

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Coronavirus disease 2019 (COVID-19), caused by severe acute respiratory syndrome coronavirus 2, spread rapidly as a pandemic and led to significant illness severity and deaths. Data from the early phases of the pandemic showed significant increase in perioperative mortality among patients with preoperative COVID-19. In February 2021, international, multicenter, prospective cohort groups reported that mortality increased among patients with preoperative COVID-19 within 7 weeks of diagnosis, and patients with ongoing symptoms had higher mortality than those asymptomatic or whose symptoms had resolved.1
A retrospective study on pediatric patients reported that the incidence of perioperative respiratory adverse events (PRAEs) was higher in children with positive COVID-19 tests than in matched controls in 2020.2 A recent study reported the complications associated with pediatric airway management in 2020; the incidence of hypoxemia was higher in children who tested positive for COVID-19 and who were symptomatic than in those who tested negative or were asymptomatic.3
In late 2021, new COVID-19 variants such as SARS-CoV-2 B.1.1.529 (omicron) emerged. The omicron variant has increased transmissibility and less severe clinical outcomes.4567 Since the first COVID-19 omicron case in Korea on November 24, 2021, more than 17,000,000 patients (33.4% of the nationwide population) had been diagnosed with COVID-19 as of February 2022.8 The omicron infection incidence reached over 90% in early February and more than 98.9% of COVID-19 cases as of mid-February 2022. On May 31, 2022, approximately 60% of children aged 1–9 years and approximately 50% of children aged 10–19 years had been infected with omicron in Korea (Fig. 1).910
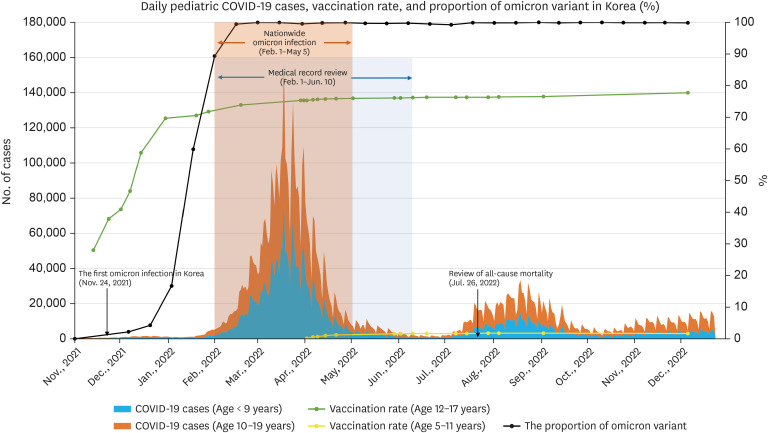
Fig. 1
Daily pediatric COVID-19 cases, vaccination rate, and proportion of the omicron variant in Korea. Nationwide mass infection occurred from February 1 to May 5, 2022. In this retrospective study, the electronic medical records of pediatric patients who underwent general anesthesia at Seoul National University Hospital from January 1 to June 10, 2023, were reviewed. All-cause mortality data were reviewed on July 26, 2022. When the omicron variant became dominant, accounting for more than half of the total, on January 27, 64.6% and 58.2% of children aged 12–17 years had received the first and second vaccination, respectively. There were no reported cases of vaccination in children aged under 11 years in the same period as the vaccination was limited to children aged ≥ 13 years in the Republic of Korea. In our study period, starting from February 1 to May 5, almost all cases of COVID-19 were confirmed to be due to the omicron variant. Vaccination rates of children aged 12–17 years were reported to be 68.5%, 65.6%, and 9.8% for first, second, and third doses, respectively, on May 31. In children aged 5–11 years, only 1.4% and 0.2% received the first and second vaccination, respectively, and there was no vaccination for children aged under 5 years at the same date. Data on the daily pediatric COVID-10 cases and the vaccination rates in Korea were downloaded from https://ncov.kdca.go.kr/ on December 22, 2022.9 Data on the proportion of omicron variant cases in Korea were downloaded from https://ourworldindata.org/coronavirus on December 22, 2022.10
COVID-19 = coronavirus disease 2019.
During the nationwide mass infection period, the Korean Society of Anesthesiologists updated the guideline for the timing of surgery; elective surgery should be delayed for 10 days after COVID-19, and elective surgery within 7 weeks from COVID-19 diagnosis needs individual risk evaluation, decision-making, and informed consent (March 2022). Mandatory COVID-19 testing before each admission was applied to prevent widespread COVID-19 in hospitals. During the omicron-dominant era, most children with preoperative COVID-19 were asymptomatic or showed mild upper respiratory tract infection (URTI) symptoms on the anesthesia day. To avoid massive backlogs in elective surgeries and procedures, the Department of Pediatric Anesthesia in our institution applied the same policy for URTI to COVID-19 omicron cases: postpone elective general anesthesia by 2 weeks if the patient has a significant fever or URTI symptoms.11 For urgent or emergency surgery, surgery for rapidly progressive tumors, and diagnosis, treatment, and care for active disease, general anesthesia was administered to prevent worsening disease progression due to delayed surgery, even if symptoms were present or within 2 weeks of COVID-19 diagnosis. Moreover, additional infection control measures, such as N95 masks, eye protection with goggles or eye shields, or gowns, were not implemented.
In recent retrospective cohort studies comparing the clinical outcomes of the omicron and delta variants in pediatric patients, omicron showed a lower risk of severe illness, including hospitalization, intensive care unit (ICU) admission, and mechanical ventilation.45 However, there was little evidence demonstrating the perianesthetic morbidity and mortality risk after preoperative COVID-19 in pediatric patients,23121314 and there was no evidence regarding anesthesia-associated risk after omicron infection.
We aimed to determine whether pediatric patients with preoperative COVID-19 omicron variant have a higher risk of overall perioperative adverse events, including PRAEs, escalation of care, and mortality.
METHODS
Case selection process
This was a single-center, retrospective study that included pediatric patients (age < 18 years) who underwent general anesthesia between February 1 and June 10, 2022, at a large, tertiary pediatric hospital. Patients were categorized into two groups: those with a preoperative COVID-19 history and those without a history during the omicron-predominant era in Korea. Patients classified as having the COVID-19 omicron variant preoperatively had (a) positive findings on real-time reverse transcription polymerase chain reaction (RT-PCR) testing of nasopharyngeal swabs, (b) positive rapid antigen test performed by a physician, or (c) were automatically notified by synchronization of nationwide infection data from the Korea Disease Control and Prevention Agency (KDCA). Patients classified as not having preoperative COVID-19 were those who had negative RT-PCR nasopharyngeal swab findings within 3 days from admission. Time from the diagnosis of COVID-19 to the day of anesthesia was categorized based on a previous study and reported guidelines11516: 0–2 weeks; 3–4 weeks; 5–6 weeks; and ≥ 7 weeks. The exclusion criteria included patients who underwent cardiac surgery, airway reconstruction surgery, or suspension laryngoscopy; who had structural airway disease; who required preoperative mechanical ventilation; or who had uncertain COVID-19 history.
Data collection
The following information was collected for each patient from the electronic medical record and the “call for help” critical incident announcement and reporting system form of the Department of Pediatric Anesthesia15: age; sex; height; weight; American Society of Anesthesiologists (ASA) physical status; previous airway surgery; documented difficult airway; preoperative oxygen; preoperative ventilator support; preoperative intensive care; type of surgery or procedure; grade of surgery (major/minor); urgency (elective/emergency); COVID-19 diagnosis date; vaccination history; symptoms of COVID-19 at anesthesia day; preoperative chest radiography reading; incidence of PRAEs and desaturation (SpO2 < 95%, > 1 minute) during anesthetic induction, maintenance, emergence, and the post-anesthesia care unit (PACU) stay; significant atelectasis and high peak inspiratory pressure (PIP) (≥ 25 cmH2O) after anesthesia induction; laryngospasm; bronchospasm; oxygen supply after PACU discharge; unexpected use of postoperative mechanical ventilation or high flow nasal cannula; unexpected admission; postoperative pneumonia; and acute respiratory distress syndrome (ARDS).
Data on intraoperative high-resolution time-synchronized vital signs and respiratory waveforms were collected and transferred to a personal computer using the Vital Recorder program (VitalDB, Seoul, Korea; https://vitaldb.net/).18 The pre-anesthesia, anesthesia, PACU, and VitalDB records were carefully and extensively reviewed by three members (J.B.P., J.Y.S., and Y.E.J.) of the research team for consistency.
The all-cause mortality data of those who underwent general anesthesia between February 1 and June 10, 2022, at our hospital were obtained from the Ministry of Security and Public Administration of Korea on July 26, 2022 (Fig. 1).910
In the preliminary retrospective review, the incidence of PRAEs was 7.5% in our institution (unpublished data). Taking this value as a reference, we assumed the incidence of PRAEs of 15% in a group of patients with preoperative COVID-19. Assuming a power of 0.8 for the 7.5% difference, with a two-sided α of 0.05, the sample size for each group was calculated as 277. However, as many children with preoperative COVID-19 history as possible during the study period were included in the analysis.
Outcome definitions
The primary outcomes were the overall perioperative adverse events, including PRAEs, escalation of care, and mortality.1231315 PRAEs included laryngospasm (use of a neuromuscular blocker or propofol or documented in the electronic medical record), bronchospasm (use of a bronchodilator or documentation in the electronic medical record), crackle or wheezing, copious secretion, high PIP (≥ 25 cmH2O), desaturation (SpO2 < 95% for >1 minute), significant airway obstruction requiring intervention, postoperative need for oxygen supplement for > 2 hours; and postoperative pneumonia.111920 Escalation of care included unplanned requirement for postoperative invasive or non-invasive mechanical ventilation, unexpected prolonged supplemental oxygen requirement with a high-flow nasal cannula in phase 2 PACU, unexpected admission, and ARDS. Data regarding postoperative all-cause mortality within 6 weeks were collected.
Secondary outcomes included the cause of desaturation, location of postoperative care (PACU/ICU), and location after PACU care (ward/day-surgery center/ICU).
Matching process
Pediatric patients with the preoperative COVID-19 omicron variant were matched in a 1:1 ratio to children who tested negative for COVID-19 based on age, weight, sex, and department via the following protocol. Encounters were narrowed to those with the exact or nearest matching age, weight, sex, and operation department using the R software (version 4.2.2; R Foundation for Statistical Computing, Vienna, Austria); the package “MatchIt” was used.
Statistical analysis
Data distribution was tested using the Shapiro–Wilk normality test. All data are expressed as mean ± standard deviation or median (interquartile range), unless otherwise specified. The baseline characteristics of the retrospective cohort were evaluated using the independent t-test and Mann–Whitney U test. The primary outcomes, incidence of overall perioperative adverse events including PRAEs, escalation of care, and mortality, were evaluated using the χ2
test. As desaturation is not independent of other PRAEs, we calculated the overall incidence of PRAEs and the frequency of the individual PRAEs. The secondary outcomes were evaluated using the χ2
test, independent samples t-test, and Mann–Whitney U test. Statistical analysis were performed using IBM® SPSS® Statistics 22 (SPSS Inc., IBM Corporation, Armonk, NY, USA) and R software (version 3.4.4; R Foundation for Statistical Computing); the package “moonBook” was used for statistical analysis. Statistical significance was defined as a two-sided P value of < 0.05.
Ethics statement
This study was conducted in accordance with the applicable Strengthening the Reporting of OBservational studies in Epidemiology (STROBE) guidelines and was approved by the Seoul National University Hospital Institutional Review Board, Seoul, Republic of Korea (number H-2206-083-1332; Chairman, Hyun-hoon Jung; Date of approval, June 21, 2022). The requirement for written informed consent was waived because of the retrospective study design.
RESULTS
Propensity score matching
There were a total of 2,690 pediatric general anesthesia cases during the study period: 590 (21.93%) patients had preoperative COVID-19 and 2,100 had a negative test result within 3 days. After excluding 94 patients, 496 patients were included for propensity score matching. Propensity score matching resulted in a good balance in the four confounders (age, weight, sex, and operation department), with standardized differences of < 0.1 for all variables in a 1:1 ratio (Table 1).21 A total of 992 pediatric patients were finally included in the data analysis (n = 496 in the COVID-19 group and n = 496 in the non-COVID-19 group). There was no significant between-group difference in baseline characteristics except for the incidence of emergency surgery (1.2% vs. 4.6%; P = 0.003; odds ratio [OR], 0.252; 95% confidence interval [CI], 0.245–0.259). The durations of anesthesia (mean difference, 18.3 minutes; 95% CI, 5.65–30.86) and surgery (mean difference 11.4 minutes; 95% CI, 0.76–22.02) were longer in the COVID-19 group. There were no differences in the anesthesia induction technique and maintenance. All patients underwent intravenous induction. The use of a neuromuscular blocking agent (OR, 1.51; 95% CI, 1.48–1.54) and type of airway management device were not significantly different between the groups (OR, 1.01; 95% CI, 1.00–1.02).
Table 1
Patient and surgical characteristics and anesthetic management of COVID-19 patients and non-COVID-19 patients after PSM
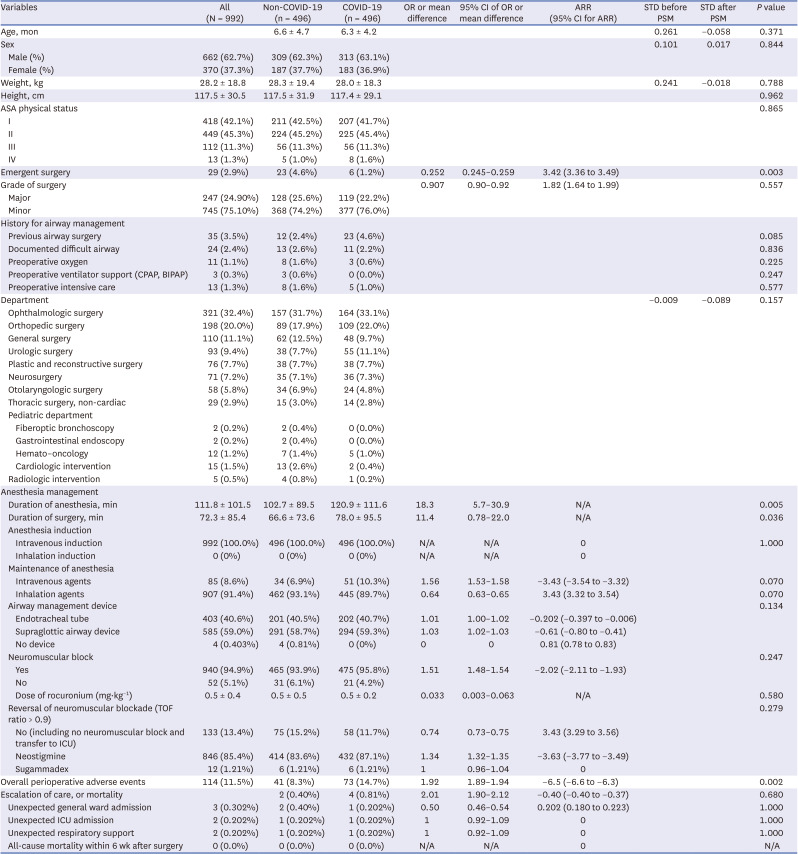
Values are mean ± standard deviation, or median (interquartile range) [range] or number (proportion).
COVID-19 = coronavirus disease 2019, OR =odds ratio, CI = confidence interval, ARR = absolute risk reduction, STD = standardized difference, PSM = propensity score matching, ASA = American Society of Anesthesiologists, CPAP = continuous positive airway pressure, BIPAP = bilevel positive airway pressure, N/A = not applicable, TOF = train–of–four, ICU = intensive care unit.
Primary outcome and secondary outcomes
The overall incidence of perioperative adverse events was significantly higher in the COVID-19 group than in the non-COVID-19 group (8.3% vs. 14.7%; P = 0.002; OR, 1.92; 95% CI, 1.89–1.94; absolute risk reduction [ARR], −6.5%; 95% CI, −6.6 to −6.3) (Table 2). The incidence of escalation of care and mortality was comparable between the two groups (ARR, −0.40%; 95% CI, −0.40 to −0.37). Neither group had any patients who died within 6 weeks of surgery. However, the incidence of PRAEs was significantly higher in the COVID-19 group than in the non-COVID-19 group (7.9% vs. 14.5%; P = 0.001; OR, 2.00; 95% CI, 1.96–2.02). The difference between the two groups was most notable for high PIP ≥ 25 cmH2O during the intraoperative period (OR, 11.0; 95% CI, 10.5–11.4). The overall incidence of perioperative desaturation was not different between the two groups (ARR, 0.4%; 95% CI, 0.3–0.5). However, length of stay in the PACU was longer in the COVID-19 group (mean difference, 18.12 minutes; 95% CI, 15.43–20.81).
Table 2
Overall perioperative adverse events including perioperative respiratory adverse events, escalation of care, and mortality of COVID-19 patients and non-COVID-19 patients after propensity score matching
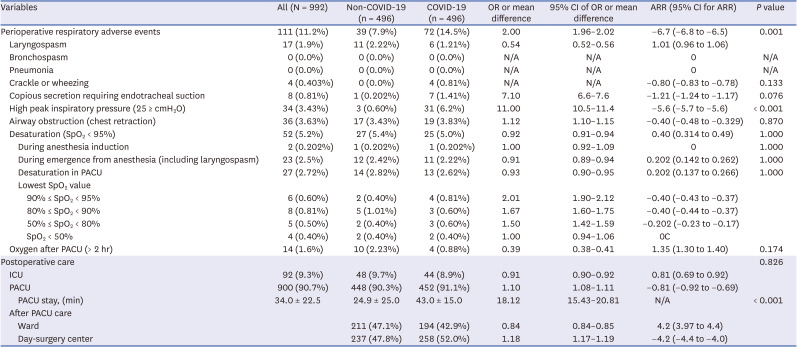
Values are mean ± standard deviation, or median (interquartile range) [range] or number (proportion).
COVID-19 = coronavirus disease 2019, OR = odds ratio, CI = confidence interval, ARR = absolute risk reduction, N/A = not applicable, SpO2 = oxygen saturation, PACU = post-anesthesia care unit, ICU = intensive care unit.
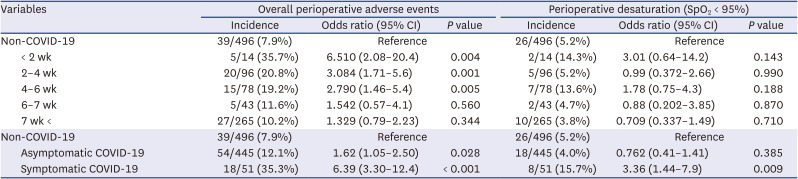
Compared with the non-COVID-19 group, there was a significantly higher risk of overall perioperative adverse events in the COVID-19 group diagnosed 0–2 weeks, 2–4 weeks, and 4–6 weeks before anesthesia (OR [95% CI] 6.5 [2.1–20.4], 3.08 [1.71–5.6], and 2.79 [1.46–5.4], respectively) (Table 3). However, we did not find any significant differences in desaturation. Symptomatic patients in the COVID-19 group had a higher risk of overall perioperative adverse events (OR, 6.4; 95% CI, 3.30–12.4) and desaturation (OR, 3.36; 95% CI, 1.44–7.9) than the non-COVID-19 group. Asymptomatic patients in the COVID-19 group had a higher risk of overall perioperative adverse events (OR, 1.62; 95% CI, 1.05–2.50), but not desaturation, than the non-COVID-19 group.
Table 3
The risk of overall perioperative adverse events and desaturation by the timing of preoperative COVID-19 omicron infection and symptoms on the anesthesia day
The univariate and multivariate analysis results for risk factors associated with overall perioperative adverse events are shown in Table 4. Preoperative COVID-19 showed a strong association (OR, 4.5; 95% CI, 1.96–10.4). In addition, a higher ASA physical status (OR, 1.43; 95% CI, 1.06–1.93), history of difficult airway (OR, 5.45; 95% CI, 2.19–13.6), preoperative intensive care (OR, 3.27; 95% CI, 0.96–11.1), and sputum (OR, 6.5; 95% CI, 1.89–22.6) or rhinorrhea (OR, 5.7; 95% CI, 2.09–15.4) on the anesthesia day increased the occurrence of overall perioperative adverse events. The use of a supraglottic airway instead of an endotracheal tube (OR, 0.53; 95% CI, 0.339–0.83) and increased time interval between COVID-19 and anesthesia (OR, 0.77; 95% CI, 0.63–0.94) were associated with the decreased occurrence of overall perioperative adverse events.
Table 4
Univariate and multivariate analysis of the risk factors associated with overall perioperative adverse events
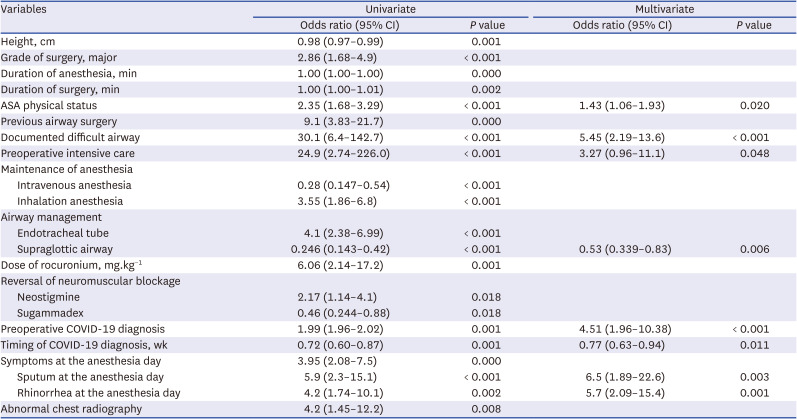
Table 5 demonstrates the patient characteristics and overall perioperative adverse events in symptomatic (n = 51) and asymptomatic (n = 445) patients in the COVID-19 group. Symptomatic patients had a higher incidence of PRAEs (OR, 3.95; 95% CI, 3.87–4.03) and desaturation events (OR, 4.4; 95% CI, 4.3–4.5) than asymptomatic patients, whereas no difference was observed in escalation of care or mortality (P < 0.492). Symptomatic patients were more likely to develop crackle or wheezing (OR, 13.8; 95% CI, 13.1–14.7), copious secretion (OR, 11.7; 95% CI, 11.3–12.2), high PIP (OR, 2.79; 95% CI, 2.71–2.87), airway obstruction (OR, 3.35; 95% CI, 3.23–3.46), and desaturation during emergence from anesthesia (OR, 9.8; 95% CI, 9.4–10.1).
Table 5
Patient characteristics and overall perioperative adverse events of patients with preoperative COVID-19 omicron infection by the symptoms on the anesthesia day
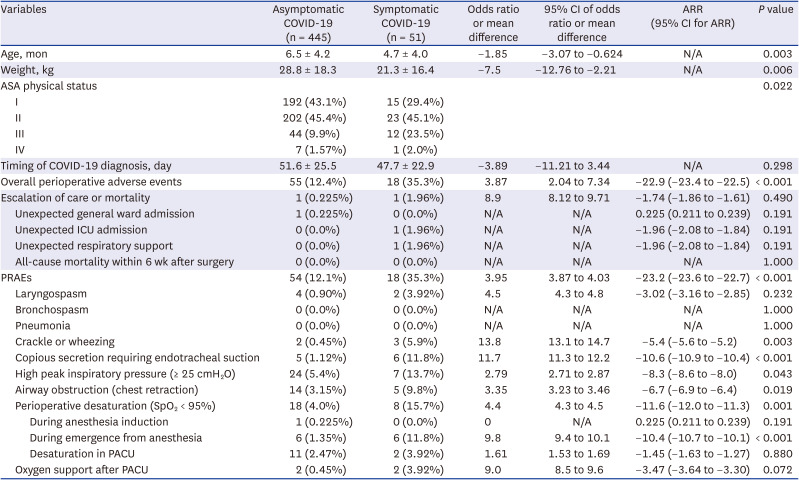
Values are mean ± standard deviation or number (proportion).
COVID-19 = coronavirus disease, CI = confidence interval, ARR = absolute risk reduction, N/A = not applicable, ASA = American Society of Anesthesiologists, ICU = intensive care unit, PRAEs = perioperative respiratory adverse event, PACU = post-anesthesia care unit.
DISCUSSION
Our retrospective, single-center, observational study showed that pediatric patients with preoperative COVID-19 omicron variant had a higher incidence of overall perioperative adverse events than non-infected matched controls. An increased time interval between diagnosis with COVID-19 omicron variant and anesthesia was associated with a decreased risk of PRAEs, including high PIP and longer PACU stay. However, the incidences of desaturation and escalation of care were not different, and no patients with preoperative COVID-19 omicron variant showed mortality within 6 weeks from anesthesia.
PRAEs are experienced by approximately 15% of pediatric patients receiving general anesthesia.1122 Airway hyper-responsiveness, copious secretions, flow obstruction, and atelectasis are considered the underlying mechanisms for PRAEs.1123 Preoperative intranasal dexmedetomidine,20 use of a short-acting beta-2 agonist,24 gentle suctioning,23 alveolar recruitment,25 and high-flow nasal oxygenation26 are helpful techniques to prevent PRAEs. With risk factors such as a recent URTI and asthma, the incidence of PRAEs increases to as high as 40–50% and serious complications can occur.11192022 In the present study, children within 2 weeks after diagnosis with the COVID-19 omicron variant (35.7%) or those who are symptomatic (35.3%) showed comparable incidence of PRAEs with that in previous studies.111922 However, the incidence of escalation of care or mortality was very low in both groups, showing relatively low severity.45
The incidence of PRAEs during anesthesia induction and airway management was rare (0.2%) in the present study compared with that in a recent study in which both intravenous and inhalation agents were used for pediatric airway management (4.26% and 1.72% for patients with and without COVID-19, respectively).3 At our institution, anesthetic induction is always performed using intravenous agents, such as propofol. Propofol, compared with sevoflurane, has the advantage of reducing the incidence of PRAEs during anesthesia induction in pediatric patients with risk factors by blunting the mechanical stimulation of the airway, and it suppresses the laryngeal reflex.22
A large number of surgeries and procedures have been canceled or postponed owing to the COVID-19 pandemic.27 Along with neurologic, cardio-pulmonary, and oncologic conditions, delays in the treatment of diseases related to functional development and growth impact both patients and their family, leading to societal costs.27 Currently, most guidelines recommend delaying surgery for at least 7 weeks after COVID-19 based on high mortality and morbidity in adults infected with non-omicron COVID-19 strains.151628
Although it was constantly mentioned that the incidence and severity of postoperative complications in children were less than those in adults after COVID-19,212 there was no concrete evidence for pediatric anesthetic practice. Retrospective data in the early COVID-19 era in 2020 demonstrated that unexpected noninvasive ventilation, postoperative pneumonia, and mortality can occur after general anesthesia in pediatric patients with COVID-19.2310 However, the virus has mutated over time. The omicron variant has faster replication efficiency in the human bronchi but lower replication competence in the human lungs compared to the delta variant.29 Therefore, the omicron variant was more transmissible than the alpha or delta variants, but severe clinical outcomes were less frequent than those with other variants in pediatric patients.45 In the present study, the incidence of overall perioperative adverse events was comparable with that of URTI, and we observed relatively low severity after preoperative COVID-19 omicron diagnosis in pediatric patients.211192022
In agreement with the consensus on preoperative URTI, we suggest rescheduling elective surgery or procedures for children within 2 weeks after a COVID-19 diagnosis or in those who have significant symptoms. In children diagnosed with COVID-19 2–6 weeks before anesthesia, the time from COVID-19 diagnosis, symptoms, clinical status, and comorbidities should be considered along with surgical urgency. Proactive risk management strategies, including intravenous induction with propofol, use of a supraglottic airway, and neuromuscular blockade monitoring, might helpful.
The present study shows the evaluating the risk of the COVID-19 omicron variant on pediatric general anesthesia for the first time.41314 Asymptomatic COVID-19 patients could be identified and included by robust and extensive screening tests before admission, and automatic alert of the electronic medical system by synchronization of nationwide database from KDCA.
Additionally, clinically relevant data on perioperative adverse events were collected from a wide range of ages and various departments in a comprehensive manner. We included detailed data on symptoms on the anesthesia day and PRAEs through high-resolution time-synchronized multi-parameter data from vitalDB18 and the “call for help” announcement and recording system at our institution.17 This study has some limitations. First, data were collected from a single tertiary pediatric center in Seoul, Korea, without ethnic diversity. No other country has shown mass omicron infections in the pediatric population (> 50% population) in such a short period (< 3 months). Second, elective surgery or procedure for patients with significant symptoms of COVID-19 would have been cancelled before anesthesia scheduling. Therefore, the risk of overall perioperative adverse events in symptomatic COVID-19 omicron cases may be underestimated. Third, the incidence of overall perioperative adverse events in non-COVID-19 patients with URTI was not compared with the COVID-19 group. Fourth, patients who underwent cardiac surgery, airway surgery, or suspension laryngoscopy, which are known to carry a higher risk of desaturation, were excluded from this study. By excluding such cases, the study aimed to focus specifically on the association between COVID-19 and PRAE, ensuring that observed events were more likely attributable to the patient’s history of COVID-19 infection rather than the surgical procedures. Lastly, as the study period was immediately after mass infection, the effect of long COVID-19 remains unknown.
In conclusion, although pediatric patients diagnosed with the preoperative COVID-19 omicron variant have an increased risk of overall perioperative adverse events. Care should be taken while deciding elective surgery or procedure for children within 2 weeks after COVID-19 or who have significant symptoms as the risk of occurrence of PRAEs is associated with.
 XML Download
XML Download