

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Endodontic treatment failure is often associated with inadequate root canal disinfection, inadequately filled root canals and inappropriate coronal restorations. Nonsurgical retreatment is usually the first treatment option if root canal treatment has failed. The first step in successful retreatment is the ideal removal of the root canal filling material [1]. Even though nickel titanium (NiTi) instruments with special designs and alloys have been proposed for retreatment, none can completely remove the filling material. Procedural errors during the nonsurgical retreatment of curved root canals may also compromise proper cleaning, disinfection, and refilling [2].
Various techniques can remove root canal filling materials, such as hand files, heated instruments, burs, ultrasonic tips, and rotary and reciprocating instruments [3]. In addition, rotary NiTi systems are specifically designed for retreatment procedures, including the ProTaper Universal Retreatment System (PTUR; Dentsply Maillefer, Ballaigues, Switzerland). PTUR includes 3 instruments with various tapers and diameters: D1, D2, and D3. The D1 (30/0.09) file has an active tip to facilitate the initial penetration into the gutta-percha. The D2 and D3 files have non-cutting tips and are used to remove the filling material from the middle and apical thirds, respectively. The inactive tips of D2 and D3 (25/0.08 and 20/0.07) files reduce the incidence of complications during the removal of filling materials [4]. Moreover, this system has a convex triangular cross-section. This system has been validated in straight root canals; however, information on the efficacy of these files in curved root canals is limited [5].
Reciprocal systems are now widely used for root canal preparation because they require less time, are easy to use, and usually allow the completion of preparation with a single file [6]. However, few studies have investigated the efficacy of these files during retreatment [7]. Innovations in the design, metal, and kinematics of endodontic instruments resulted in the development of new reciprocal single-file systems. Their improved mechanical properties, straightforward instrumentation protocols, and time-saving features have drawn the attention of researchers, particularly in relation to root canal filling removal [8]. WaveOne Gold (WOG; Dentsply Sirona, Ballaigues, Switzerland), a new reciprocating system, has been introduced. It differs from its predecessor, WaveOne, in terms of taper, design, size, and manufacturing processes. The WOG features a parallelogram cross-sectional design, 2 cutting edges, and 4 instruments, designated as 20/0.07 (small), 25/0.07 (primary), 35/0.06 (medium), and 45/0.05 (large). The file undergoes a gold wire thermal process, involving multiple cycles of heating and cooling, which results in its distinctive gold color [9]. Although the root canal shaping effect of WOG has garnered significant interest, its effectiveness in removing filling materials from curved root canals is limited [1011].
Retreatment techniques alone are not generally successful in completely removing root filling materials. Therefore, supplementary techniques have been proposed to increase the cleanliness of root canals during retreatment. Considering the limitations of instruments in removing filling material from the root canal, newer approaches as supplementary steps are currently being proposed [12]. The XP-Endo Finisher (XPF; FKG Dentaire, La Chaux-de-Fonds, Switzerland) has recently been shown to enhance the removal of root canal fillings [13]. When the XPF is inserted 7–8 mm into the root canal, the natural contractions and expansions cause the bulb and tip to enlarge and contract. Consequently, the XPF enables the removal of more residual material from the canal walls [13]. The Self-Adjusting File (SAF; ReDent Nova, Ra’anana, Israel) combines irrigation and preparation and is designed for minimally invasive treatment. This instrument offers a novel method for removing residual filling material, thanks to its scraping motion combined with continuous irrigation [14].
Erbium lasers have recently been used in many areas of dentistry and endodontics [15]. More specifically, erbium: yttrium, aluminium garnet (Er:YAG) as well as erbium, chromium: yttrium, scandium, gallium garnet (Er,Cr:YSGG) lasers have wavelengths of 2,940 and 2,780 nm, respectively. The wavelengths of both erbium lasers have the advantage of higher absorption in water than is the case for other lasers [16]. In one study, Er,Cr:YSGG lasers were reported to clean root canal walls more effectively due to their high affinity for hydroxyapatite and water [17]. However, no studies have demonstrated the efficacy of the Er,Cr:YSGG laser as an additional method during retreatment.
There is still no consensus in the literature on whether single or multiple file systems are more effective, or if supplementary methods enhance the cleaning of root canal walls in terms of residual filling materials, particularly in curved canals. Additionally, the volume of the root canal post-retreatment is often overlooked. Therefore, this study aims to compare the effectiveness of WOG and PTUR in removing root canal filling material from severely curved root canals. It also seeks to evaluate the potential adjunctive effects of XPF, SAF, and Er,Cr:YSGG laser using micro-computed tomography (μCT). Another objective is to assess the volume of the root canal following retreatment procedures with file systems and supplementary methods. The null hypotheses (Ho) tested were that: (i) there would be no differences in canal filling removal between PTUR and WOG; (ii) supplementary methods for removing residual filling materials would not have a positive impact; (iii) there would be no differences in the removal of residual filling material among XPF, SAF, and Er,Cr:YSGG laser; and (iv) there would be no differences in dentin removal between the retreatment techniques and among the supplementary methods.
MATERIALS AND METHODS
The sample size was calculated using Statistica 8.0 statistical software (StatSoft, Tulsa, OK, USA) with the F-test family for 1-way analysis, setting the following parameters based on Helvacioglu-Yigit et al. [18]: minimum = 0.03; maximum = 0.31; sigma = 0.14, and statistical power = 85%. Thus, the minimum sample size was determined to be 9 for each group, and 11 samples were used for each group.
Sample selection and preparation
This study was approved by the Ethics Committee of Suleyman Demirel University (No. 72867572/050/22780) and the study was performed at the Faculty of Dentistry of Suleyman Demirel University in Isparta, Turkey. In total, 175 extracted human mandibular first molar teeth were examined under a dental operating microscope. The inclusion criteria were closed apices, severe curvature (30°–40°), and caries-free mesiobuccal roots of 2 rooted mandibular molars. Each molar was radiographed from the mesiolingual and buccolingual directions to confirm the presence of 2 separate canals in the mesial root. Mesiobuccal root canal curvature was measured on radiographic images with AutoCAD software (Autodesk, San Rafael, CA, USA) according to the Schneider method [19]. Sixty-six mandibular first molars with mesiobuccal canals with severe root canal curvature (30°–40°) and an initial apical size equivalent to a size 10 K-file were selected. Mandibular molar teeth that had calcifications, previous endodontic treatment, caries, internal or external resorptions, cracks, additional canals, and calcifications were excluded. Subsequently, the teeth lengths were set to 14 mm by removing the coronal tooth structure. The position of the apical foramen was inspected with a stereomicroscope at ×40 magnification. A single operator performed the access cavity preparation, chemo mechanical preparation, obturation, and retreatment procedures.
ProTaper Universal instruments (Dentsply Maillefer) were used up to file F2 at the working length (WL). A size 10 K-file was inserted between each instrument to provide apical patency, and the canals were irrigated with 2 mL of 2.5% sodium hypochlorite (NaOCl) between each file change. The final irrigation was applied with 2 mL of 2.5% NaOCl and 2 mL of 17% ethylenediaminetetraacetic acid, followed by 5 mL of saline. The root canals were dried with ProTaper F2 paper points, obturated with ProTaper F2 gutta-percha and AH Plus sealer (Dentsply DeTrey, Konstanz, Germany) using a single-cone technique. The quality of the root canal filling was verified by mesio-distal and bucco-lingual periapical radiographs and Cavit (ESPE, Seefeld, Germany) was used to seal the access cavities temporarily. The teeth were incubated at 37°C in 100% humidity for 14 days to allow the root canal sealer to set.
At first, samples were divided into 2 groups according to the retreatment technique (PTUR, WOG) (n = 33) and then into 3 based on the supplementary method (XPF, SAF, and Er,Cr:YSGG laser) (n = 11) using a block randomization method.
Initial μCT scan
The samples were scanned using μCT (SkyScan 1174, Bruker micro-CT; Bruker, Kontich, Belgium) with the following parameters: 33 μm isotropic resolution, 50 kV, 800 μA, pixel size of 33 μm, beam hardening correction of 30%, smoothing of 2, and ring artefact correction of 4. Scanning was performed by 360° rotation around the vertical axis with a rotation step of 0.7, frame averaging of 3, random movement of 10, and camera exposure time of 2,500 ms.
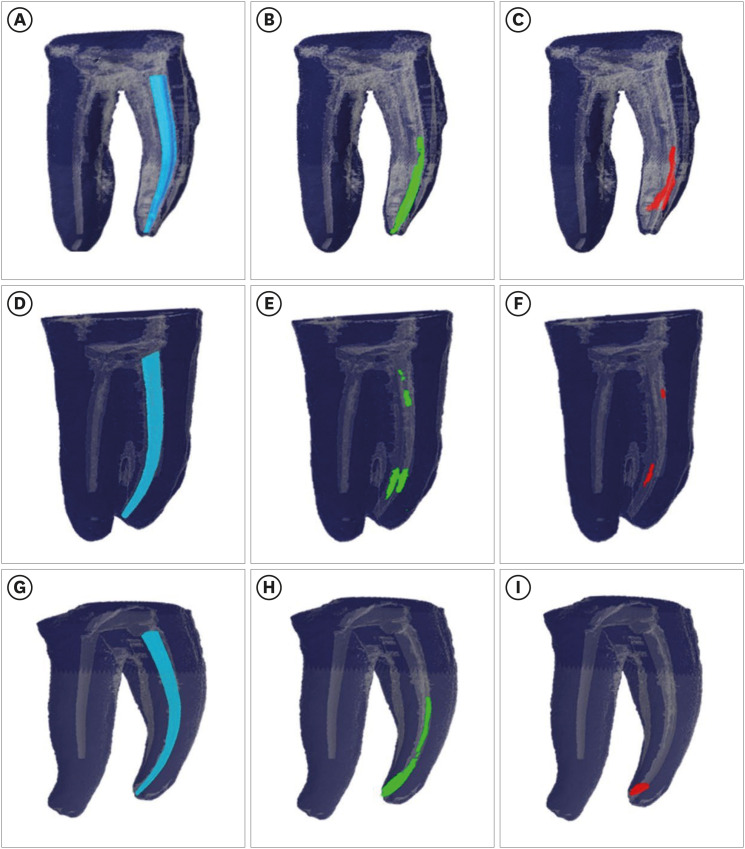
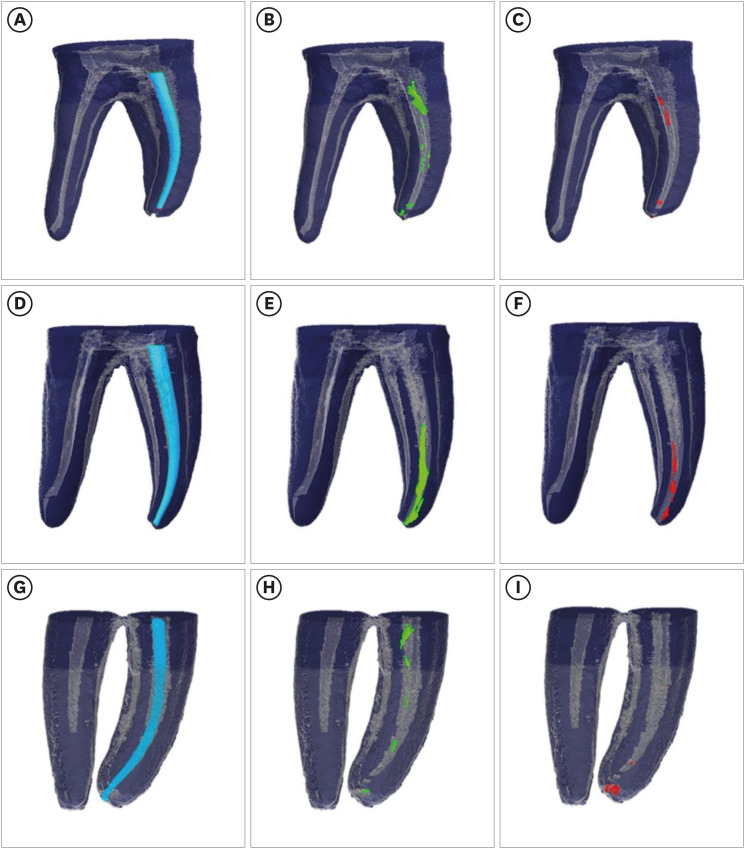
The original grayscale images were processed, the volume (mm3) of the root canal (initial canal volume; ICV) and the root canal filling (initial filling volume; IFV) were calculated. Grayscale thresholds were described to differentiate dentin from the canal filling material. A region of interest was selected for each slice to allow the calculation of the volumes of the root canals and filling materials (Figures 1 and 2).
Retreatment techniques
Retreatment procedures were performed with either PTUR or WOG. After the temporary fillings were removed, 0.1 mL of orange oil was introduced into the pulp chamber for 3 minutes. All procedures were conducted using X-Smart (Dentsply Maillefer). Each instrument was used for 2 canals only. The file separations and deformations that occurred during the operation were recorded.
1. PTUR (n = 33)
A D1 file was used in the coronal third, followed by a D2 file in the middle third. The filling material in the apical third was removed with a D3 file (20/0.07) with slight apical pressure at the WL. The operation time (T1) was recorded. Finally, the D2 file was used at the WL again until there was no filling material on the instrument, and the operation time (T2) was recorded. All the files were used at a constant speed of 500 rpm with 3 Ncm torque. The root canals were irrigated with 2 mL of 2.5% NaOCl between each file, and 10 mL of 2.5% NaOCl was used as final irrigation.
2. WOG (n = 33)
WOG primary files (size 25/0.07) were used in the reciprocating program “WaveOne ALL,” with gentle apical pressure and a brushing movement. After 3 movements of at most 3 mm amplitude, the file was removed and cleaned with sterile gauze and then inspected to detect any distortions. The root canals were irrigated with 2 mL of 2.5% NaOCl after every 3 mm of up-and-down movement in the WOG group. The procedure was repeated until the WL was reached and the operation time (T1) was recorded. The retreatment procedure was accepted as complete when no filling material was observed on the file, and the operation time (T2) was recorded. 10 mL of 2.5% NaOCl was used as final irrigation.
Supplementary methods
1. XPF (n = 11)
The XPF was operated with an electric motor (X-Smart) at 800 rpm constant speed and a torque of 1 Ncm using in-and-out motions with an amplitude of 7 to 8 mm for 60 seconds. The XPF was cooled with a cold spray (Frigofast, Calderara Di Reno, Italy) to keep the file straight for setting the WL. The canals were irrigated with 5 mL of 2.5% pre-warmed (37°C) NaOCl during this procedure, and final irrigation was performed using 5 mL of 2.5% NaOCl.
2. SAF (n = 11)
The SAF with a diameter of 2.0 mm was operated in the RDT3-NX handpiece (NSK, Tokyo, Japan) at a frequency of 83.3 Hz, speed of 5,000 rpm and amplitude of 0.4 mm with gentle vertical vibrations at the WL and continuous irrigation flow of 5 mL/min. The SAF was activated for 2 minutes under simultaneous irrigation with 2.5% NaOCl delivered by the EndoStation peristaltic pump (VATEA; ReDent Nova).
3. Er,Cr:YSGG laser (n = 11)
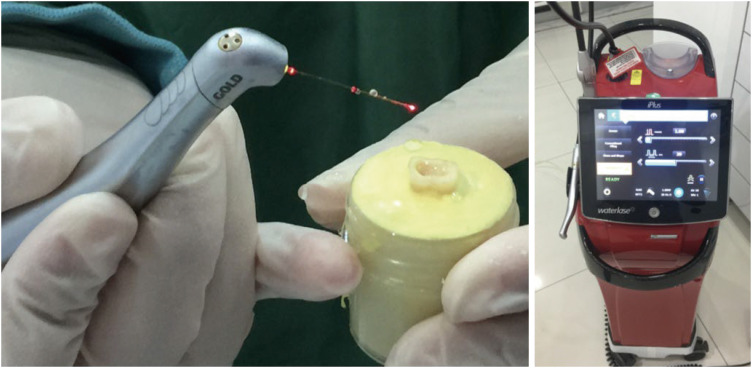
The Er,Cr:YSGG laser (2,940 nm, Waterlase; Biolase, San Clemente, CA, USA) at 1.5 W with a pulse duration of 140 µs and a frequency of 20 Hz was delivered with a 25-mm-long fiber optic tip (RFT2; Biolase). The air and water options were closed, and the laser was activated after the tip of the optic fiber was adjusted to the WL. The tip was used to circulate the entirety of the canal walls with helical movements in an apico-coronal direction. The laser was deactivated for 10 seconds after every 10 seconds of active use. The procedure was repeated for a total of 2 minutes with continuous irrigation with 10 mL of 2.5% NaOCl (Figure 3).
Statistical analysis
The differences between IFV and FV1, IFV and FV2, and FV1 and FV2 were statistically analyzed using the t-test. The volumes of filling material before and after preparation were compared between groups (PTUR or WOG) by analysis of covariance (ANCOVA). The t-test was used to compare the percentage of residual filling between the 2 retreatment techniques.
The supplementary step with XPF, SAF, or Er,Cr:YSGG laser was evaluated by comparing data from the filling material volumes before and after these procedures using ANCOVA. The significance among the supplementary methods in terms of percentage of residual filling was statistically analyzed with factorial analysis of variance.
The differences between ICV and CV1, ICV and CV2, and CV1 and CV2 were statistically analyzed using the t-test. ANCOVA was used to compare PTUR and WOG, and to evaluate any differences among the supplementary methods in terms of CV2. Then, the post hoc Tukey test was used to compare the supplementary methods in terms of CV.
The differences in time required to reach the WL (T1) and total removal time (T2) between PTUR and WOG were statistically analyzed with the Mann-Whitney U test. The significance level established for all analyses was 5% (p < 0.05).
RESULTS
The mean IFV before retreatment was similar for all samples (p > 0.05). None of the samples exhibited total removal of the filling material following the retreatment techniques and additional methods. Both PTUR and WOG reduced the volume of canal filling material (p < 0.01), and the mean residual volume of the filling material significantly decreased in all samples subjected to the additional methods (p < 0.01).
The mean volume (mm3) and standard deviation (mm3) of residual filling after the retreatment techniques and supplementary methods are detailed in Table 1. WOG resulted in 81.52% reduction of the filling mass, while PTUR removed a mean of 81.98%. The differences between the retreatment techniques were not statistically significant (p > 0.05).
Table 1
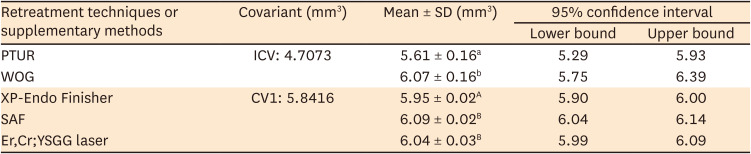
The volumes (mm3) of residual filling material after retreatment techniques and supplementary methods
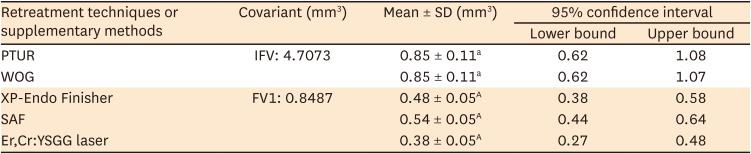
SD, standard deviation; IFV, initial filling volume; PTUR, ProTaper Universal Retreatment; WOG, WaveOne Gold; SAF, Self-Adjusting File; FV1, filling volume 1; Er,Cr:YSGG, erbium, chromium: yttrium, scandium, gallium garnet.
Different letters indicate a statistically significant difference (p < 0.01).
The average percentage of the residual FV removed was 42.86% for the XPF, 36.38% for the SAF, and 55.23% for the Er,Cr:YSGG laser following the retreatment techniques.
Table 2 displays the mean values for ICV, CV1, and CV2. All retreatment techniques and additional methods resulted in an increase in root CV (p < 0.01). WOG removed significantly more dentin than PTUR (p < 0.01) (Table 3). The XPF resulted in less reduction in dentin than the SAF and the Er,Cr:YSGG laser when CV1 was taken as the covariant (p < 0.01) (Table 3).
Table 2
The volume (mm3) of initial root canals (initial canal volume, ICV), after the retreatment technique (canal volume 1, CV1), and the supplementary method (canal volume 2, CV2)

| Root canal volumes | Mean ± SD (mm3) | p value |
|---|---|---|
| ICV | 4.71 ± 1.17a | < 0.01 |
| CV1 | 5.84 ± 1.39b | < 0.01 |
| CV2 | 6.03 ± 1.40c | < 0.01 |
Table 3
The volume (mm3) of root canals after the retreatment technique and supplementary method
WOG was faster than PTUR in terms of reaching the WL (73.06 seconds and 132.58 seconds, respectively) and total removal time (122.45 seconds and 170.75 seconds, respectively) (p < 0.01) (Table 4).
Table 4
Time to reach working length (T1) and removal of canal filling material (T2) with ProTaper Universal Retreatment (PTUR) and WaveOne Gold (WOG) systems

| Time (sec) | File system | Means ± SD (mm3) | p value |
|---|---|---|---|
| T1 | PTUR | 132.58 ± 70.28a | < 0.01 |
| T2 | PTUR | 170.75 ± 44.21b | < 0.01 |
| T1 | WOG | 73.06 ± 20.37A | < 0.01 |
| T2 | WOG | 122.45 ± 27.54B | < 0.01 |
No file separation or visible deformation was observed during the retreatment procedures or supplementary steps.
DISCUSSION
The inability to eradicate microorganisms from the root canal system often results in treatment failure. However, no existing techniques can fully remove root canal filling materials during retreatment [20]. In this study, none of the NiTi systems or supplementary methods were successful in completely removing canal filling material from the severely curved canals. Variations in root canal morphology, intracanal ramifications, and root canal curvatures heighten the risk of procedural errors during endodontic treatment. The curved mesial canals and concave distal surfaces of mandibular molar teeth have been identified as potential risk factors for strip perforation and root fractures. Consequently, mesial root canals of mandibular molars carry a high risk of complications, making it challenging to achieve ideal endodontic treatment [21]. In the present study, severely curved (curvature of 30°–40°) mesio-buccal root canals of mandibular molar teeth were used to simulate the difficult conditions of retreatment procedures.
The first null hypothesis of this study was accepted, because the single-file system (WOG) and the multiple-file retreatment system (PTUR) demonstrated similar efficiency in removing root fillings. The comparison of the efficacy of multiple-file rotary instruments and single-file reciprocal systems for retreatment procedures has been a point of interest for many researchers, including ourselves [2223]. PTUR is specifically designed to extract filling materials from root canals, utilizing cutting edges, grooves, and varying tapers and lengths. A comparison of Reciproc, PTUR, and Hedström files in curved root canals using μCT revealed no significant differences [22]. Both Reciproc and WaveOne were found to be as effective as PTUR [23]. Limited data have been reported concerning the retreatment capabilities of the WOG system. Although the WOG system is manufactured with a more flexible NiTi gold-wire and a different taper, tip, and parallelogram section design compared to WaveOne, its ability to remove filling material was found to be similar [24]. A recent study reported that the PTUR, WOG, Reciproc, and Reciproc Blue systems were equally effective in removing filling materials from curved root canals [25]. However, the performance of the WOG system was found to be inferior to the other 2 files operating with full rotation in oval root canals. This was attributed to the design of the WOG system, which may not provide sufficient space for debris removal, potentially leading to inadequate cutting efficiency [26].
The PTUR instruments, thanks to their unique convex triangular groove design and kinematic rotation, generate friction heat that plasticizes the gutta-percha. This allows the gutta-percha to be drawn into the file’s grooves, effectively removing it. Moreover, the D1 file features an active cutting tip for the initial penetration of the gutta-percha in the root’s coronal third. Concurrently, the cross-sectional design of PTUR files facilitates the removal of large quantities of gutta-percha [5]. Therefore, the decision to use the PTUR file system for retreatment was based on these superior design features. The system’s ability to remove root canal fillings has been validated by existing literature [23]. A comparison with the WOG file system was sought, but the literature provides limited information on its use in retreatment [11].
Utilizing a single instrument during retreatment may expedite the process of removing root canal filling material. Moreover, the NiTi heat treatment procedure and the inactive tip of the WOG can potentially make gutta-percha removal safer compared to using retreatment files. However, the high flexibility inherent in this system, due to heat treatment and the lack of an active tip, may pose challenges for the file to penetrate the gutta-percha. Consequently, the decision to use the WOG file system for gutta-percha removal was based on limited information regarding the use of the WOG for retreatment [11].
The superior efficacy of PTUR for retreatment procedures has been well-documented [13]. This performance was attributed to the system’s cross-sectional design features, the D1 instrument’s excellent ability to penetrate gutta-percha, and the consistent taper of the files. The efficiency of the Reciproc and PTUR file systems was evaluated by sectioning in straight root canals, and it was found that PTUR left fewer remnants of gutta-percha and sealer [23]. However, these systems did enlarge the apical size beyond the initial apical size (#50). Therefore, widening the apical width can significantly improve the cleaning of the root canal wall [25].
The second null hypothesis of this study was rejected because the supplementary methods improved the removal of residual filling materials, as has been demonstrated in the other studies [2]. The absence of a significant difference in the removal of residual canal filling among the 3 supplementary methods resulted in the acceptance of the third hypothesis.
It has been reported that XPF is effective for cleanliness due to the file’s ability to expand at body temperature, move in a helical pattern, and effectively remove residual filling material [2]. The volume of residual filling left after additional preparation with an XPF file was reported to be 0.48 mm, a finding that aligns with the results of the present study [27].
While the SAF is highly flexible, it lacks the ability to penetrate, making it unsuitable for standalone use in removing canal filling materials. However, numerous studies have shown that when used in conjunction with other methods, the SAF can effectively clean residual filling materials by brushing against the canal walls, a finding that is consistent with our current study [28].
Erbium lasers possess a high absorption capacity in water, which results in a reduced thermal impact on the periradicular tissues compared to other lasers. The Er:YAG laser has been used either independently or as an additional step in the removal of filling materials [29]. However, only one study in the literature has considered the use of the Er,Cr:YSGG laser for the removal of residual obturation materials [30]. Lasers can eliminate root canal filling materials through photoablation and photothermal effects. The energy of the Er,Cr:YSGG laser is absorbed by water or irrigation solutions when the laser device’s water option is set to ‘open,’ separating gutta-percha from the root canal walls. This is known as the photoablation effect. Additionally, the filling material undergoes carbonization due to laser application, a process known as the photothermal mechanism [29]. Using the Er,Cr:YSGG laser at 1 W in root canals resulted in a temperature increase of 3.84°C around the root surface, but this increase is not sufficient to cause irreversible damage [31]. A recent study showed the formation of carbonizations and cracks with a higher laser power (3.0 W). Therefore, a power of 1.5 W was used in the current study. To mimic the irrigation protocol under standard clinical conditions and to ensure consistency across all supplementary methods, NaOCl was used as an irrigant in this study. Laser-activated irrigation with erbium lasers has been shown to enhance the cleaning of the root canal system due to the creation of intense turbulent flow. It has been reported that the additional use of the Er,Cr:YSGG laser improved canal wall cleaning following retreatment procedures with PTUR instruments, a finding that was also observed in the current study [32]. It was also demonstrated that the Er,Cr:YSGG laser was more effective in the coronal and middle thirds than in the apical third. This was attributed to the circular movement of the fiber tip in the coronal and middle thirds, while a parallel movement was used in the apical area. The amount of remaining canal filling material on the entire root canal wall was evaluated in this study. The researchers concluded that the removal of root filling material in the apical third is more challenging for all supplementary methods.
The fourth null hypothesis of this study was dismissed due to observed differences in dentin removal between the retreatment techniques and the supplementary methods. While there were no significant disparities in the removal of filling material between PTUR and WOG, WOG was found to remove more dentin. Given that the study utilized curved and narrow mesio-buccal root canals of mandibular molars, size 25 was selected for the apical third in both systems to assess the effectiveness of the supplementary methods. Achieving effective chemical disinfection, through irrigation and medication, is crucial. This is largely tied to the success of canal preparation and the development of root canal shaping that enables a new, high-quality obturation. However, excessive dentin removal from the root canal could potentially lead to vertical root fracture or perforation, thereby weakening the root [33]. The existing literature includes studies indicating that reciprocal instruments may remove excessive dentin during root canal preparation. Yet, no significant differences were found between PTUR and Reciproc in terms of the volume of dentin removed during root canal retreatment [22]. These results diverge from those of the current study, a discrepancy that could potentially be explained by operator-dependent factors such as the intensity of the brushing motion or the duration of the working time.
It has been claimed that the shape of the root canal molds the XPF to its form. The instrument’s tip and bulb scrape the root canal. Given that the XPF is a non-tapered instrument and purports to cleanse the root canal walls while preserving their original shape, fewer volumetric changes were observed in the root canal wall compared to other adjunctive methods during retreatment. Although the SAF showed comparable efficiency in cleaning the root canal wall, it expanded the root CV more than the other techniques (p > 0.05). This can be attributed to the SAF’s extreme flexibility due to its design, which prevents it from adequately penetrating the filling material. However, it excels at dentin removal [34]. The Er:YAG laser was utilized at 30, 40, and 50 mJ for retreatment procedures, resulting in 2.4%, 2.1%, and 2.6% changes in the CV, respectively [29]. However, these results could not be compared with the findings of the current study due to the supplementary use of lasers.
In this study, the working time incorporated the duration of irrigation, the cleaning of dentin chips and filling materials on the file, and the replacement of the D1, D2, and D3 files, all to mimic a clinical setting. WOG was significantly faster than PTUR, which used 3 instruments. Clinicians have often preferred a single-file system due to its ability to streamline the instrumentation protocol and reduce operation time. Factors such as tooth anatomy, obturation technique and material, retreatment technique, use of solvents, the number of files used, and the clinician’s experience can all influence the working time. While it has been shown that applying a solvent in the initial stages of preparation can reduce operation time, the results of this study align with previous literature that did not use a solvent [2226]. Previous studies have also demonstrated that the use of a solvent does not enhance root canal cleanliness [3536].
As an alternative, orange oil is advantageous for removing root canal fillings due to its biocompatibility and effectiveness with root canal sealers that contain epoxy resin and calcium hydroxide. This solvent also has advantages such as being non-harmful to health, possessing a pleasant scent, and being utilized in the production of pharmaceutical fragrances. There is no evidence of it being carcinogenic or genotoxic. Moreover, orange oil is less cytotoxic and more biocompatible than eucalyptol and chloroform, and it results in less root canal transportation than chloroform [37]. Oyama et al. [38] revealed that orange oil was more effective than chloroform for retreatment. However, Salgado et al. [39] showed that the use of orange oil was associated with an increase in root canal filling remnants. They attributed this situation to the use of a solvent, which has disadvantages for canal cleaning and the contamination of gutta-percha and paste on the canal walls due to the use of solvents during retreatment. Rodrigues et al. [40] evaluated the efficiency of gutta-percha removal, similar to our study. They applied orange oil only at the cervical level in the pulp chamber. In our study, a small quantity of orange oil was introduced into the pulp chamber to soften the gutta-percha and facilitate the penetration of instruments.
Vertical root fractures often lead to tooth extraction and are a significant issue in many teeth that have undergone endodontic treatment. The formation of microcracks in the dentin and subsequent risk of vertical root fracture can be influenced by various characteristics of NiTi file systems, such as their cross-sectional shape, geometry, taper, apical diameter, and kinematics [41]. The XPF system, specifically designed for 3-dimensional shaping of root canals, is noteworthy. This system, according to the manufacturer, is prefabricated using the NiTi MaxWire alloy, which provides superior flexibility and adaptability to irregularities in the root canal. Furthermore, its taperless production prevents dentin defects from root canals [13]. To our knowledge, there is no existing information regarding dentin crack formation following the use of XPF. In this study, we found that XPF caused the least change in root CV compared to 2 other systems. This could be attributed to XPF’s lower risk of causing microcracks and vertical root fractures. In contrast, the SAF system cleans the duct using an in-and-out motion, which helps prevent stress formation along the root canal [14]. The present study showed that the SAF removed more dentin than the XPF. When comparing the 3 systems, the SAF and Er,Cr;YSGG laser systems appear to pose a higher risk for vertical root fractures. Papoulidou et al. [15] reported that the Er,Cr:YSGG laser group had nearly half the number of newly formed microcracks compared to the ultrasonic group after laser and ultrasonic applications. In the present study, we observed a slight increase in dentin volume after the Er,Cr:YSGG laser application compared to the other 2 cleaning techniques. This could be significant in terms of the risk of vertical root fractures. A systematic review reported that there was no difference in the removal efficiency of root canal filling between rotary and reciprocal files, and the results are in agreement with the results of our study [42].
The key strengths of this study included the comparison of entirely distinct supplementary methods and the assessment of extracted dentin during the retreatment process. However, the study had certain limitations. One such limitation was that the quantity of remaining filling material was not separately evaluated for each third of the root canal. Additionally, all retreatment procedures could have been conducted at 37°C within a cabinet to better mimic oral conditions.
CONCLUSIONS
The PTUR and WOG systems demonstrated equal effectiveness in removing root canal fillings from severely curved root canals. However, the WOG system resulted in a more significant increase in root CV. While supplementary techniques enhanced the removal of filling material, none were able to completely clear the root canals of root fillings. The XPF should be viewed as a viable option, particularly for retreatment cases in curved root canals, as it resulted in only a minimal change in root CV. The clinical significance of this study lies in the potential for supplementary methods to improve root canal cleanliness following conventional retreatment procedures.
 XML Download
XML Download