

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Hemangioblastoma (HB) is a rare central nervous system (CNS) tumor commonly found in the cerebellum, brain stem, and spinal cord [1]. It is generally regarded as a benign, slow-growing, non-metastasizing neoplasm [12]. Sporadic HB is usually solitary and accounts for 70% of cases. In contrast, HB with manifestations of von Hippel-Lindau (VHL) disease is often multifocal and accounts for 30% of cases [1]. Sporadic HB occasionally shows local recurrences; however, dissemination recurrence is extremely rare [13]. Here, we report a patient with sporadic supratentorial HB, who exhibited whole neuroaxis dissemination for more than two decades.
CASE REPORT
A 68-year-old female patient presented with severe radiating pain in the right leg. Gadolinium (Gd)-enhanced lumbar spine MRI showed an intradural mass (2.5 cm in diameter) at the L4 level (Fig. 1A). Additional whole-spine MRI showed multiple small masses at the cervical and thoracic spines (Fig. 1B).
The patient underwent spinal surgery and a total removal of the intradural mass (July 2022). During surgery, it was found that the mass was related to neither the dura matter nor the adjacent nerve rootlets. However, interestingly, the final histological diagnosis was HB. Histopathologically, the tumor exhibited analogous histological features, showing irregularly formed vessels interspersed with large stromal cells exhibiting hyperchromatic nuclei (Fig. 1C). Notably, the tumor cells exhibited limited immunopositivity for alpha-inhibin (Fig. 1D) but demonstrated robust immunopositivity for epidermal growth factor receptor (EGFR) (Fig. 1E).
The postoperative clinical course was uneventful, and the previous radiating pain disappeared. Evaluation for VHL disease, including systemic radiological and ophthalmological examination, showed negative results.
Review of past brain surgery and multiple gamma knife radiosurgery history
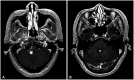
In December 2000 (22 years ago), the patient had undergone craniotomy and a subtotal removal of a large solid tumor in the third ventricle extending to the lateral ventricles (Fig. 2). As per the medical records, a profound bleeding episode occurred during surgery, and the pathological diagnosis was angioblastic meningioma with hemorrhage. Immunohistochemistry revealed positive vimentin and factor VIII staining and negative HMB45 staining. However, the findings were limited by the extent of the available information. Clinically, after the first brain tumor resection, the patient was severely disabled due to left hemiplegia, and the Karnofsky performance score (KPS) was 60.
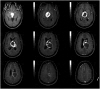
At 14 years after the brain surgery, Gd-enhanced axial brain MRIs (April 2014) showed two newly developed tumors in the cerebellomedullary cistern (Fig. 3A) and fourth ventricle (Fig. 3B). The first gamma knife radiosurgery (GKRS) was performed for them; the tumor volumes were 0.57 cm3 and 0.19 cm3, respectively, and the prescription radiation doses were 13.0 Gy and 13.5 Gy, respectively (April 2014). After 5 years, the second GKRS was performed for three newly developed tumors, which were located in the cerebellopontine cistern, ambient cistern, and lateral ventricular wall. Two-fraction GKRS was performed with a prescription dose of 2×7.6 Gy (December 2019). Two years later, the third GKRS was performed for a newly developed tumor near the right optic nerve in the basal cistern. The tumor volume and the prescription radiation dose were 0.71 cm3 and 12 Gy, respectively (July 2021). Until this point, we managed this patient as a recurred and disseminated ventricular meningioma patient.
Pathological review of the first specimen from December 2000
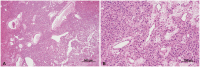
The original tissue specimen in 2000 was reevaluated following two instances of recurrence. Microscopic examination at low magnification revealed irregularly dilated blood vessels and extensive hemorrhage (Fig. 4A). Upon closer inspection at high magnification, vacuolated stromal cells characterized by large hyperchromatic nuclei and an eosinophilic foamy cytoplasm were identified amidst well-developed blood vessels (Fig. 4B). Based on a biopsy review, the presence of the primary tumor was consistent with the histological diagnosis of HB.
Second spinal surgery and posterior fossa surgery
Six months after the first spinal surgery (February 2023), follow-up whole-spine MRI showed the progression of all spinal tumors, and the tumor at the T9 level demonstrated a severe mass effect on the spinal cord (Fig. 5A). The patient underwent a second spinal surgery and gross total removal with thoracic midline myelotomy. The location of the tumor was in the central canal of the thoracic spinal cord, and the histopathological diagnosis was HB, which was the same as in the first spinal surgery. The postoperative course was uneventful, and the patient’s neurological status remained unchanged.
Three months after the second spinal surgery (May 2023), the patient underwent suboccipital craniotomy due to the progression of the tumor in the right cerebellopontine angle (Fig. 5B). The tumor severely compressed the brain stem, which was subtotally removed.
In the subsequent recurrence, there were prominent tumor cells characterized by a clear cytoplasm and delicate fibrovascular septae (Fig. 5C). Immunohistochemical analysis revealed positive staining for alpha-inhibin (Fig. 5D) and EGFR (Fig. 5E). This was the fourth diagnosis of HB for this patient.
DISCUSSION
The dissemination of sporadic HB is very rare, and less than 20 patients have ever been reported [14567891011121314]. Most of them had a solid cerebellar HB as a primary tumor, and more than three-fourths of cases showed no association with VHL disease [23481415161718192021]. However, thus far, there has been no report of the dissemination of a supratentorial HB.
Two decades ago, the patient was diagnosed with an angioblastic meningioma. However, the diagnosis may be incorrect considering that the origin was the third ventricle. We reviewed the histopathological specimen from the first surgery in 2000 and concluded that the diagnosis was supratentorial HB. The incorrect diagnosis may be explained as follows: 1) the immunohistochemical findings of this tumor could be the same as those of HB; 2) at the time of pathological examination, due to blood clots caused by hemorrhage, accurate diagnosis could be difficult; and 3) when diagnosing the tumor, both the ventricular origin of the tumor and the rarity of the supratentorial HB could not be considered [2223].
Interestingly, there have been several reports of sporadic HB dissemination over an extended period [13]. Bains et al. [1] reported a patient with disseminated CNS HB, and the interval to dissemination was 12 years. They also reviewed previously reported cases, and the interval to dissemination varied from 7 months to 30 years. Kim et al. [3] reported a similar case of disseminated HB into the cauda equina after the removal of a solitary cerebellar HB after a 10-year duration. They suggested that the disseminated HB is an extremely unusual type of recurrence, which is known as hemangioblastomatosis [38141516171819]. They also described the pathophysiology of hemangioblastomatosis as the spillage and spread of tumor cells through the cerebrospinal fluid (CSF) space, which may be an origin of hemangioblastomatosis in patients with a genetic predisposition. They noted that no case of de novo disseminated HB without previous surgery has been reported. Most of the previously reported cases showed multiple mass lesions in the infratentorial area and spinal cord, and the rarity of supratentorial lesions might reflect CSF flow and the effect of gravity, thus supporting the hypothesis of tumor spread through the CSF pathway [3].
Similarly, the case presented here showed a medical history of disseminated sporadic HB, which was disseminated from the supratentorial area to the posterior fossa and finally to the spinal cord via the CSF system over 20 years. We investigated reported cases of disseminated sporadic HB with a duration of 10 years or more (Table 1).
The weak point of this report might be the initial diagnosis (ventricular meningioma) in the old medical records, which we believe was an incorrect diagnosis. There have been reports on the difficulty of differential diagnosis between supratentorial HB and angioblastic meningioma [2223]. Therefore, there may be a high possibility of misdiagnosis as ventricular meningioma. Kim et al. [22] reported a VHL patient with meningeal supratentorial HB mimicking angioblastic meningioma. Crivelli et al. [23] also reported a rare case of solid supratentorial HB. They suggested that the difference between angioblastic meningioma and HB is controversial because of the nonspecific radiological findings of these supratentorial uncommon tumors [23]. Therefore, differential diagnosis between supratentorial HB and angioblastic meningioma might be relatively difficult.
In the management of disseminated HB, there is currently no optimal treatment for preventing the progression of dissemination [12]. Chung et al. [2] emphasized that surgeons should be cautious of tumor cell spillage during the initial surgical management of these tumors, and continuous follow-up should be performed for patients, including those who underwent complete removal of the primary HB.
In conclusion, we presented a patient with whole neuroaxis dissemination of a sporadic supratentorial HB with a brief literature review. The involvement of a pathomechanism is highly likely. This report describes the dissemination of a supratentorial HB, which has not been reported previously. Notably, the dissemination from the supratentorial area to the spine took more than 20 years in the presented case. Therefore, physicians should be aware of the possibility of a long latent period for the dissemination of sporadic HB in the CNS after surgery.



 XML Download
XML Download