

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Hodgkin lymphoma (HL), a hematopoietic malignancy, affects lymph nodes throughout the body [123]. While it is a significant malignancy, its progression to the central nervous system (CNS) is remarkably rare, with an incidence of only 0.02% [456]. Primary or secondary lymphomas account for 2.2%–4.0% of all brain tumors [578910]. In the spectrum of CNS lymphomas, diffuse large B-cell lymphoma (DLBCL) is the predominant histological subtype, comprising an estimated 90%–95% of cases [7810]. Burkitt lymphoma, T-cell lymphoma, and HL each have frequencies that are comparable to each other but are significantly rarer than DLBCL [11]. Of these, our case specifically focuses on HL. To gain deeper insight into these cases, we conducted a detailed literature review spanning from 1980 to 2023, focusing on intracranial HL (IC-HL) cases [91213141516171819202122232425262728293031323334353637383940414243444546]. Through our literature review and understanding of our case, our goal is to emphasize the key differences between DLBCL and HL.
Go to : 
CASE REPORT
A 27-year-old male patient, with a known history of HL, presented with gait disturbance. A brief summary of his HL history is as follows. Three years ago, he presented with persistent high fever and weight loss. Imaging revealed systemic lymphadenopathies in the axillary, neck, and mediastinal regions, as well as multifocal osseous lesions. A diagnostic biopsy from a cervical lymph node, coupled with a bone marrow assessment, confirmed a diagnosis of classic HL, lymphocyte-rich variant, at stage IVXB with documented bone marrow involvement. After confirming the diagnosis, the patient underwent serial chemotherapy regimens according to the National Comprehensive Cancer Network (NCCN) guideline [4748]. Initially, the patient underwent two cycles of ABVD (adriamycin, bleomycin, vinblastin, dacarbazine), which resulted in a partial response. This was followed by four cycles of BEACOPP (bleomycin, etoposide, adriamycin, cyclophosphamide, vincristine, procarbazine, prednisone). Although this regimen also led to a partial response, disease progression subsequently occurred. The treatment strategy was augmented by two cycles of ICE (ifosfamide, carboplatin, etoposide), but this approach resulted in further disease progression. The patient’s therapy was then adjusted to include four cycles of brentuximab vedotin, which successfully led to the absence of disease in the bone marrow. Further management involved six cycles of GDP (gemcitabine, dexamethasone, cisplatin), achieving a metabolic complete response. The treatment course was concluded with autologous stem cell transplantation.
During follow-up, the patient complained of headaches and nausea, but other than increased size of small lymph nodes at four locations in the neck, no other sites of disease were identified. This prompted an MRI examination. Upon his presentation, a brain MRI revealed a 4.5 cm sized mass lesion in the right occipital lobe with a clear and well-defined margin, showing strong contrast enhancement, with attachment to the dura mater and the superior sagittal sinus (Fig. 1A). Accompanying peritumoral edema was prominent in the right cerebral hemisphere, extending to the thalamus and corpus callosum. This edematous change precipitated both subfalcine and transtentorial herniations (Fig. 1B). Initially, two cycles of high-dose methotrexate combined with steroids were given, assuming CNS involvement of lymphoma in HL. However, both symptoms and follow-up imaging results continued to worsen. Upon further review with MRI, and given the lack of therapeutic response, it became apparent that the possibility of another type of brain tumor different from HL, especially meningioma, had to be considered. Consequently, a craniotomy was scheduled both to reduce the ongoing mass effect and to obtain a biopsy. Before surgery, considering the possibility of a meningioma, an external carotid angiography was conducted. During the angiography, a tumor blush was observed from the distal branch of the occipital artery, leading to feeding artery embolization.
 | Fig. 1Pre- and postoperative MRI findings. A: A contrast-enhanced MRI displaying a lesion measuring approximately 4.5 cm, characterized by a well-defined margin, strong enhancement, and invasion into the dura mater and superior sagittal sinus. B: A T2 FLAIR image illustrating diffuse cerebral edema. C and D: Postoperative T1-enhanced MRI and T2 FLAIR images, respectively, depicting a reduced enhancement of the lesion and a decrease in brain edema
|
A craniotomy was performed for tumor resection. Upon dissecting the dura mater, which showed intense adhesion (Fig. 2A), an extensive fibrotic lesion with a well-defined margin, resembling fibrous meningioma, was identified (Fig. 2B). The tumor was encapsulated, and there was almost no bleeding tendency due to feeding artery embolization. The intraoperative findings were markedly different from the typical characteristics observed during DLBCL surgery, which often presents with soft tissue, unclear boundaries, and a severe bleeding tendency. An intraoperative frozen biopsy revealed an abundance of small, round cells. Macroscopically complete removal of tumor and dural coagulation were done (Fig. 2C and D).

The histopathological examination of the resected tissue revealed mononucleated characteristic Reed-Sternberg cells (Fig. 3A). Immunohistochemical staining demonstrated the cells to be positive for CD30 and CD15 (Fig. 3B and C), while negative for CD20 (Fig. 3D), confirming classic HL. These findings confirmed the diagnosis of systemic classic HL with intracranial involvement [123449].
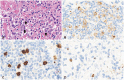 | Fig. 3Histopathological examination (×400 magnification). A: Hematoxylin and eosin-stained tissue section highlighting characteristic mononucleated Reed-Sternberg (Hodgkin) cells (indicated by the arrows). B and C: Immunohistochemical staining reveals positive reactions for CD30 and CD15. D: Immunohistochemical staining for CD20 indicates negative cell reactions.
|
Postoperatively, the patient underwent whole-brain radiotherapy, receiving a total dose of 40 Gy. The latest follow-up revealed MRI indicating no remnant tumor in the previous tumor bed (Fig. 1C and D). Clinically, he demonstrated significant improvement in his gait disturbances and regained his ability to walk independently. Currently, the patient has been in remission for 8 months and remains under close monitoring.
Go to :
DISCUSSION
Between 1980 and 1999, only eight cases of intracranial involvement in HL were reported [1213141516171819]. From 2000 to the time of our current case, 39 additional cases have surfaced [9202122232425262728293031323334353637383940414243444546]. The increasing number of case reports underscores the importance of focusing on IC-HL. While sporadic case reports on IC-HL have emerged over time, a few articles have collected, organized, and published these reports [192021293334354246]. In fact, some cases were missed even within these limited publications. To ensure a complete collection of all cases, we conducted detailed searches on PubMed, Scopus, and Google Scholar. We carefully cross-referenced each case report and attempted to make sure that no cases were missed. Through this process, we gathered all the published literature on IC-HL from 1980 to 2023 and summarized it in Table 1 [91213141516171819202122232425262728293031323334353637383940414243444546]. Based on this table, we aim to highlight some differences between DLBCL and IC-HL.

Table 1
Summary of intracranial Hodgkin lymphoma cases reported in literature from 1980 to 2023
| Study | Yrs | Age (yr) | Sex | Location | HL | Surg | Tx | Follow-up |
|---|---|---|---|---|---|---|---|---|
| Nagashima et al. [12] | 1980 | 60 | M | Falx cerebri | No | R | Cx+Rx | 11 mo, DOD |
| Bender and Mayernik [13] | 1986 | 34 | M | Frontal lobe and dura, right | Yes | B | Cx+Rx | N/A |
| Doorly et al. [14] | 1987 | 51 | M | Cerebellum | No | R | Cx+Rx | 12 mo, NED |
| Ashby et al. [15] | 1988 | 62 | M | Frontoparietal lobe, right | No | R | Cx+Rx | 14 mo, NED |
| Sickler et al. [16] | 1990 | 84 | F | Parietooccipital lobe, right | No | R | Rx | 8 mo, NED |
| Clark et al. [17] | 1992 | 53 | F | Cerebellum | No | R | Rx | 6 mo, NED |
| Deckert-Schlüter [18] | 1998 | 62 | F | Fronto-parietal lobe, left | Yes | R | Cx+Rx | 13 mo, NED |
| Klein et al. [19] | 1999 | 54 | M | Occipital lobe, left | No | R | Cx+Rx | 12 mo, NED |
| Biagi et al. [20] | 2000 | 52 | M | Tempoparietal lobe | No | R | Rx | 29 mo, NED |
| Herrlinger et al. [21] | 2000 | 66 | W | Fronto-parietal lobe, left | No | R | Cx+Rx | 18 m, NED |
| Johnson et al. [22] | 2000 | 55 | F | Cerebellum | No | R | Rx | 8 mo, NED |
| Figueroa et al. [23] | 2004 | 23 | F | Posterior fossa | Yes | R | Cx+Rx | N/A |
| Hirmiz et al. [24] | 2004 | 38 | M | Parietal lobe, right | Yes | R | Cx+Rx | 12 mo, NED |
| de Castro et al. [25] | 2007 | 63 | M | Frontotemporal lobe, left and cerebellum | No | N/A | N/A | N/A |
| Hwang et al. [26] | 2007 | 64 | F | Cerebellum | No | R | Rx | 16 mo, NED |
| Morawa et al. [27] | 2007 | 51 | M | Frontal lobe, right | Yes | R | Cx+Rx | N/A |
| Subklewe and Anagnostopoulos [28] | 2007 | 65 | F | Temporal lobe, right | No | N/A | N/A | 18 mo, NED |
| Apollonsky et al. [29] | 2008 | 22 | F | Frontal lobe, left | Yes | R | Cx+Rx | 48 mo, NED |
| Gerstner et al. [9] | 2008 | 58 | F | Not specified | No | R | Rx | 90 mo, NED |
| 2008 | 60 | F | Not specified | No | R | Rx | 1 mo, NED | |
| 2008 | 46 | M | Not specified | Yes | B | N/A | N/A | |
| 2008 | 72 | M | Not specified | Yes | R | No | 5 mo, NED | |
| 2008 | 37 | F | Not specified | Yes | B | Cx+Rx | 15 mo, DOD | |
| 2008 | 19 | M | Not specified | Yes | B | Cx+Rx | 128 mo, NED | |
| 2008 | 44 | M | Not specified | Yes | No | Cx+Rx | 4 mo, DOD | |
| 2008 | 23 | M | Not specified | Yes | R | Cx+Rx | 53 mo, NED | |
| Almhanna et al. [30] | 2009 | 65 | M | Temporal lobe, left | Yes | R | Cx+Rx | N/A, DOD |
| Foo et al. [31] | 2011 | 58 | M | Temporal lobe, left | No | R | Rx | 14 mo, RD |
| Torgerson et al. [32] | 2011 | 79 | F | Temporal lobe, left | Yes | B | Rx | 1 mo, N/A |
| Gressi et al. [33] | 2013 | 77 | M | Cerebellum | No | R | Rx | 8 mo, NED |
| 2013 | 59 | M | Brain stem | No | R | N/A | 2 mo, N/A | |
| 2013 | 65 | F | Temporal lobe, left | Yes | B | Cx | 22 mo, NED | |
| Kresak et al. [34] | 2013 | 70 | M | Cerebellum | No | R | Rx | 10 yr, NED |
| 2013 | 72 | F | Cerebellum | No | R | Rx | 6 mo, NED | |
| Henkenberens et al. [35] | 2014 | 47 | M | Cerebellum | No | R | Cx+Rx | 9 mo, NED |
| Martinez et al. [36] | 2014 | 74 | F | Brain stem | No | B | Rx | N/A |
| Sharaf et al. [37] | 2014 | 77 | M | Cerebellum | No | R | Rx | 7 mo, NED |
| van Blydenstein et al. [38] | 2014 | 41 | M | Parietal lobe, left | Yes | B | No | 10 d, DOD |
| Shivane et al. [39] | 2016 | 59 | F | Frontal lobe, right | No | R | Cx+Rx | 2 mo, NED |
| Alfaseh et al. [40] | 2019 | 38 | M | Cerebellum | No | R | Cx+Rx | 7 yr, NED |
| Azriel et al. [41] | 2019 | 49 | M | Septum pellucidum | No | R | Cx | N/A |
| Riccioni et al. [42] | 2020 | 30 | M | Frontal - orbital - ethmoidal, left | No | R | Cx+Rx | 30 mo, NED |
| Szczepanek et al. [43] | 2020 | 33 | F | Temporal lobe, left and cerebellum | Yes | R | Cx+Rx | N/A |
| Ahmed et al. [44] | 2021 | 35 | M | Parietal lobe, right | Yes | R | Cx | 4 mo, NED |
| Fu et al. [45] | 2021 | 60 | M | Cerebellum | No | R | Cx | 3 mo, NED |
| Kanagalingam et al. [46] | 2023 | 71 | M | Frontal lobe, right | No | R | Cx+Rx | 5 yr, NED |
| Present report | 2024 | 27 | M | Occipital lobe, right | Yes | R | Rx | 8 mo, NED |
![]()
First, examining the age distribution, while primary CNS lymphoma has a significantly higher incidence between the ages of 60 and 80 compared to other age groups [781011], IC-HL also has a higher incidence in the 60s, but not markedly more than in other age ranges (Fig. 4). This is consistent with the observation that HL displays a bimodal incidence peak in both younger and older populations [148].

Of a total of 47 cases, including ours, 39 had clearly described locations. Among these, 24 cases (61.5%) of the total, had tumors located in the supratentorium. This rate is significantly lower compared to DLBCL, where tumors are located in the supratentorium in approximately 87% of cases. Furthermore, IC-HL was found in the cerebellum in 13 cases (33.3%). Including the 2 cases from the occipital lobe and 2 from the brain stem, 43.5% of cases are associated with posterior circulation regions, such as the brainstem, cerebellum, and occipital lobe. Within the supratentorium, while DLBCL predominantly affects the frontal lobe and periventricular white matter, IC-HL often arises adjacent to the dura mater, presenting in varied locations. This can lead to potential misdiagnoses of IC-HL as other tumors, particularly meningiomas, or as ischemic or inflammatory lesions during the initial radiologic diagnosis. Our case also displayed unique morphological characteristics, from well-defined borders to intense enhancement patterns, extending into the dura and sinus. These features are similar to those seen in meningiomas (Fig. 1A). These characteristics distinguish IC-HL from DLBCL and are beneficial for its diagnosis. There were 19 cases (40.4%) accompanied by systemic HL, while 28 cases (60.6%) were not, indicating that the frequency of isolated IC-HL is relatively high. As previously mentioned, it is hard to diagnose HL using just radiologic findings, so a biopsy is essential to differentiate it from other tumors like meningiomas. Pathologically, the presence of monucleated Reed-Sternburg cells and immunohistochemical staining for CD30 and CD15 are key markers, making the biopsy-based diagnosis of classic HL definitive [1248].
While the primary treatment strategy for DLBCL involves chemotherapy induction after a biopsy, out of 44 cases where surgical details were clearly recorded, 36 (81.8%) of IC-HL underwent surgical resection, and only eight cases (18.1%) had just a biopsy. Among the 44 cases where postoperative treatment details were clearly described, 21 cases (47.7%) underwent concurrent chemotherapy and radiotherapy, 15 cases (34.1%) had radiotherapy alone, and 4 cases (9.1%) had chemotherapy alone. The majority of the cases received radiotherapy. The follow-up period for “no evidence of disease” varied. Only one case reported a death soon after surgery, with the patient passing away 10 days postoperation due to complications from pulmonary edema [38].
In the radiologic findings unique to IC-HL cases, the majority of the literature suggests that maximal safety resection is achievable. This is largely attributed to the clear demarcation between the tumor and normal tissue, and the common presentation of IC-HL on the brain’s surface. These characteristics notably distinguish IC-HL from DLBCL. Furthermore, the minimal bleeding risk simplified the surgical approach. In our case too, these advantageous conditions allowed for an uncomplicated piecemeal resection (Fig. 2). Hence, when IC-HL is suspected, pursuing maximal safety resection combined with chemotherapy and radiotherapy appears to be advantageous. Currently, a universally accepted treatment for IC-HL remains elusive, emphasizing the need for further research to determine the optimal treatment strategy.
In conclusion, through our case report and literature review, we have examined the distinct differences in IC-HL from radiological, surgical, and etiological findings. We suggest that our insights be helpful and hope they contribute to further research and advancements in the treatment of IC-HL.
Go to :
 XML Download
XML Download