

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Lynch syndrome (LS) is an autosomal dominant disorder caused by mutations in mismatch repair (MMR) genes, including MLH1, MSH2, MSH6, and PMS2, which represent loci on 3p22.2, 2p21, 2p16.3, and 7p 22.1, respectively [12]. LS is also associated with an increased risk of colorectal, endometrial, and several other cancer types [34]. Brain tumors occur in 1%–6% of LS cases, with glioblastomas being the most common type [5]. Recent studies have elucidated the pathogenesis and treatment of MMR-deficient gliomas, including LS-associated gliomas. Immune checkpoint inhibitors (ICIs) have shown promising results in some cases of microsatellite instability (MSI)-high (H) malignancies, but their efficiency varies with the case [6]. Herein, we report a case of LS-associated MSI-H glioblastoma showing resistance to immunotherapy, and review the relevant literature.
Go to : 
CASE REPORT
History and examination
A 41-year-old female patient presented with headaches and sensory disturbances in the right upper limb for the past 6 weeks. Her mother had been diagnosed with LS through genetic screening. The patient was treated for rectal cancer at the age of 29 years (Fig. 1A). Initial CT revealed two brain tumors in the precentral gyrus of the left frontal lobe. MRI revealed two ring-enhancing lesions with peritumoral edema at the same site (Fig. 1B, C, E, and F). A malignant brain tumor was suspected, and the patient was referred to our department for surgical treatment. Following admission, she developed right-sided facial palsy and hemiparesis. A second MRI performed at our hospital showed rapid tumor enlargement. The patient underwent subtotal surgical resection of the tumor with awake craniotomy (Fig. 1D and G).
 | Fig. 1Patient brain neuroimaging. A: Pedigree showing affected and unaffected members of the patient’s family. B-G: MRI showing two lesions. The lesions are hyperintense on axial T2-weighted images (B and E) and ring-enhancing on contrast-enhanced T1-weighted images (C and F). Postoperative contrast-enhanced T1-weighted image shows subtotal resection (white arrow) (D and G).
|
Pathological findings
Histopathological analysis showed focal necrosis with pseudo palisades and microvascular proliferation, along with an MIB-1 proliferation index of 70%, leading to a diagnosis of isocitrate dehydrogenase (IDH) wild-type glioblastoma (Fig. 2). Genetic testing by next-generation sequencing showed alternations in PIK3CA R88Q, TP53 R282W, TP53 R158H, NF1 R304, and ATRX T1582NX. MSI was high and the tumor showed an MSH2 variant on germline sequencing analysis.
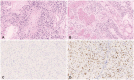 | Fig. 2Histopathological findings showing glioblastoma feature, including poorly differentiated pleomorphic tumor cells with marked nuclear atypia and brisk mitotic activity, focal necrosis with pseudopalisades, and microvascular proliferation. The tumor cells were negative for isocitrate dehydrogenase (IDH)-1. P53 staining showed strong positivity in about 30% of the tumor cells. The lesion was diagnosed as glioblastoma, IDH wild type (A and B: H&E staining, ×100; C: IDH, ×200; D: p53, ×200).
|
Postoperative course
After surgical resection, the patient was treated with daily administration of temozolomide (TMZ; 75 mg/m2) and concurrent radiotherapy (60 Gy). She was subsequently administered TMZ and bevacizumab (10 mg/kg, biweekly). However, 10 months after the initial surgery, the tumors recurred at the same location. A year after the initial surgery, the patient underwent a second surgery, involving subtotal resection. Two weeks after the second surgery, the patient received two cycles of pembrolizumab (200 mg) therapy. However, the second treatment cycle was followed by disease progression and dissemination. Disease progression occurred despite six cycles of pembrolizumab therapy and radiation therapy (40 Gy) for the cerebellar lesion. The patient died due to glioblastoma progression 19 months after the initial treatment.
Go to :
DISCUSSION
Glioblastoma and LS
Although the association between LS and glioma is well-known, the clinical course and outcomes of LS-associated glioblastomas remain unclear. The lifetime risk of brain tumors in LS patients ranges from 1% to 6% by the age of 70 years [7]. Therkildsen et al. [8] demonstrated that 56% of LS-associated brain tumors are glioblastomas. They also reported the average survival duration of 12.1 months (1–41 months) for LS-associated glioblastomas. A literature review of the LS-associated glioblastoma cases treated with immunotherapy revealed that the survival duration is above 60 months if immunotherapy is successful. In contrast, the survival duration is 15.5–19 months in cases resistant to immunotherapy (Table 1).

Table 1
Reported glioblastoma cases with Lynch syndrome that underwent immunotherapy
| Study | Age/Sex | Location | Other associated tumors | Duration between the diagnosis of high-grade glioma and cancer | Surgery | Treatment | MMR mutations | MSI | TMB | Ki-67 | Survival after the diagnosis of high-grade glioma |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Anghileri et al. [24] | 33/F | Left frontal lobe | Adenoma with high-grade dysplasia in the transverse colon | 4 years | GTR | RT/TMZ → nivolumab | MSH2, MSH6 | N/A | High | N/A | Alive at 84 months |
| Sherman and Vitaz [29] | 57/F | Left occipital lobe | Colorectal cancer | 10 years | GTR | RT 60 Gy/TMZ → RT 45 Gy/nivolumab 240 mg | N/A | MSI-H | N/A | N/A | Alive at 5 years |
| Kawaguchi et al. [12] | 79/F | Left parietal lobe | Colorectal cancer | 12 years | GTR | RT 34 Gy/TMZ → pembrolizumab | MSH2 | MSI-H | 101.6/Mb | 47% | Died after 15.5 months |
| Present case | 41/F | Left frontal lobe | Colorectal cancer | 12 years | STR | RT 60 Gy/TMZ → pembrolizumab 200 mg | MSH2 | MSI-H | High | 70% | Died after 19 months |
![]()
Mutated genes in MMR-deficient glioblastomas
LS is caused by heterozygous and homozygous germline mutations in one of the MMR genes [9]. MSH2 (40%–50%) and MLH1 (30%–37%) germline mutations are the most common, while MSH6 and PMS2 mutations are found in only 7%–13% and up to 9% of the cases, respectively [910]. Therkildsen et al. [8] demonstrated a significant increase in the risk of brain tumors with MSH2 gene mutations.
MMR-deficient IDH wild-type glioblastomas, including the present case, are associated with TP53, NF1, EP300, GATA3, NOTCH1, and PIK3CA mutations [1112]. Most LS-associated glioblastomas also have MSI-H [11]. A subset of MSI-H Lynch tumors also present with TP53 mutations, which are otherwise rare in MSI-H cancers [13]. All TP53-mutant tumors present with a non-polypous histology, suggesting that TP53 and CTNNB1 mutations may act as the drivers of nonpolyposis cancer formation in LS [14].
MMR deficiency is often associated with MSI-H and tumor mutational burden (TMB)-H, contributing to poor outcomes [1516]. Some studies have reported that MMR-deficient gliomas could be resistant to TMZ [17]. According to Kim et al. [11], the progression-free survival ranges from 1 month to 42 months for patients with recurrent malignancies. The 2-year survival rate was found to be 29.0% in MMR-deficient glioblastomas. Moreover, Kaplan-Meier survival analysis revealed that patients with MMR-deficient high-grade gliomas had shorter progression-free and overall survival rates compared to those without MMR-deficient high-grade gliomas.
Adjuvant therapy for MMR-deficient glioblastomas
ICIs have shown promising results for some MSI-H malignancies [18]. Increased expression of neoantigens promotes the effect of programmed cell death-1 (PD-1) blockade on MMR-deficient cancers [6]. However, the effect on gliomas is limited due to intratumor heterogeneity related to MMR deficiency [1920]. This heterogeneity is attributed to an acquired MMR gene mutation found in gliomas treated with TMZ [2122]. Previous reports have indicated that MSI-H is not always associated with the effect of anti PD-1 immunotherapy in MMR-deficient glioblastoma [2324]. Meanwhile, TMB is associated with favorable outcomes following anti PD-1 immunotherapy [11242526]. Indraccolo et al. [27] reported that the relationship between MMR/TMB deficiency and MSI may vary with the tumor type.
Friedman et al. [28] demonstrated that EGFR amplification is associated with poor survival rates after ICI treatment in recurrent glioblastoma patients. EGFR can serve as a biomarker for ICI resistance and may be used to distinguish between responders and non-responders.
The efficacy of ICI in the treatment of MMR-deficient glioblastomas has been disappointing, but it remains unknown whether glioblastomas with TMB-H or without EGFR amplification respond to ICI in LS patients [2428]. Further clinical trials of immunotherapy for specific MMR-deficient brain tumors are required.
In conclusion, we presented a case of LS-associated glioblastoma showing ICI resistance despite MSI-H. Our findings indicate that some LS-associated glioblastomas may be resistant to immunotherapy.
Go to :
 XML Download
XML Download