

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Liver resection is the primary curative treatment for hepatobiliary malignancies. Advancements in surgical techniques and anesthetic care have improved the outcomes of liver surgery in recent decades [1]. The perioperative mortality rate of liver resection, which previously exceeded 10%, has decreased by 2%–4% [23]. Among the factors associated with the prognosis of liver resection, blood loss during liver resection is an important factor associated with postoperative complications, long-term outcomes, and survival [456]. Despite efforts to minimize blood transfusion during liver surgery, the perioperative transfusion rates remain high, ranging from 9% to 65%, and exhibit considerable variation between institutions, types of surgery, or patient characteristics [47].
Various strategies have been investigated to reduce perioperative blood loss and its unfavorable sequela [4]. Although patient blood management (PBM), a multidisciplinary patient-centered approach focusing on the minimization of blood product use and improvement of patient outcomes, has been introduced as the standard of care for transfusion medicine [8], the concept of PBM was introduced to liver surgery relatively late compared to other surgeries owing to several specific concerns regarding liver resection [3]. However, the importance of reducing blood transfusion through PBM has been raised [39]. Individual studies in Korea showed transfusion rates of 29% for laparoscopic hepatectomies, 24.5% for laparoscopic major liver resections, and 9% for left hemihepatectomies [9101112], which were comparable to those in previous studies. However, other types of surgery, such as hip arthroplasty or knee arthroplasty, showed a very high transfusion rate compared to other countries despite a decreasing trend [1314]. The excess demand for blood compared with availability by blood donation has been an important issue in the Korean blood management system; thus, in addition to encouraging blood donation and research on blood resources, the minimization of transfusion is required [15].
In combination with high transfusion rates during liver surgery in general and higher transfusion rates for certain types of surgery (hip arthroplasty or knee arthroplasty) in Korea than in other countries, this study aimed to review the blood transfusion rate during liver resection by country to prepare the basis for PBM policy.
METHODS
Data sources and search strategies
This systematic review was performed in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines [16]. Since only previously published literature was included as study materials, ethical approval was not required for this review, and an exemption was granted by the Institutional Review Board of the Hanyang University College of Medicine (No. HYUIRB-202308-004). To assess the most recent evidence, we systematically searched articles published in PubMed, Embase, and Web of Science over the past 3 years as of December 2022. The first search was conducted in March 2023, and the search period was from January 1, 2020, to December 31, 2022.
A combination of Medical Subject Headings (MeSH) and text words was used for liver resection and blood transfusion. The applied search terms were ((((((“transfusion”[Title/Abstract] AND “liver resection”[Title/Abstract]) OR “Hepatectomy”[Title/Abstract]) NOT “systematic review”[Title]) NOT “a review”[Title]) NOT “Meta-Analysis”[Title]) NOT “review”[Title]) AND ((english[Filter]) AND (2020:2022[pdat])).
Inclusion and exclusion criteria
The study population included patients who underwent liver resection, and the search was limited to studies published in English with no age restrictions. Randomized and non-randomized (retrospective and prospective cohort) studies were considered. The exclusion criteria included types of research designs such as multinational institutional studies, editorials, case reports, reviews, and cases where the principal diagnosis was unrelated to the liver (stomach cancer, pancreatic cancer, colon cancer, etc.). Studies involving liver resection due to metastatic cancer to the liver or recurrent liver resection and liver transplantation-related resection of the donor were also excluded. All types of hepatectomy and blood product transfusions were included.
Data collection
One researcher screened the titles and abstracts, and 2 independent researchers conducted a full-text review. Disagreements between the 2 researchers were resolved through discussions. Following the study selection process, data from the identified studies were independently extracted and entered into a predesigned spreadsheet by 2 researchers. The outcomes of interest included transfusion rate by country, primary cause of liver resection (benign liver disease, hepatocellular carcinoma [HCC], and intrahepatic cholangiocarcinoma), surgical method open surgery and minimally invasive surgery (MIS; which included all of laparoscopic surgery, minimally invasive liver resection, and robotic surgery), and cultural area (Korea, Asian countries other than Korea, and Western countries).
Quality assessment
Two researchers independently assessed the methodological quality of the studies. For observational studies, the Risk of Bias Assessment Tool for Non-randomized Studies (RoBANS) was used. The RoBANS covers 6 areas: participant selection, confounding variables, exposure measurement, blinding of outcome assessments, incomplete outcome data, and selective outcome reporting. Each area of the RoBANS tool was judged as “low,” “high,” and “unclear” [1718]. Quality assessment of randomized comparative clinical trials was performed using the risk of bias (RoB) tool. This tool evaluates 5 domains of bias: the randomization process, deviations from intended interventions, missing outcome data, measurement of the outcome, and selection of the reported results. The RoB for each of the 5 domains and overall was described as low, with some concerns, or high [1920].
Analysis
Descriptive results regarding the overall transfusion rate and by country, primary cause of liver resection, surgical method, and cultural area are summarized as the average transfusion proportion. The proportion of transfusions in each study was meta-analyzed using fixed- or random-effects models. Study heterogeneity was assessed using the Q-test and I2 test; if there were significant heterogeneities, a random-effects model was applied; otherwise, a fixed-effects model was applied. The pooled odds ratios (ORs) and 95% confidence intervals (CIs) comparing the blood transfusion rates between open surgery and MIS were estimated and stratified by cultural area. In comparing blood transfusion rates between open surgery and MIS in terms of pooled OR, to increase the comparability, only studies presenting transfusion rates in open surgery and MIS within the same study were considered. Publication bias was evaluated using funnel plots and Egger’s and Begg’s tests. All analyses were performed using RevMan 5.3 (The Nordic Cochrane Center).
RESULTS
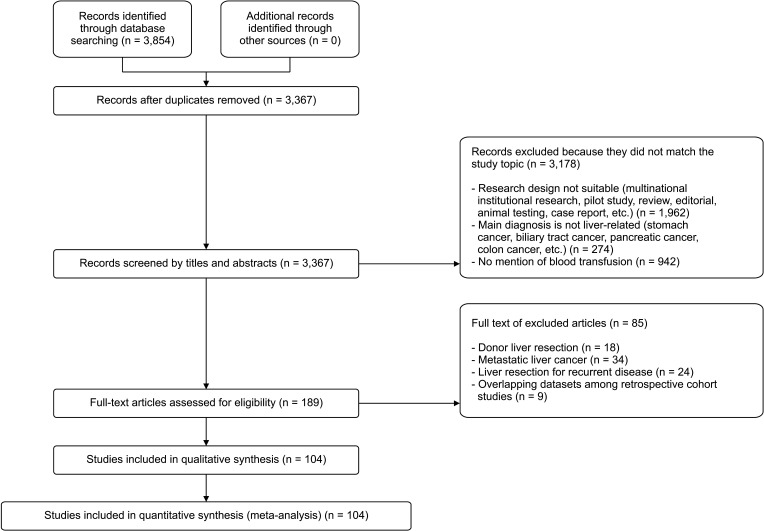
The initial search identified 3,854 articles (Fig. 1). After screening titles, abstracts, and quick reviews of the manuscript to identify transfusion-related outcomes not described in the abstract, 189 eligible studies were included in the in-depth full-text review. Finally, 104 papers were included after a full-text review by 2 independent researchers. See Supplementary Table 1 for a summary of the selected literature. A total of 103,778 patients who underwent liver resection across 104 studies met the inclusion criteria. Among the included papers, 3 clinical trials [212223] and 101 retrospective cohort studies [24252627282930313233343536373839404142434445464748495051525354555657585960616263646566676869707172737475767778798081828384858687888990919293949596979899100101102103104105106107108109110111112113114115116117118119120121122123124] were identified, and 41 [222325262733343536424849505152536466676975848586878890919395104106114117118119120121122123124], 12 [29373839414365798099100103], and 14 [2455637273778198102107108109110115] studies were conducted in China, Korea, and Japan, respectively. Studies conducted in these 3 countries accounted for 63.2% of all included studies (Table 1). Supplementary Table 2 and Supplementary Figs. 1, 2 show the biased assessment of the included studies.
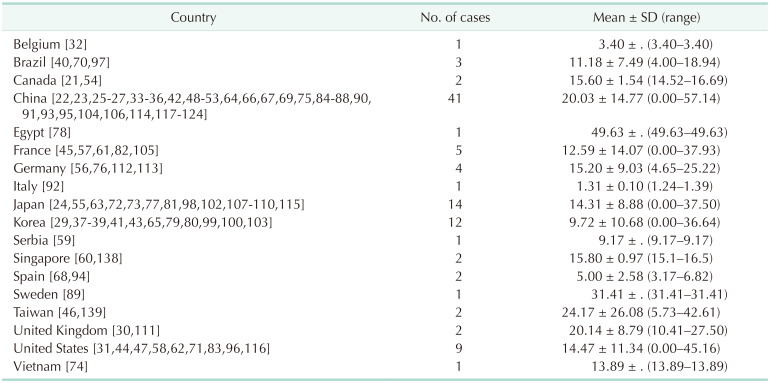
According to a meta-analysis, the average transfusion rate in all studies was 16.53%, with an individual study ranging from 0.00% [2941458290110124] to 57.14% [52]. When divided by the countries where the study was conducted, Egypt had the highest blood transfusion rate (49.63%, Table 1), followed by Sweden, Taiwan, the United Kingdom, and China, with a perioperative transfusion rate of more than 20%. However, of these countries with high transfusion rates, except China, the included studies were only 1 or 2.
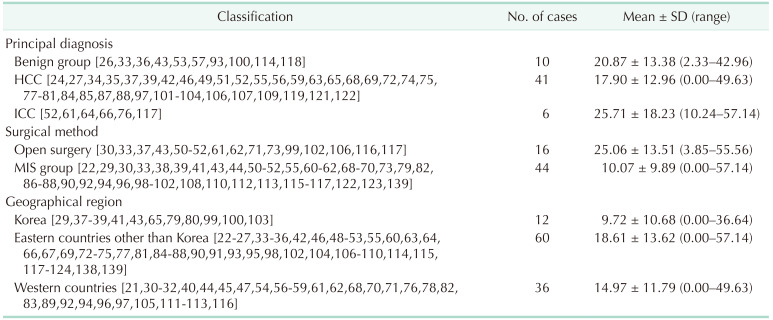
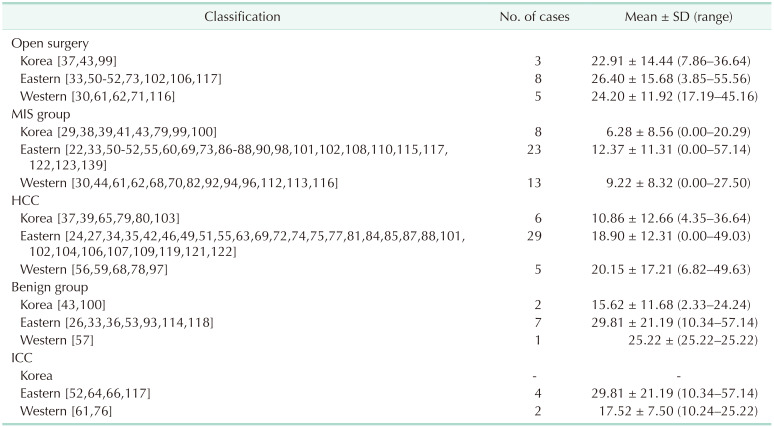
Table 2 shows transfusion rates by primary diagnosis, surgical methods, and cultural area. When stratified by primary diagnosis, the transfusion rate for the patients with intrahepatic cholangiocarcinoma was 25.71% (range, 10.24%–57.14%), which was higher than those of HCC or benign liver diseases (mean transfusion rate of 17.90% and 20.87%, respectively). Open surgery had a higher transfusion rate than MIS (25.06% vs. 10.07%). The transfusion rate in Korea was lower than those reported in Western and Eastern countries other than Korea (9.72%, 14.97%, and 18.61%, respectively). The range of blood transfusion in Korea was narrow (range, 0.00%–36.64%). When comparing the blood transfusion rate during liver resection in Korea with those in Western and Eastern countries and subdividing it into primary diagnosis and surgical methods, we observed lower blood transfusion rates in all areas (Table 3).
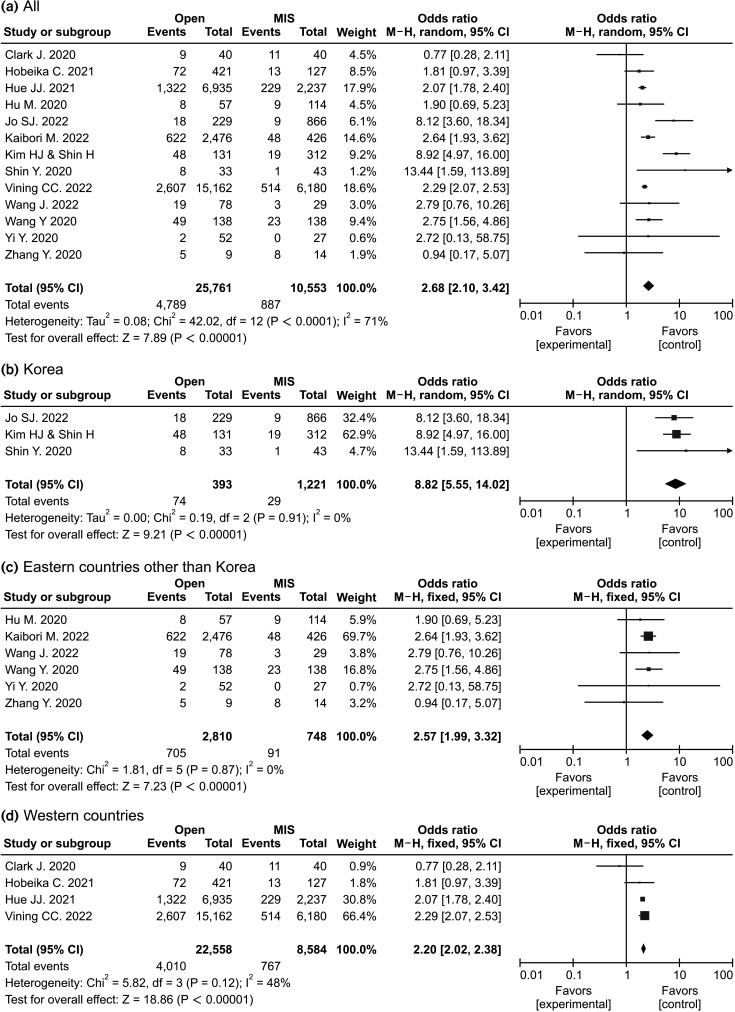
When the probability of transfusion in open surgery was compared with that in MIS, the number of studies included in pooled OR decreased because we included only studies presenting transfusion rates in both open surgery and MIS within the same study. The OR for transfusion was 8.82 (95% CI, 5.55–14.02) in Korea, 2.57 (95% CI, 1.99–3.32) in Asian countries other than Korea, and 2.20 (95% CI, 2.02–2.38) in Western countries (Fig. 2).
DISCUSSION
Liver resection is the curative treatment for malignant and benign liver diseases as well as metastatic cancers of the liver. Despite a decreased transfusion rate during liver resection, transfusion remains a common intervention during hepatic resection. In this study, between 2020 and 2022, the average transfusion rate during liver resection was 16.20%, a lower transfusion rate than that in other systematic reviews, in which the overall proportion of transfusions was 38.3% [4]. A recent study based on hepatic lobectomies performed between 2011 and 2014 registered in a university consortium showed a transfusion rate of 20%, while another study suggested a transfusion rate of at least 25% following liver resection [125]. Although a direct comparison would yield different results, these results support a decreased transfusion rate. Many previous studies on perioperative transfusion did not restrict conditions associated with liver resection. Although colorectal liver metastasis is one of the main indications for liver resection [126], we excluded patients who underwent liver resection for metastatic carcinoma of the liver because of the very high transfusion rate compared to that with other conditions [127].
Previous studies have focused on the detrimental consequences of transfusion during liver resection, risk factors for transfusion, and strategies to reduce blood loss rather than the transfusion rate itself [4125128129]. We focused on the regional differences in transfusion rates in patients who underwent liver resection. There are large differences in the characteristics of liver disease between Asian and Western countries in terms of causes, etiologies, and clinical characteristics, which could affect the outcomes of liver diseases [130131]. In this study, the rate of blood transfusion in Eastern countries other than Korea was higher than in Western countries regardless of surgical method (open or MIS). However, when stratified by liver resection-associated conditions, the transfusion rates for HCC and benign diseases were lower in Eastern countries than in Western countries. In many Asian countries, hepatitis B is the most common cause of liver diseases, including HCC; however, hepatitis C and alcoholic liver disease are the liver diseases that frequently cause HCC in Western countries [131]. Guidelines for the surgical treatment for HCC in Asian countries are more aggressive than those in Western countries, and liver resection is frequently performed in patients with cirrhosis and portal hypertension, whose coagulation disorder and bleeding tendency are higher [131]. Experience with more frequent surgeries and advancements in technology may explain these results.
Lower blood loss and transfusion rates have been reported in laparoscopic surgery than in open surgery; the OR of transfusion during laparoscopic vs. open surgery was 0.36 [132133]. A more recent meta-analysis of comparative cohort studies showed higher volume loss in major laparoscopic liver resection than in open liver manor resection; however, transfusion rates were comparable between the 2 groups [134]. Improved surgical techniques, such as the Glissonian approach, selective clamping, intraoperative ultrasonography, argon beam coagulation, and staplers, help achieve hemostasis and reduce transfusion [134]. In this study, despite the limited number of included studies to estimate pooled OR, the ORs of the transfusion rate of open surgery compared with those of MIS in Asian and Western countries were 2.57 and 2.20, respectively, which were comparable to the OR of previous meta-analyses comparing laparoscopic vs. open surgery [132133]. In Korea, only 3 studies presenting transfusion rates in both MIS and open surgery were included during the study period, and the OR was 8.8. When comparing the number of MIS and open surgeries included in the estimation of pooled OR, the number of MIS was higher than that of open surgery in Korea. However, the number of MIS was lower than that of open surgery in Eastern countries other than Korea and Western countries. Therefore, the improved techniques in Korea could be expected to yield a wide gap in transfusion rate between MIS and open surgery.
Among Asian countries, the transfusion rate of open surgery in Korea was lower than that in other Asian countries, irrespective of diagnosis and surgical methods. When stratified by surgical method, the differences in transfusion rate during open surgery in Korea, Eastern, and Western nations were minimal (approximately 25%); however, the differences in transfusion rate during MIS were significantly lower in Korea than in other Eastern and Western countries. A multicenter study regarding laparoscopic liver resection from 2001 to 2011 showed an intraoperative transfusion rate of 24.5% [11]; thus, after 2011, a significant decrease in transfusion rate during MIS in Korea was identified. Korea has implemented strict blood transfusion management since establishing blood transfusion guidelines in 2009 [135]. Accordingly, blood transfusions for liver disease among all diseases in Korea decreased from 2.94% in 2009 to 2.71% in 2018 [136]. This may be explained by the fact that in Korea, blood transfusion rates are higher in women than in men [136], and liver disease is more common in men than in women [137]. Additionally, it appears to result from efforts to reduce massive bleeding, including advances in laparoscopic liver resection techniques, selective hepatic blood flow blockage during hepatectomy, low central venous pressure maintenance, and sophisticated liver parenchymal dissection.
This study has several limitations. Primarily, although we performed a subgroup analysis according to the primary diagnosis and surgical methods, inherent heterogeneity between studies existed. Within the HCC group, the size and number of tumors may differ, as well as the underlying characteristics of the patients; thus, these heterogeneities might affect perioperative transfusion. Additionally, the confounding variables considered in each study differed. To identify the transfusion rate in recent studies, we restricted the articles included in the meta-analysis to those published within 3 years, but there would be changes in surgical and adjuvant therapies that might affect blood loss and transfusion within the time period. All included studies were observational; thus, there is a possibility of selection bias, publication bias, or bias due to confounding factors. In addition, preoperative procedures that attempted to reduce blood loss and transfusion were not assessed.
In this study, we analyzed the global transfusion rate during liver resection in recent studies. Although there is evidence of a decreasing prevalence of perioperative blood transfusion during liver resection, transfusion remains a common intervention. In addition to patient diagnosis and surgical methods, differences in culture and medical environment according to race and geographic location also affect blood transfusion rates during liver resection. Therefore, nationwide PBM strategies should be implemented to ensure successful PBM results.
 XML Download
XML Download