

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Brainstem gliomas, which make up 10%–20% of pediatric central nervous system tumors, are classified into two different types—focal brainstem gliomas and diffuse intrinsic pontine gliomas (DIPGs)—largely based on MRI findings [1]. Focal brainstem gliomas are usually benign tumors of World Health Organization (WHO) grade I–II, whereas DIPGs are almost always highly malignant and fatal [123]. The prototypical features of focal brainstem gliomas on brain MRI are well-defined borders, lack of surrounding edema, iso- or hypointensity on T1-weighted images, hyperintensity on T2-weighted images, and homogeneous contrast enhancement. By contrast, DIPGs are infiltrative diffuse pontine tumors, typically presenting with brainstem expansion on imaging with partial contrast enhancement [4]. Since 2016, the WHO classification of brainstem tumors requires tissue biopsy to reveal molecular characteristics [5]. In this classification, many DIPGs are newly referred to as diffuse midline glioma (DMG), H3 K27M-mutant. Although modern techniques of stereotactic or navigation-guided biopsy ensure accurate and safe biopsy of the lesion, biopsy of brainstem lesions is still not generally performed due to the possibility of critical side effects [67].
Most sporadic brainstem gliomas exhibit neurological symptoms and signs, such as isolated cranial nerve deficits, neck stiffness, pain, and contralateral hemiparesis [3]. However, some of them occur asymptomatically, especially among neurofibromatosis type I patients [8]. Thus, it is challenging for neurosurgeons or oncologists to perform the biopsy of a brainstem lesion, especially when the patient presents with minimal or no symptoms.
We report a case of a 9-year-old girl with no neurological symptoms who presented with a brainstem glioma–mimicking lesion on MRI, which regressed spontaneously during years of follow-up.
CASE REPORT
A 9-year-old girl presented to a local university hospital for a precocious puberty examination due to low height (25th percentile). She did not have any neurological symptoms. Gonadotropin-releasing hormone (GnRH) stimulation test results were consistent with central precocious puberty. Next, brain MRI was performed. It revealed a 12×9×10-mm well-defined, lobulated, contoured, T1 low-intensity and T2 high-intensity intra-axial lesion with equivocal gadolinium enhancement, diffusion restriction, mild choline (Cho) elevation (Cho/creatine [Cr] ratio of 1.68) with N-acetylasparate (NAA) suppression (Cho/NAA ratio of 0.82), and 11C-methionine positron emission tomography (PET) uptake at the pons, suggesting a tumorous lesion or toxic/metabolic lesion (Fig. 1).
The patient visited our outpatient clinic for a second opinion. A routine laboratory examination, including a hormone test, revealed no abnormal findings. On physical examination, she had breast budding but did not show any other secondary sexual characteristics. The attending pediatrician and radiation oncologist brought the case to the neuro-oncology board meeting. As the brainstem lesion had no mass effect unlikely to DIPG, brainstem tumor was not a perfect diagnosis explaining the MR findings. Tumor-mimicking demyelinating lesion is one of the possible diagnoses, but no further workup such as cerebrospinal fluid examination was done since parents were reluctant of further exams because she had neither corresponding clinical history nor symptoms and signs. The board members suggested observation and follow-up MR spectroscopy with perfusion MRI as she had no symptoms or signs related to the brainstem lesion.
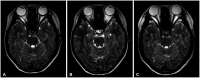
One and a half months after the initial MRI, MR spectroscopy with perfusion MRI and 18fluorodeoxyglucose (FDG) PET were conducted for further evaluation. T2-weighted MRI showed no definite change in the pontine high-signal lesion, and MR spectroscopy revealed no choline elevation (Cho/Cr ratio of 1.13) or NAA reduction (Cho/NAA ratio of 0.56) (Fig. 2A and B, respectively). Perfusion MRI showed no definite relative cerebral blood volume increase (Fig. 2C), and 18FDG PET showed no hypermetabolic lesion (Fig. 2D).
The attending physician did not start any type of treatment as the patient had no symptoms from the lesion, although it had a small possibility of being tumorous, and chemo-/radiation therapy for brainstem lesions could cause serious adverse events for a child. A leuprolide acetate (a GnRH agonist) injection was done 3 months after the initial MRI.
Follow-up MRI 6 months after the initial study showed a decrease in the extent of the lesion on T2-weighted imaging (Fig. 3A); on a follow-up MRI 1.5 years after the initial visit, the lesion was almost invisible (Fig. 3B), and it remained invisible on the most recent follow-up 6.5 years after the initial evaluation (Fig. 3C).
DISCUSSION
Differential diagnosis of brainstem lesions in children is challenging as pediatric brainstem tumors are among the most common lesions [9]. DIPG or DMG, one the most common brainstem tumors, shows typical radiographic features on MRI of infiltrating the majority of the pons, hypo/iso-intensity on T1-weighted imaging, hyperintensity on T2-weighted imaging, and, frequently, ventral involvement of the pons with encasement of the basilar artery. By contrast, focal brainstem lesions pose a particular diagnostic concern by including not only tumors but also inflammatory mimics. Fortunately, focal brainstem tumors are usually low-grade gliomas, such as tectal midbrain and cervicomedullary gliomas.
The tumor-like lesions that occur in the brain are diverse and can result from infection, hemorrhage, stroke, demyelination, phakomatoses (neurocutaneous syndromes), malformations, vasculitis, and metabolic disorders [10]. Among these, demyelinating lesions, including those from acute disseminated encephalomyelitis and multiple sclerosis, are relatively frequent and share some MRI characteristics with tumorous lesions [11]. However, those diseases can be differentiated by a preceding history of infection, multiple bilaterality of the lesions, or the patient’s age at initial presentation. In some cases, demyelinating disease manifests as a solitary lesion similar to a tumor, called a tumefactive demyelinating lesion. These lesions exhibit decreased cerebral blood volume in perfusion MRI and elevation of Cho, lactate, and even glutamate-glutamine peaks in MR spectroscopy [12]. They usually appear as hypometabolic lesions in 18FDG and 11C-methionine PET, but some appear as hypermetabolic lesions [13]. In this case, the lesion had 11C-methionine PET uptake but did not show hyper uptake in 18FDG PET 1.5 months after initial imaging. PET uptake suggests malignancy in many cases, but reports have also shown uptake in tumefactive demyelinating lesions [13]. The mechanism of uptake differs for 18FDG and 11C-methionine as methionine uptake is increased by elevated methionine metabolism and active methionine transport, whereas FDG uptake is increased by high glycolytic metabolism [14].
In this case, MR spectroscopy results were different in the initial imaging and follow-up imaging 1.5 months later in our institution. The initial imaging showed mild Cho elevation (Cho/Cr ratio of 1.68) with NAA suppression (Cho/NAA ratio of 0.82), whereas follow-up imaging showed no Cho elevation (Cho/Cr ratio of 1.13) or NAA reduction (Cho/NAA ratio of 0.56). The difference in MR spectroscopy is hard to explain, but we suggest that not only the time interval but also different MR sequences for analysis according to the hospital or device could contribute to the difference.
Since the 2016 WHO central nervous system tumor classification update, molecular characteristics have been included as a crucial factor in tumor classification, and most DIPGs have fallen into the category of DMG with H3 K27M mutations [5]. In this case, the focal nature of the lesion suggested that it was unlikely to be DIPG or DMG, which is one of the main reasons for the biopsy being deferred.
The optimal treatment for brainstem gliomas is various according to the malignancy grade, the patient’s performance, etc. [1516]. Currently, radiation followed by chemotherapy could be recommended if malignant brainstem glioma is suspected. However, one study showed that in low-grade tumors, upfront observation alone did not result in inferior overall survival or progression-free survival compared with the chemotherapy or radiation therapy group [17].
The limitations of our case are as follows. First, no further workup, such as a cerebrospinal fluid exam or examination of serum markers related to demyelinating diseases, was performed. Second, no biopsy was performed; thus, the final diagnosis remains unknown.
Upon the experience of this case, we cordially suggest that if children is asymptomatic with tumor-like brainstem lesion on MRI, upfront observation should be considered primarily.


 XML Download
XML Download