

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Coronary artery disease (CAD) is one of the major causes of left ventricular (LV) systolic dysfunction, which subsequently leads to heart failure (HF) of ischemic origin (so-called “ischemic cardiomyopathy”). Patients who have experienced acute coronary syndrome or had CAD and were treated with percutaneous coronary intervention (PCI) often exhibit ischemic cardiomyopathy.123 In general, HF is also regarded as a prothrombotic condition with increased platelet reactivity and hypercoagulability due to various mechanisms.456 Antiplatelet agents, in particular P2Y12 inhibitors, have been reported to play an integral role in the secondary prevention of ischemic events after PCI in high-risk patients.78 The antiplatelet effect of P2Y12 inhibitors may be more closely related to clinical events in HF patients with a thrombogenic milieu.9 However, the responsiveness of P2Y12 in an individual patient is not uniform and is believed to be affected by clinical and genetic factors.
Based on platelet reactivity measured by platelet function assays, the concept of therapeutic range with either high platelet reactivity (HPR) or low platelet reactivity (LPR) has been suggested. HPR is associated with an increased incidence of ischemic events, such as myocardial infarction (MI) or death, in patients who previously underwent coronary interventions. On the other hand, LPR is associated with increased bleeding events.10111213141516
Currently, none of the studies have evaluated the association between platelet reactivity and LV systolic dysfunction status, and its prognostic implication in CAD patients treated with drug-eluting stent (DES) implantation. Therefore, we aimed to evaluate the prognostic implication of the association between platelet reactivity and LV systolic function in a large-scale cohort of CAD patients treated with DES implantation.
METHODS
Study design and participants
The PTRG-DES (Platelet function and genoType-Related long-term proGnosis in DES-treated patients with CAD) consortium was established to determine the association of platelet function test (PFT) and genotyping with long-term prognosis during clopidogrel treatment in a large-scale East Asian cohort treated with DES. This consortium was endorsed by the Korean Society of Interventional Cardiology (ClinicalTrials.gov Identifier: NCT04734028).17 A total of nine prospective registries from 32 Korean academic centers joined the PTRG-DES consortium and contributed data of 13,160 DES patients treated between July 2003 and August 2018. We obtained 11,714 PFT results measured by VerifyNow assay (PTRG-PFT cohort), and 8,163 genotyping results related to clopidogrel responsiveness (PTRG-Genotype cohort) from the consortium. Consecutive patients at each center were successfully treated with one or more DES approved by the US Food and Drug Administration or Conformité Européene mark. Patients adequately loaded with aspirin and clopidogrel were eligible for enrollment in the study, regardless of patient or lesion complexity. The exclusion criteria were occurrence of a major complication during the procedure, fibrinolytic therapy, and need for oral anticoagulant.
Procedures
All PCI procedures were performed in accordance with the standard technique.18 Following the procedure, patients were administered 100 mg of aspirin and 75 mg of clopidogrel per day. Patients were recommended aspirin indefinitely and clopidogrel for a duration of at least 1 year. All other treatments administered were according to the standard care. Clinical outcomes were evaluated until the last outpatient visit.17
PFT
Platelet reactivity was measured during the peri-procedural period using the VerifyNow assay (Accriva, San Diego, CA, USA). The measurements were performed after an adequate time duration to ensure full anti-platelet effect.19 Aspirin was administered as either (1) a coated 300-mg oral dose at least 6 hours or (2) a dose of 100 mg at least 5 days before PCI. Clopidogrel was administered in one of the following ways: 1) a dose of 600 mg at least 6 hours; 2) a dose of 300 mg at least 12 hours; or 3) a dose of 75 mg at least 5 days before PCI. If eptifibatide or tirofiban was used during PCI, a 24-hour washout period was required before VerifyNow testing. No patients receiving abciximab were enrolled as a long washout period would be needed.17
VerifyNow assay is a whole-blood, point-of-care, turbidimetric optical detection assay designed to measure agonist-induced platelet aggregation.19 Blood samples were collected in 3.2% citrate Vacuette tubes (Greiner Bio-One Vacuette North America, Monroe, NC, USA). Measurements were performed in accordance with the manufacturer’s protocol, the details of which have been described elsewhere.20 The cartridge comprised fibrinogen-coated polystyrene beads, 20 mmol/L adenosine diphosphate, and 22 nmol/L prostaglandin E1. The optical signal of this channel was reported as “P2Y12 reaction units (PRUs).” We assessed PRUs as continuous and categorical measures. Additionally, the cutoffs of HPR to ADP were defined according to the time-dependent receiver operating characteristic curve analysis from the PTRG-PFT cohort (≥ 252 PRUs).21
Status of LV systolic dysfunction
Echocardiography was performed using commercially available equipment during the peri-procedural period. Standard echocardiography and calculations were performed according to the recommendations of the American Society of Echocardiography.22 Echocardiography was performed by certified echocardiographers, and an echocardiography specialist supervised all the measurements independently. Left ventricular ejection fraction (LVEF) was calculated according to the modified Simpson rule using LV end-systolic and end-diastolic volumes.23
According to the current guidelines and status of LV systolic function, the study population was divided into two groups: preserved-ejection fraction (PEF: LVEF ≥ 50%) group and reduced-EF (REF: LVEF < 50%) group. Additionally, in a separate analysis, we classified LV systolic dysfunction based on LVEF: (1) preserved EF (PEF), LVEF ≥ 50%; (2) mildly reduced EF (mrEF), 40% < LVEF < 50%; and (3) reduced EF (rEF), LVEF ≤ 40%.2425
Clinical outcomes
The primary endpoint was occurrence of major adverse cardiac and cerebrovascular events (MACCEs) including all-cause death, MI, definite stent thrombosis (ST), or stroke. In addition, major bleeding was defined as Bleeding Academic Research Consortium bleeding types 3-5.26
All deaths were considered to have occurred due to cardiovascular (CV) causes unless a definite non-CV cause was established. Acute MI was defined as increased cardiac troponin values with ischemic symptoms or ischemic changes on electrocardiogram or imaging evidence of recent loss of viable myocardium or new regional wall motion abnormality, all of which were not related to the procedure.27 Stroke was defined as evidence of neurological deficit requiring hospitalization and presence of clinically documented lesions on brain computed tomography or magnetic resonance imaging. An independent clinical events committee masked to VerifyNow and LVEF results adjudicated all the clinical events using original source documents.
Statistical analysis
Kolmogorov–Smirnov test was performed to analyze normal distribution of continuous variables. Continuous variables were expressed as mean ± standard deviation or as medians (interquartile range [IQR]), while categorical variables were presented as absolute numbers and frequencies (%). Student’s unpaired t-test was used for parametric continuous variables and Mann–Whitney U test for non-parametric continuous variables. Analysis of variance was used for comparison amongst the three groups. Comparisons between categorical variables were performed using Pearson’s chi-square test or Fisher’s exact test when the Cochran rule was not met.
All demographic characteristics and laboratory measurements were evaluated in a univariate analysis. Variables with P < 0.1 in the univariate analysis were then entered into multivariate logistic backward elimination analysis to obtain odds ratios (ORs) and 95% confidence intervals (CIs). Univariate and multivariate Cox proportional hazard analyses were performed to identify proportional hazard risk on clinical events according to PRU levels and to adjust for known potential confounders (index MI presentation, age, sex, body mass index, hypertension, dyslipidemia, smoking, diabetes mellitus, chronic kidney disease, anemia, congestive HF, previous PCI, previous stroke, multivessel disease, PCI for left main or left anterior descending artery, use of 2nd DES, complex PCI, beta blocker, angiotensin blockade, statin, and proton pump inhibitor). A P value < 0.05 was considered statistically significant. All statistical analyses were performed using R (version 4.2.1, R Foundation for Statistical Computing, Vienna, Austria).
Ethics statement
The Institutional Review Board of each participating center reviewed and approved the registry and waived the requirement for written informed consent for access to an institutional registry (Kangnam Sacred Heart Hospital Institutional Review Board approval no. 2018-10-019). The study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki as reflected in a priori approval by the institution’s human research committee.
RESULTS
Baseline characteristics
In the PTRG-PFT cohort (11,714 patients with VerifyNow result), the on-admission LVEF data was available for a total of 9,319 patients (79.6%) (81.8% [n = 7,620] in the PEF and 18.2% [n = 1,084] in the REF groups) (Fig. 1). According to the LVEF level, no statistically significant differences were observed between the PEF and REF groups in terms of PRU level (216 ± 77.3 vs. 220.5 ± 82.0; P = 0.070), but the prevalence of HPR was significantly different (33.2% vs. 35.4%; P = 0.008) (Table 1).
Fig. 1
Flow chart.
LVEF = left ventricular ejection fraction, PEF = preserved ejection fraction, REF = reduced ejection fraction, HPR = high platelet reactivity, mrEF = mildly reduced ejection fraction.
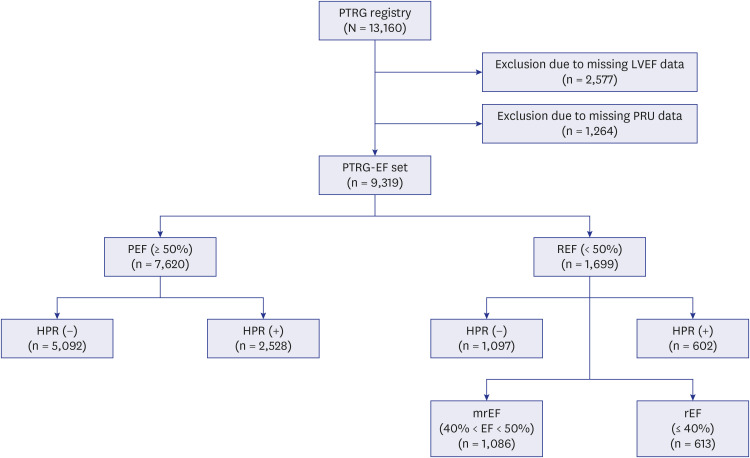
Table 1
Comparison of baseline characteristics between reduced and preserved ejection fraction groups
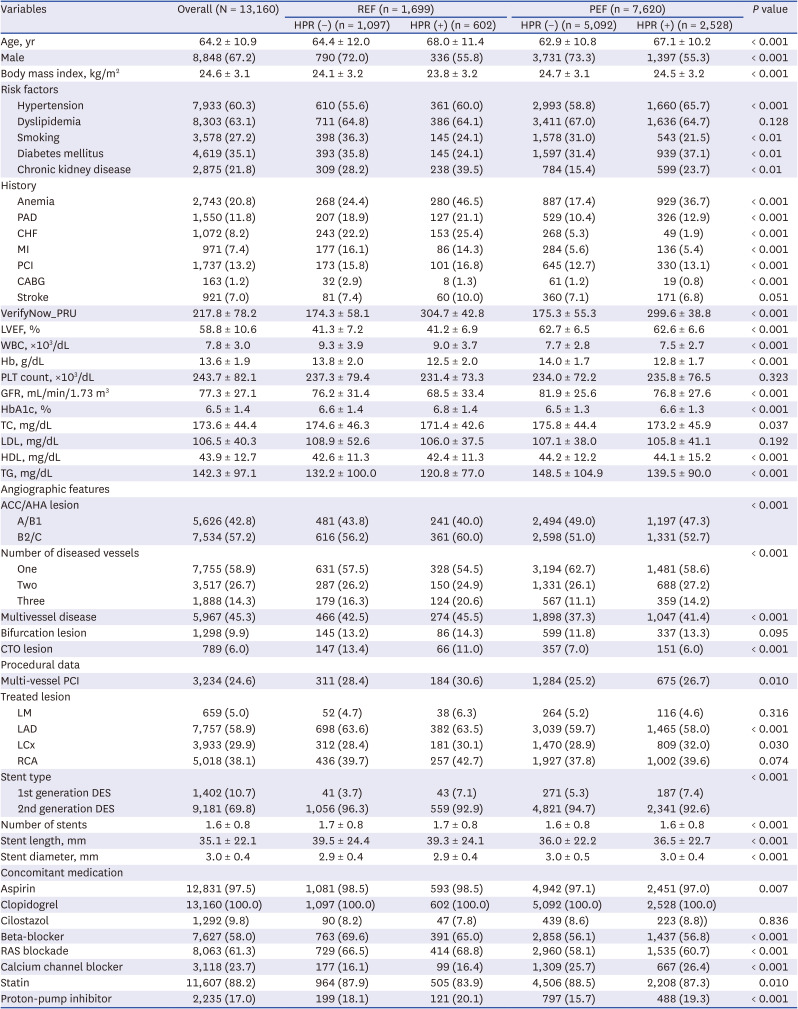
Values are presented as mean ± standard deviation or number (%).
REF = reduced ejection fraction, PEF = preserved ejection fraction, HPR = high platelet reactivity, PAD = peripheral artery disease, CHF = congestive heart failure, MI = myocardial infarction, PCI = percutaneous coronary intervention, CABG = coronary artery bypass graft, LVEF = left ventricular ejection fraction, WBC = white blood count, Hb = hemoglobin, PLT = platelet, GFR = glomerular filtration ratio, TC = total cholesterol, LDL = low-density lipoprotein, HDL = high-density lipoprotein, TG = triglyceride, CTO = chronic total occlusion, LM = left main, LAD = left anterior descending artery, LCx = left circumflex artery, RCA = right coronary artery, RAS = renin-angiotensin-aldosterone system, DES = drug-eluting stent.
In addition, no statistically significant differences in PRU level (216.5 ± 77.3 vs. 219.3 ± 82.5 vs. 222.7 ± 81.2 PRUs; P = 0.111) and HPR prevalence (33.2% vs. 35.0% vs. 36.2%; P = 0.179) were found amongst the three groups according to the LVEF level (Supplementary Table 1). We further investigated the relationship between PRUs and LVEF, which showed no association (Supplementary Fig. 1).
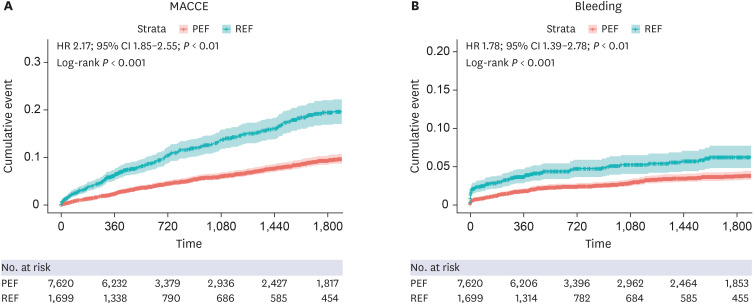
Clinical outcomes according to LV systolic function
During the median follow-up period of 16.8 months (IQR, 12.0–59.8), a total of 455 MACCEs (6.0%) (224 deaths [2.9%], 118 non-fatal MI [1.5%], 37 ST [0.5%], and 132 non-fatal stroke [1.7%]) and 223 cases of major bleeding (2.9%) occurred in the PEF group. In the REF group, 227 cases of MACCEs (13.2%) (164 deaths [9.7%], 47 non-fatal MI [2.8%], 13 ST [0.8%], and 42 non-fatal stroke [2.5%]) and 88 cases of major bleeding (5.2%) was documented (Supplementary Table 2). The REF group had a significantly higher rate of occurrence of MACCEs compared with the PEF group (HR, 2.17; 95% CI, 1.85–2.55; P < 0.001). In addition, major bleeding occurred more frequently in patients with REF than those with PEF (HR, 1.78; 95% CI, 1.39–2.78; P < 0.001) (Fig. 2). In the multivariable analysis, REF was found to be an independent determinant of MACCE and major bleeding occurrence (Supplementary Table 3). Patients with mrEF (HR, 1.58; 95% CI, 1.29–1.95; P < 0.001) and rEF (HR, 3.38; 95% CI, 2.76–4.14; P < 0.001) showed an increased 5-year risk of MACCEs. Moreover, patients with mrEF (HR, 1.42; 95% CI, 1.03–1.95; P = 0.03) and rEF (HR, 2.46; 95% CI, 1.77–3.42; P < 0.001) also showed an increased risk of major bleeding (Supplementary Fig. 2).
Prognostic implication of HPR status according to LV systolic dysfunction
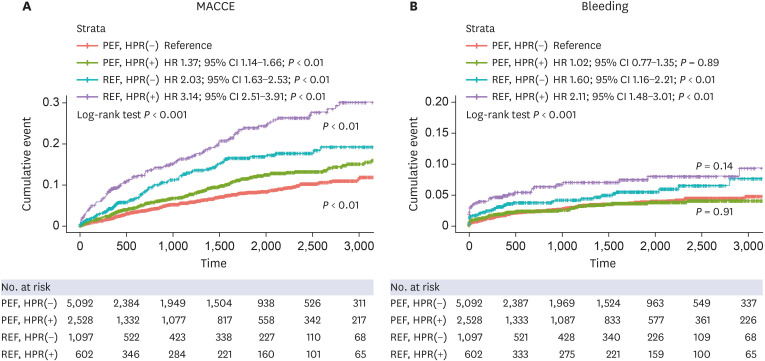
We analyzed the risks of primary outcome and major bleeding according to HPR status and LV systolic dysfunction. Irrespective of LV systolic dysfunction, the HPR phenotype significantly increased the risk of MACCEs (P
interaction < 0.01), and this effect was more prominent in cases of all-cause death and ST (Tables 2 and 3). No association was found between the frequency of major bleeding and HPR phenotype in both PEF and REF groups (Fig. 3).
Table 2
Clinical outcomes in the reduced and preserved ejection fraction groups according to left ventricular ejection fraction and/or high platelet reactivity
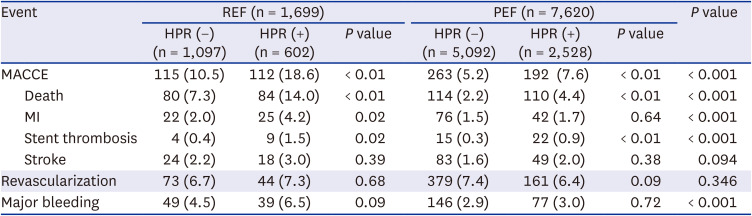
Table 3
Clinical outcomes according to left ventricular ejection fraction and/or high platelet reactivity
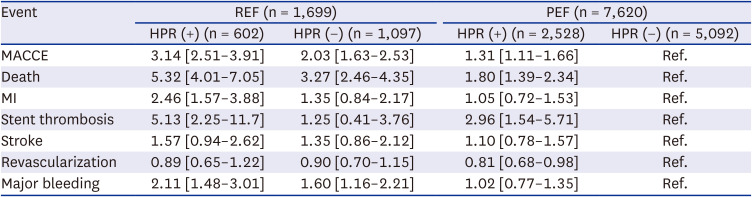
Fig. 3
Kaplan-meier curves related to left ventricular dysfunction and HPR status.
MACCE = major adverse cardiac and cerebrovascular event, REF = reduced ejection fraction, HPR = high platelet reactivity, HR = hazard ratio, CI = confidence interval, PEF = preserved ejection fraction.
We also investigated the association between PRUs and outcomes in each group using spline analysis. The curve showed a linear pattern in the PEF group. Although the spline analysis showed that the outcome decreased with reduction in PRUs in the REF group, the risk tended to rise below 100 PRUs. However, this was not significant (Supplementary Fig. 3).
DISCUSSION
To the best of our knowledge, this study is the first to evaluate the clinical impact of LV dysfunction and platelet reactivity on clinical outcomes (ischemic events and major bleeding) in a large-scale cohort of East Asian patients with CAD who underwent DES-based PCI. The principal findings of this study were as follows:
1) Patients with < 50% LVEF (REF group) showed a two-fold increase in composite ischemic events (MACCEs) compared with the PEF group.
2) The REF group showed a 65% increase in major bleeding events compared with the PEF group.
3) HPR status and PRU levels ≥ 252 had an impact on MACCEs in both the REF and PEF groups; however, no such association was evident in terms of bleeding events.
4) Further breakdown of the REF group into rEF (LVEF ≤ 40%) and mrEF (LVEF 41–50%) showed a difference in MACCE incidence.
Platelets play a key role in thrombotic occlusion during the rupture of a coronary atherosclerotic plaque, leading to myocardial ischemia and infarction.28 Moreover, thrombotic occlusion in epicardial arteries and platelet microembolization can induce tissue damage by microcirculatory arrest.29 Acute myocardial loss due to ischemia can induce myocardial remodeling.30 The mechanisms of remodeling are unclear; however, coronary microcirculation could mediate myocardial ischemic injury.3132 Endothelial cell swelling and sloughing along with platelet aggregates might lead to capillary obstruction. Moreover, advanced capillary impairment could result in intramural bleeding.33 Chronically ischemic myocardium may display structural remodeling of the coronary microvasculature, which appears as atrophy of larger microvessels and reduced vascular distensibility.3435 Moreover, myocardial reperfusion injury could occur paradoxically, resulting in fresh myocardial injury and cardiomyocyte death.36 This process leads to myocardial remodeling that results in reorganization of myocytes, intercellular matrix components, and vessels. Any of these can be reduced, normal, or increased, resulting in myocardial changes that are dependent on the loading conditions, neuroendocrine activation, and genetic factors. Failure to recover from these adverse remodeling events results in progressive dilatation, recruitment of border zone myocardium into the scar, and eventually deterioration in contractile function, known as LV dysfunction.3037
LV dysfunction is a criterion of HF. HF is associated with increased MACCE and thrombotic events, such as venous thromboembolism, due to platelet activation and hypercoagulability.383940414243 In line with these concepts, our data demonstrated that patients with LV dysfunction experienced increased ischemic events compared with those without LV dysfunction, and this difference was statistically significant.
Although the association between bleeding and HF is not well understood, some studies have reported that HF accompanied with atrial fibrillation and chronic kidney disease resulted in increased bleeding.444546 In this study, major bleeding was significantly higher in the REF group compared with the PEF group. The mechanisms of bleeding in HF have not been clearly identified. However, it might be associated with platelet dysfunction and microvascular damage with subsequent derangement of hemostasis, which might increase bleeding.47 Therefore, antiplatelet and anticoagulation therapy in HF patients should be carefully considered in the presence of concomitant vascular disease. Moreover, the balance between thromboembolic and bleeding risk should be carefully monitored.
HPR with the antiplatelet agent clopidogrel is a well-known risk factor for ischemic events in patients undergoing PCI.4849 We used 252 PRUs as the optimal cutoff value, which was higher than the cutoff values used in Europe and the United States.484950 Although the optimal PRU value was higher than that in the Western population, the incidence of ischemic events was lower, which was in concordance with the “East Asian concept.”51 Interestingly, the outcomes were consistent even when the Western cutoff (208 PRUs) was adopted. This demonstrates that the presence of HPR, regardless of whether the Western or East Asian cutoff is being applied, stands out as a significant predictor of future ischemic events (Supplementary Fig. 4). No consistent reports on the association between HPR and bleeding events exist in the literature.4852 The ADAPT-DES (Assessment of Dual AntiPlatelet Therapy With Drug Eluting Stents, N = 8,583) study reported a reduction in relevant bleeding in the HPR group compared with the no-HPR group. However, HPR status did not identify patients at risk for bleeding in a multicenter, prospective registry (j-CHIPS) in Japan, suggesting that ethnic differences might affect the results.4852 In our study, even though HPR status in patients with reduced EF resulted in increased MACCEs, it did not show any difference in terms of bleeding events. This was in accordance with a Japanese study.48 Interestingly, although the presence of HF demonstrated increased MACCE and bleeding risk in the study population, only MACCE, and not bleeding, risk was significantly increased in conjunction with HPR status. This suggests that HPR status may interfere with bleeding tendency in patients with HF, which needs to be validated in a prospective study.
This study has a few limitations. First, the PTRG-DES registry only included patients treated with clopidogrel (excluding potent P2Y12 inhibitors, such as prasugrel and ticagrelor). However, including only those treated with clopidogrel resulted in homogeneity in the study population. Second, owing to the non-randomized, observational cohort design, there may have been inherent selection bias and the possibility of residual confounding factors even after multivariable adjustment. Third, this analysis focused only on platelet reactivity and LV functional status. Further investigations incorporating genetic aspects, like CYP2C19 gene analysis, could be valuable. Finally, LVEF and PRU values were only assessed at the time of index PCI, which might have changed during the study period. Despite these limitations of restricting the generalizability of the results, this study has shown the impact of platelet reactivity on LV function status in a large-scale East Asian PCI cohort.
LV dysfunction was associated with an increased incidence of MACCEs and major bleeding in patients who underwent PCI. The HPR status further exhibited significant increase of MACCEs in patients with LV dysfunction in a large, real-world registry.
 XML Download
XML Download