

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Urinary tract infection (UTI) is common in children and requires antibiotic treatment. Antibacterial resistance in UTIs is a growing problem in both children and adults.123 It is of concern that UTIs caused by resistant pathogens such as extended-spectrum β-lactamase (ESBL) positive gram-negative bacilli (GNB) is rising in children without significant risk factors in the community.456
We previously reported the antibiotic resistance pattern in children less than 24 months of age with UTI and showed an increasing resistance rate of ESBL positivity among isolates of Escherichia coli and Klebsiella pneumoniae from 1.3% to 8.2% over two test periods, 2000–2004 and 2010–2014.7 In young febrile children with toxic appearance and significantly increased inflammatory markers, parenteral antibiotics are used as the empiric treatment. Oral antibiotic treatment is common practice in children with UTIs and there are several options for oral antibiotic treatment.8 However, pediatric UTI caused by ESBL-positive GNB has limited options for oral antibiotics.
Fosfomycin and nitrofurantoin are broad-spectrum cell wall inhibitors that can be useful oral treatment options in non-complicated UTIs of community origin due to their rapid oral absorption, high urine concentration, and bactericidal activity against a wide range of gram-negative and gram-positive bacteria.91011 The purpose of this study was to investigate the susceptibility of ESBL-positive E. coli and K. pneumoniae isolates cultured from pediatric urine samples to two oral antibiotics (fosfomycin and nitrofurantoin).
METHODS
This study included isolates from urine in pediatric patients at Samsung Medical Center from November 2020 to April 2022. Clinical information and microbial data were collected from electronic medical records. Patients over 18 years of age or with malignant diseases were excluded.
Bacterial isolates
ESBL-positive E. coli and K. pneumoniae isolated from urine samples were collected. For repeated isolates from the same patient, only the first isolate was tested. Bacterial species were identified using the VITEK 2 system (bioMérieux, Marcy-l'Etoile, France).
Determination of fosfomycin and nitrofurantoin minimal inhibitory concentration (MIC)
Antibiotic media were prepared with concentrations ranging from 0 mg/L to 256 mg/L through 0.5 serial dilution. Mueller Hinton Agar (BD, Franklin Lakes, NJ, USA) was used for fosfomycin testing and Mueller Hinton Broth (BD) was used for nitrofurantoin.1213 The final inoculation concentration was 104 cfu/spot for fosfomycin testing and 105 cfu/mL for nitrofurantoin. The cultures were incubated at 37°C for 16 hours. E. coli (ATCC 25922), Enterococcus faecalis (ATCC 29212), and Pseudomonas aeruginosa (ATCC 27853) were also tested as controls.
MIC analysis followed the Clinical & Laboratory Standards Institute (CLSI) guidelines,14 and the concentration at which growth was completely inhibited was measured as the MIC of the corresponding strain. According to CLSI guidelines, the E. coli and K. pneumoniae breakpoints for susceptibility was set to ≤ 64 μg/mL and ≤ 32 μg/mL for fosfomycin and nitrofurantoin, respectively.
RESULTS
ESBL-positive isolates
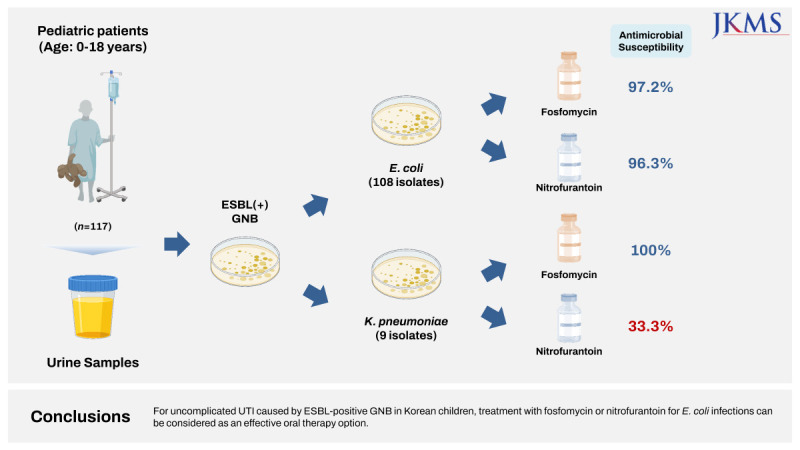
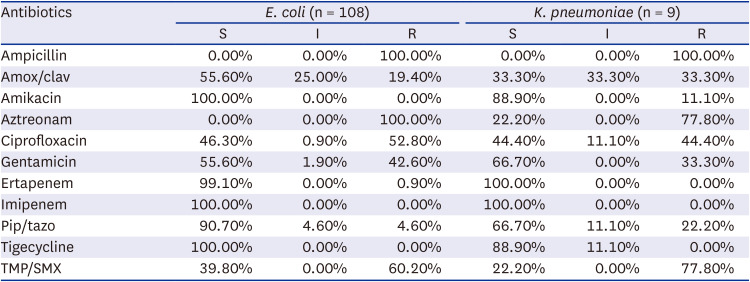
A total of 117 ESBL-positive isolates were collected, of which 108 (92.3%) were E. coli and nine (7.7%) were K. pneumoniae. The median age of patients at the time of positive urine culture was seven months (range, 0.0–18.5 years) (Supplementary Table 1). Among these, 13 isolates (11.1%) were from patients in the PICU; E. coli (n = 11) and K. pneumoniae (n = 2). A total of 104 (88.9%) isolates were from patients in the GW; E. coli (n = 97) and K. pneumoniae (n = 7). Isolates showed high resistance to ampicillin, aztreonam, ciprofloxacin, gentamicin, and trimethoprim/sulfamethoxazole (TMP/SMX) (Table 1).
Table 1
Antibiotic susceptibility of isolates
ESBL-positive E. coli antibiotic susceptibility
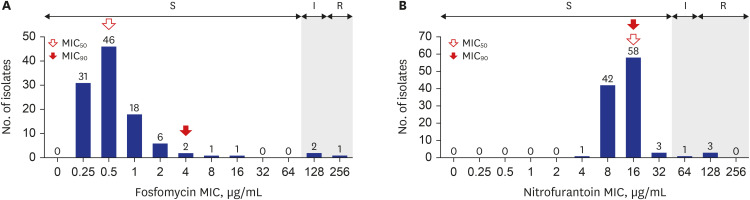
The susceptibility of ESBL-positive E. coli to fosfomycin and nitrofurantoin is shown in Fig. 1. The MIC50 and MIC90 for fosfomycin against the 108 E. coli isolates were 0.5 μg/mL and 2 μg/mL, respectively (Fig. 1A). The fosfomycin susceptibility rate was 97.2% (105/108). Fosfomycin susceptibility was significantly lower in isolates from the PICU than those from the GW (81.8% vs. 99.0%, P = 0.027; Table 2). The MIC50 and MIC90 of nitrofurantoin against the 108 E. coli isolates was 16 µg/mL for both MICs (Fig. 1B). The nitrofurantoin susceptibility rate was 96.3% (104/108). Although not significant, nitrofurantoin susceptibility in isolates from the PICU tended to be lower than those from the GW (81.8% vs. 97.9%, P = 0.051; Table 2).
Fig. 1
Distribution of MICs and susceptibility of ESBL-positive E. coli isolates. (A) ESBL-positive E. coli fosfomycin MIC. (B) ESBL-positive E. coli nitrofurantoin MIC.
MIC = minimum inhibitory concentration, ESBL = extended-spectrum β-lactamase, S = sensitive, I = intermediate, R = resistant.

ESBL-positive K. pneumoniae antibiotic susceptibility
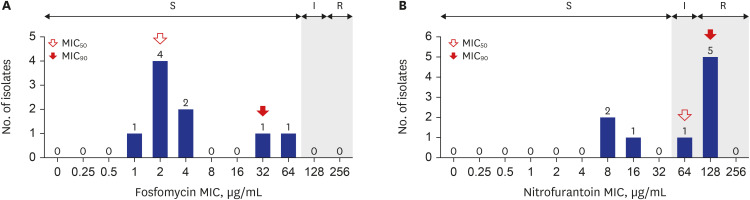
The MIC50 and MIC90 of fosfomycin for the nine K. pneumoniae isolates were 2 μg/mL and 32 μg/mL, respectively (Fig. 2A). All K. pneumoniae isolates were susceptible to fosfomycin; however, only 33% of K. pneumoniae isolates were susceptible to nitrofurantoin. The MIC50 and MIC90 for nitrofurantoin in the nine K. pneumoniae isolates were 64 μg/mL and 128 μg/mL, respectively (Fig. 2B).
Fig. 2
Distribution of MICs and susceptibility of ESBL-positive K. pneumoniae isolates. (A) ESBL-positive K. pneumoniae fosfomycin MIC. (B) ESBL-positive K. pneumoniae nitrofurantoin MIC.
MIC = minimum inhibitory concentration, ESBL = extended-spectrum β-lactamase, S = sensitive, I = intermediate, R = resistant.
DISCUSSION
In this study, we investigated fosfomycin and nitrofurantoin susceptibility in ESBL-positive E. coli and K. pneumoniae isolated from urine in pediatric patients (≤ 18 years). Susceptibility to both fosfomycin and nitrofurantoin in E. coli and susceptibility to fosfomycin in K. pneumoniae were high, above 95%, while only one-third of K. pneumoniae isolates were susceptible to nitrofurantoin. Infection caused by ESBL-positive GNB in children has increased with the increasing use of broad-spectrum antibiotics in recent years.15 In particular, in cases of pediatric UTIs caused by ESBL-positive E. coli and K. pneumoniae, broad-spectrum parenteral antibiotic administration is inevitable in many cases, which not only increases hospital length of stay and medical expenses but may result in the emergence of new resistant bacteria. Recently, it has been reported that fosfomycin and nitrofurantoin, which are old antimicrobial agents, are highly effective against GNB isolated from in urine,101116 and interest in these two drugs as a treatment option for uncomplicated UTI has increased.
Several previous studies have reported on ESBL-producing GNB susceptibility to fosfomycin and nitrofurantoin. In a Canadian study, ESBL-producing E. coli isolated from UTI patients (both children and adults included) reported 100% and 83.3% susceptibility to fosfomycin and nitrofurantoin, respectively, from 2010 to 2013.17 In the U.S., susceptibility of the E. coli ESBL-phenotype to fosfomycin and nitrofurantoin in 2012 was reported to be 98.7% and 82.9%, respectively; however, the susceptibility of 65 Klebsiella ssp. with the ESBL-phenotype (including K. pneumoniae 59 isolates) for nitrofurantoin was very low at 4.6%.18 The results from a 2015 to 2017 study by the East Sussex Healthcare NHS Trust in England showed that ESBL-producing E. coli showed high susceptibility to fosfomycin (98%) and nitrofurantoin (93%), whereas Klebsiella species showed rather low susceptibility at 62% and 58%, respectively.19 In a study conducted on E. coli isolated from adult UTI patients in China, the incidence of ESBL-producing strains ranged from 18% to 43%. The susceptibility to fosfomycin and nitrofurantoin in 332 ESBL-producing isolates (including ESBL-uncertain isolates) was 90.1% and 93.1%, respectively, in 2021.20 In a study of pediatric UTI patients in India, among 271 isolated ESBL-positive strains, E. coli showed the highest proportion with 221 cases (81.6%). The susceptibility to fosfomycin and nitrofurantoin was 98.5% and 95.2% for E. coli and 96.8% and 75.1% for K. pneumoniae, respectively, in 2022 (including both ESBL-positive and ESBL-negative isolates).21 The susceptibility of 267 cases of ESBL-producing E. coli to fosfomycin isolated from urine in Korea was 99.6%, followed by ciprofloxacin (68.5%), trimethoprim–sulfamethoxazole (55.4%), and ampicillin (31.5%).22 However, it is not clear whether pediatric isolates were included in this study.
In our data, ESBL-positive E. coli showed good in vitro susceptibility for both oral fosfomycin and nitrofurantoin, and thus can be reserved for therapeutic candidates. On the other hand, we observed that ESBL-positive K. pneumoniae had a rather low susceptibility to nitrofurantoin, suggesting the importance of antimicrobial susceptibility testing before antibiotic choice. According to Infectious Disease Society of America guidance for the treatment of ESBL-positive Enterobacterales, single-dose oral fosfomycin is selectively recommended as an alternative option for uncomplicated ESBL-positive E. coli cystitis only, since other GNBs including K. pneumoniae retain an intrinsic fosA gene, the product of which can hydrolyze the drug.2324 Nitrofurantoin on the other hand is suggested as the preferred choice for uncomplicated cystitis caused by general ESBL-positive Enterobacterales based on its safety and efficacy, even compared to oral fosfomycin.2325 The guideline suggests that both drugs be avoided for pyelonephritis and complicated UTI because of their low penetration into the renal parenchyma. Intriguingly, recent adult studies have focused on extending multi-dose oral fosfomycin as the treatment option for pyelonephritis or complicated ESBL-positive E. coli UTI.2627 Wald-Dickler et al.26 conducted a multicenter retrospective cohort study that compared clinical efficacy of the outpatient regimen of oral fosfomycin with that of standard ertapenem. The authors found no statistical difference between the two groups regarding clinical success rate at 30-day and relapse rate, suggesting oral fosfomycin as a reasonable step-down option for complicated UTIs.
Unfortunately, only a few pediatric studies regarding oral fosfomycin or nitrofurantoin for UTI treatment have compared data to the adult population.2829 Purcell et al.28 reviewed the medical literature from 1946 to 2020 on oral fosfomycin treatment for pediatric UTI and only found eight related studies, most of which were published more than 20 years ago without reporting multidrug-resistant organisms. With recently increasing ESBL UTI cases among the pediatric population, further organized clinical studies for optimal dosing are in need, as supported by our in vitro clinical data.30
According to the most recent Australian multicenter cohort study published in 2023, fosfomycin was effective for pediatric UTI (aged < 1 year: 1g/single dose or two doses, 1–12 years: 2g/single dose, > 12 years: 3 g/single dose).31 However, this study also mentions that further studies are needed to confirm the appropriate administration therapy and optimal duration of fosfomycin in pediatric population. There is not much literature on the side effects of fosfomycin. According to a clinical record analysis of the side effects of 35,481 fosfomycin conducted in Japan, the overall incidence of side effects was 3.5%. Side effects were higher when the daily dose exceeded 3 g, gastrointestinal disorders (2.7%) were the most common side effects, and there was one case of thrombocytopenia and one case of anemia.32 In a Turkish study of 50 pediatric patients (age 1–17), nitrofurantoin was found to be effective to treat the lower UTI due to ESBL-positive E. coli and no specific adverse effects were observed during the 10-day course of nitrofurantoin treatment (5 to 7 mg/kg/day, 4 divided doses).29 However, there is a report that pulmonary fibrosis was observed during long-term treatment (several years).33 Therefore, additional studies are also needed to confirm the appropriate medication therapy and duration of nitrofurantoin.
In this study, the rate of fosfomycin resistance of E. coli in the PICU was significantly higher compared to the GW. Fosfomycin acts by inhibiting the initial enzymatic step of peptidoglycan biosynthesis in the cytoplasm. Antibiotic resistance mechanisms of fosfomycin are impaired drug uptake, enzymatic drug inactivation, and target modification. Worldwide spread of fosfomycin-modifying enzymes causing drug inactivation has drawn the attention as the emerging mechanism of resistance. This enzymatic drug inactivation is usually plasmid-mediated and fosA3 is most frequently found. There are several studies that reported fosA3 gene variants expressed with resistance to other antibiotic classes.343536 In fact, a previous Korean study by Lee et al.37 reported that among the 21 fosfomycin non-susceptible isolates (E. coli and K. pneumoniae), 7 isolates harbored plasmid mediated fosA3 gene, which was connected to blaCTX-M via insertion sequence, IS26-composite transposon. Therefore, we consider that the higher rate of fosfomycin resistance in PICU may have been influenced by greater exposure to other antibiotics in critically-ill patients in PICU and status of multidrug resistance in some isolates from PICU. However, only 11 E. coli isolates from PICU were included in this study. Therefore, we are cautious to mention any plausible conclusion at this point.
This study has some limitations. First, the study was performed at a single institution, the number of isolates was relatively small at 117, and K. pneumoniae representation was very low at only nine isolates. Second, since this study focused on antimicrobial susceptibility tests of E. coli and K. pneumoniae only, we did not examine the treatment outcome or application of these two drugs in children with uncomplicated UTI. Third, other GNB were not tested.
In conclusion, we examined fosfomycin and nitrofurantoin susceptibility in E. coli and K. pneumoniae isolated from urine in Korean children. Our study implies that fosfomycin and nitrofurantoin are oral treatment options that can be used in pediatric patients with UTI caused by ESBL-positive E. coli.
 XML Download
XML Download