hour ABPM BP readings with the corresponding PPG signals for ABPM calibration. To ensure consistency and avoid overestimation, we applied strict criteria when selecting calibration data for ABPM across all participants. The selection was based on the characteristics of the actual calibration setting, characterized by stable BP readings and high-quality signals. Since ABPM acquires readings at 20-minute intervals, using multiple BP measurements for calibration could inadvertently inflate accuracy. To mitigate this, we selected data from a specific time point characterized by consistent BP conditions for the ABPM calibration. As previously mentioned, our criteria for selecting calibration data for ABPM were based on the real-world calibration environment, focusing on data within 10–20% range of each subject's 24-hour BP distribution.
As previously mentioned, selecting calibration data hinges on securing stable BP readings and ensuring high-quality signals. Given the dynamic nature of 24-hour ambulatory BP monitoring, maintaining a static state for measurement control proves challenging. However, the lower BP values within the 24-hour profile often exhibits comparatively more stable BP and better signal quality. Consequently, calibration data were deliberately chosen from the lower 10–20% BP range for each subject. This approach excluded the bottom 0–10% of readings to mitigate potential outliers and emphasized the subsequent 10% segment (from the bottom 10% to the 20%). From the ABPM readings and their corresponding PPG signals within this range, we selected a specific data pair, prioritizing the PPG signal that not only passed our signal quality algorithm but also exhibited the highest auto-correlation.
Electronic BP monitoring device calibration
Calibration of the CART-I Plus was also performed using a standard electronic BP monitoring device (Omron HEM-7080; Omron, Kyoto, Japan). This calibration followed the ISO 81060-2:2018 ‘5.2.4.1 Same arm sequential method.’19) The calibration process included two data collection rounds, capturing both PPG signals and corresponding BP readings from the cuff-type BP device. If signal quality was deemed inadequate or if there was a significant discrepancy in BP values between the two rounds, recalibration was executed.
Data analysis
According to the ISO 81060-2:2018, the comparison involves mean difference of test versus reference BP measurements ≤5 mmHg with SD ≤8 mmHg for systolic and diastolic BP.19) In addition, European Society of Cardiology (ESH) recommends assessing correlation (correlation coefficient ≥0.70) between test awake-asleep BP changes and reference awake-asleep BP changes when comparing with ABPM. Our data analysis was aligned with international standards.20)
Statistical analyses were conducted using R version 4.2.2, with a significance threshold set at p<0.05. Mean BP values were compared across 24-hour, daytime, and nighttime periods for individual participants. Outcomes were expressed as mean error and standard deviation. The correlation between CART-I Plus and ABPM measurements was determined using Pearson correlation coefficients, and the agreement between the two methods was visualized using Bland-Altman plots.
RESULTS
Patients’ characteristics
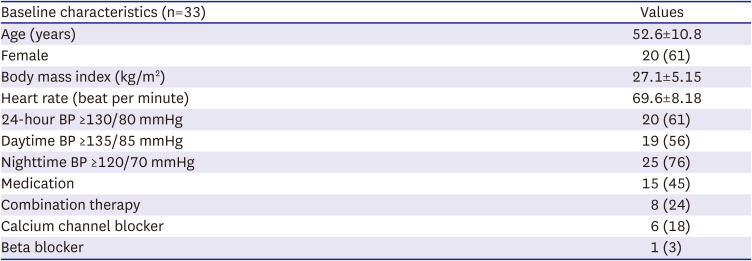
The participants, predominantly female (61%), had an average age of 52.6±10.8 years and a mean body mass index of 27.1±5.15 kg/m2. The analysis revealed that 61% had a 24-hour BP ≥130/80 mmHg, and a significant proportion also exceeded the thresholds for daytime and nighttime BP. Nearly half (45%) were on medications, including combination therapy, calcium channel blockers, and beta blockers, highlighting a pre-existing condition of cardiovascular management among the participants (Table 1).
Table 1
Characteristics of the study patients
Comparison of measured blood pressure between CART-I Plus and ambulatory blood pressure monitoring
ABPM recorded 24-hour, daytime, and nighttime SBP/DBP values of 129.7±11.7/84.4±11.2, 131.9±11.6/86.3±11.1, and 124.5±13.6/80.0±12.2 mmHg, respectively. In contrast, CART-I Plus measurements were 131.4±14.1/81.1±12.0, 132.7±13.9/81.9±11.9, and 128.7±14.6/79.3±12.2 mmHg for these respective periods (Table 2). Table 3 details the mean differences in SBP/DBP between ABPM and CART-I Plus, showing variations of 1.74±6.69/−3.24±6.51 mmHg over the 24-hour, 0.75±7.44/−4.41±7.42 mmHg during daytime, and 4.15±6.15/−0.67±5.23 mmHg during nighttime. These data highlighted the nuanced disparities and agreements in BP readings acquired through the two distinct methodologies.
Table 2
Comparison of average BP between ABPM and CART-I Plus
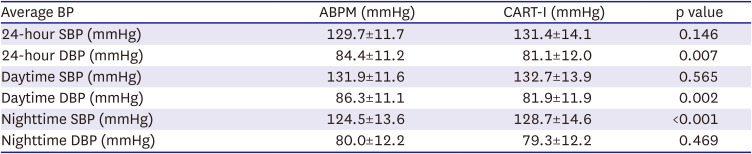
Table 3
Agreement of blood pressure measurements between the 24-hour ambulatory BP monitoring and CART-I Plus

| BP | SBP (mmHg) | DBP (mmHg) |
|---|---|---|
| 24-hour | 1.74±6.69 | −3.24±6.51 |
| Daytime | 0.75±7.44 | −4.41±7.42 |
| Nighttime | 4.15±6.15 | −0.67±5.23 |
| Change | −3.39±5.86 | −3.74±4.72 |
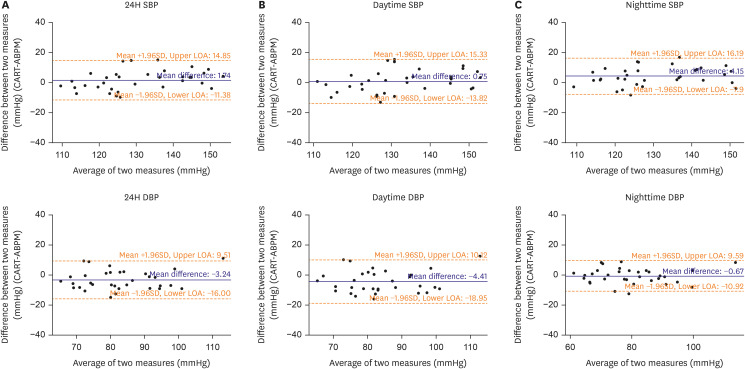
We assessed the mean difference and the 95% limits of agreement (LOA) using Bland-Altman plots, comparing CART-I Plus and ABPM readings for 24-hour, daytime, and nighttime BP on days both devices were worn concurrently (Figure 2). The 24-hour SBP exhibited a mean difference and LOA of 1.7 (−11.4; 14.9) mmHg. For daytime SBP, these values were 0.8 (−13.8; 15.3) mmHg, and for nighttime SBP, they were 4.2 (−8.9; 16.2) mmHg. For DBP, a consistent pattern emerged, with the greatest precision observed during nighttime. Specifically, the mean difference and LOA for 24-hour DBP were -3.2 (−16.0; 9.5) mmHg, daytime DBP showed −4.4 (−19.0; 10.1) mmHg, and nighttime DBP demonstrated −0.7 (−10.9; 9.6) mmHg.
Figure 2
Analysis of agreement between CART-I Plus and ABPM for 24H Blood Pressure Monitoring. (A) Bland-Altman plot illustrating the agreement for SBP and DBP during 24H. (B) Bland-Altman plot showcasing the agreement for SBP and DBP during the daytime. (C) Bland-Altman plot highlighting the agreement for SBP and DBP during the nighttime. In each plot, the dashed line indicates the mean difference (bias) between the two devices, while dotted lines mark the 95% LOA.
24H = 24-hour; ABPM = ambulatory blood pressure monitoring; DBP = diastolic blood pressure; LOA = limits of agreement; SBP = systolic blood pressure.
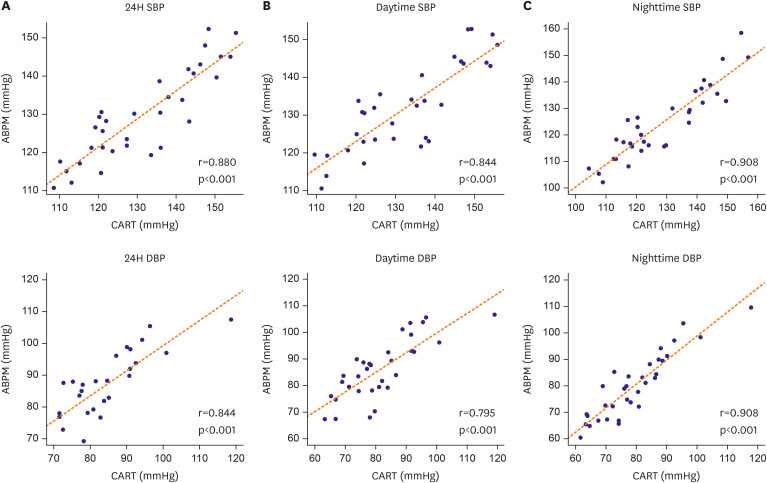
Both devices demonstrated strong correlations in 24-hour, daytime, and nighttime BP measurements (Table 4, Figure 3). The correlation coefficient for 24-hour SBP was 0.880, for daytime SBP it stood at 0.844, and for nighttime SBP, it was 0.908 (all with p<0.001). Similarly, for DBP, strong correlations were observed: 0.844 for 24-hour, 0.795 for daytime readings, and 0.908 for nighttime readings (all p<0.001).
Table 4
Correlation between 24-hour ambulatory BP monitoring and CART-I Plus

| BP | SBP (mmHg) | DBP (mmHg) | ||
|---|---|---|---|---|
| r | p value | r | p value | |
| 24-hour | 0.880 | <0.001 | 0.844 | <0.001 |
| Daytime | 0.844 | 0.795 | ||
| Nighttime | 0.908 | 0.908 | ||
| Change | 0.725 | 0.750 | ||
Figure 3
Comparative analysis between CART-I Plus and ABPM for 24H blood pressure monitoring. (A) Scatter plot illustrating the relationship for SBP and DBP over the entire 24H span. (B) Scatter plot showcasing the correlation for SBP and DBP during daytime hours. (C) Scatter plot highlighting the correlation for SBP and DBP taken at nighttime. The solid line in each plot represents the linear regression best fit, while the dashed line demonstrates the line of identity.
24H = 24-hour; ABPM = ambulatory blood pressure monitoring; DBP = diastolic blood pressure; SBP = systolic blood pressure.
Daytime-nighttime change of measured blood pressure between CART-I Plus and ambulatory blood pressure monitoring
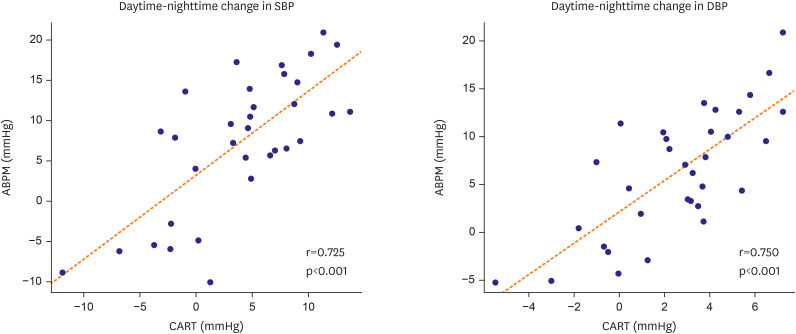
The CART-I Plus showed a diminished variance between daytime and nighttime BP readings, with SBP and DBP differences of −3.4±5.9 and −3.7±4.7 mmHg, respectively, offering a contrast to traditional ABPM readings (Table 3). A strong correlation was also observed in the BP transition from daytime to nighttime between the CART-I Plus and ABPM, as evidenced by correlation coefficients of 0.725 for SBP and 0.750 for DBP, both significant at p<0.001 (Table 4, Figure 4). These findings indicate the CART-I Plus’s reliability and potential clinical utility, suggesting it as an effective tool for more stable and consistent BP monitoring across different times of the day.
Tracking 24-hour blood pressure changes with electronic blood pressure monitoring device calibration
Comparing average 24-hour, daytime, and nighttime SBP and DBP differences between the CART-I Plus calibrated with the electronic BP monitoring device and ABPM (Supplementary Table 1), a high level of agreement was observed. The differences in mean 24-hour, daytime, and nighttime SBP were −0.9±7.6 mmHg, −2.0±8.0 mmHg, and 1.7±8.3 mmHg, respectively. For DBP, the differences for 24-hour, daytime, and nighttime readings were −3.4±7.9 mmHg, −4.6±7.7 mmHg, and −0.7±9.0 mmHg, respectively. Consistent with the results from ABPM calibration, the CART-I Plus calibrated with the electronic BP monitoring device also indicated a diminished change between daytime and nighttime for both SBP and DBP (−3.7±6.0 mmHg and −3.9±4.8 mmHg, respectively) when compared to ABPM.
DISCUSSION
This study evaluated the performance of the ring-type cuffless BP device, CART-I Plus, in monitoring 24-hour BP changes in comparison to conventional out-of-office cuff BP measurement techniques. The CART-I Plus device generally recorded slightly higher SBP values and marginally lower DBP values across different periods in comparison to ABPM. Bland-Altman plots indicated a commendable agreement between CART-I Plus and ABPM, with significant correlation coefficients evident across 24-hour, daytime, and nighttime periods for both SBP and DBP measurements. A similar degree of concordance was identified when CART-I Plus was calibrated utilizing electronic BP monitoring device. This study results shed light on the approach to comparing ring-type cuffless BP monitoring with ABPM. The methodology for comparing wearable devices with ABPM has been a subject of debate, but the recently released ESH Recommendation16) provides guidelines in this regard. According to this recommendation, the initial findings from wearable cuffless BP studies suggest that a PPG-based ring-type BP device could potentially serve as a substitute for ABPM. The demonstrated efficacy of the ring-type BP device in this study, along with anticipated results from follow-up studies, heralds a new paradigm in continuous and 24-hour BP monitoring.19)
In a study comparing a wrist-worn cuffless BP device to ABPM,20) Bland-Altman analysis revealed a mean difference and LOA that closely align with our results. However, in that study, the correlation between two devices were not significant for SBP and DBP. Another investigation that compared a PPG-based BP watch to ABPM found substantial correlations between the two modalities, echoing our data.21) Receiver operating characteristics (ROC) analysis in this study produced an area under the curve (AUC) of 1 for both SBP and 24-hour BP measurements, reinforcing the potential utility of PPG-based cuffless BP systems in hypertension diagnostics. Yet, in another study22) using a PPG-integrated smartwatch, the ROC curves depicted lower AUC values for hypertension diagnosis. CART-I Plus demonstrated improved accuracy compared to previous studies,20)22)23)24) and its unique ring-type design offers user-friendliness and integration into daily routines.
In a study25) that utilized the CART-I Plus, calibrated via manual auscultation (S.W. PARK., in press), a marginal difference was observed between the CART-I Plus and the traditional cuff-based device, demonstrating remarkable accuracy. Our analysis further corroborated the precision of the CART-I Plus, aligning it with both ABPM and electronic BP monitoring device metrics. It is essential to consider that oscillometric BP devices can yield varying results depending on the manufacturer, emphasizing the importance of selecting an appropriate calibration instrument.26) Recent recommendations advocate for a minimum 24-hour gap between calibration and the initiation of ABPM to enhance accuracy.16)
This study has some limitations, including the relatively small sample size and differences in the calibration method compared to recent recommendations. However, it provides valuable insights into the accuracy and potential clinical utility of the CART-I Plus device for BP monitoring.
In summary, the CART-I Plus, a ring-type cuffless BP measurement device, exhibited commendable accuracy in estimating BP using PPG signals across different time periods when compared to traditional 24-hour ABPM. Its innovative design and proficient data capture mechanisms make it a significant advancement in BP monitoring, with potential for future integration into clinical settings, particularly for monitoring nocturnal hypertension. The ease of use, and the ability to capture continuous, real-world data underscore the transformative potential of cuffless BP monitors in enhancing the precision, patient’s adherence, and convenience of BP management. As healthcare systems increasingly embrace digital solutions, the clinical implications of cuffless monitors extend beyond traditional monitoring methods, offering a promising avenue for more patient-centric and data-driven hypertension care.
 XML Download
XML Download