

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Acute cholecystitis (AC) is a prevalent hepatobiliary disease that requires definitive surgical management, and laparoscopic cholecystectomy (LC) has been established as the standard treatment for AC. Since the inception of the Tokyo Guidelines in 2007, the management approach for AC has been determined based on the severity grade, ensuring the selection of appropriate treatment strategies [1]. The Tokyo Guidelines 2018 (TG18) offers essential recommendations for optimal management of AC, serving as a valuable reference for clinicians in their decision-making process regarding suitable treatment modalities for patients with AC [2]. According to the TG18, early LC may be considered for patients with moderate AC who have low morbidities, especially in cases where advanced LC management is available [345]. Furthermore, the TG18 suggests that early LC is feasible for patients with severe AC who exhibit favorable organ system failure (FOSF) and do not present negative predictive factors [6].
Percutaneous transhepatic gallbladder drainage (PTGBD) has emerged as a crucial strategy in the management of patients with moderate and severe AC, as it effectively stabilizes the general condition of patients prior to surgical intervention [7]. The TG18 provides valuable recommendations for the management of AC and advocates for the use of PTGBD followed by elective or delayed cholecystectomy in patients with moderate or severe AC and a poor general condition unresponsive to antimicrobial therapy or general supportive treatment [8]. In moderate-to-severe AC patients, the presence of negative risk factors and FOSF are considered pivotal factors in the decision-making process for the choice between PTGBD or LC. Considering the advanced age and presence of severe comorbidities in patients undergoing PTGBD, it becomes crucial to mitigate the potential risks associated with LC and to effectively manage perioperative complications. However, adhering to the recommendations of the TG18 for early or urgent cholecystectomy poses challenges for many clinicians, primarily due to limitations in medical resources and infrastructure. Clinicians frequently opt for PTGBD as an initial therapeutic approach to mitigate inflammation in patients with moderate-to-severe AC followed by delayed cholecystectomy. However, this approach may lead to severe fibrosis and adhesion, which can complicate dissection during LC, resulting in high open conversion rates [9]. Several contentious issues surround the management of moderate-to-severe AC, including the timing of LC, indications for PTGBD, and the optimal approach for challenging LC cases [1011].
The guidelines undergo constant revisions to incorporate new findings from ongoing investigations. Therefore, the present study assessed the effectiveness of LC following PTGBD and the feasibility of early LC by comparing 2 distinct surgical approaches in patients with grade II or III AC.
METHODS
This retrospective study was approved by the Institutional Review Board of Samsung Medical Center (No. 2017-07-017), and the need for informed consent was waived. All methods were carried out in accordance with the Declaration of Helsinki.
Patients and data collection
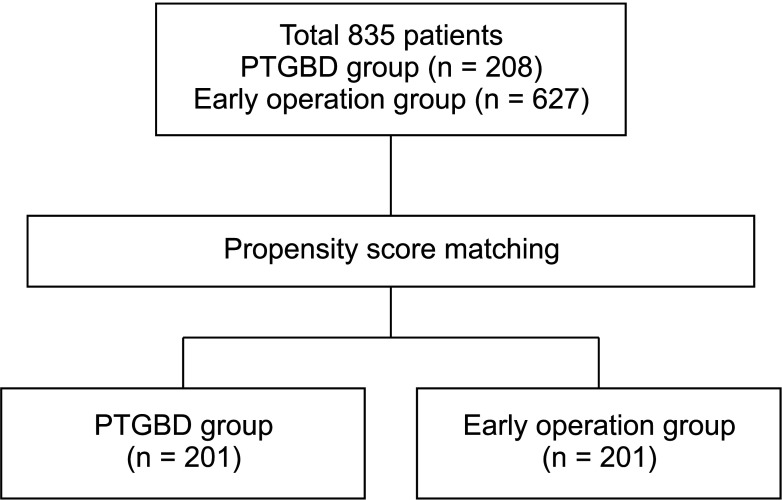
Prospective data were collected of patients who underwent LC for TG18 grade II and III AC at Samsung Medical Center, Seoul Metropolitan Government-Seoul National University Boramae Medical Center, Ajou University Hospital, and Inje University Ilsan Paik Hospital. Each participating institution consisted of 3–4 junior to expert senior hepato-biliary-pancreatic surgeons who were responsible for performing LC. Notably, the institutions had a substantial caseload, conducting 800 to 2,000 LC and over 100 PTGBD annually. This significant caseload aligns with the designation of “advanced center and expert surgeon” as referred to in the TG18. Data from January 2014 to December 2017 were systematically recorded in an electronic database. After obtaining Institutional Review Board approval, the data were retrospectively extracted and reviewed. A total of 835 patients who underwent LC for grade II and III AC were included in this retrospective study. The patients were initially divided into 2 groups: the delayed LC after PTGBD group (n = 201) and the early LC group (n = 627) (Fig. 1).
In the PTGBD group, all patients maintained drainage until the time of surgery, ensuring that the procedure was not concluded solely through aspiration. To minimize the selection bias inherent in retrospective analysis, we conducted 1:1 propensity score matching (PSM) [12]. After PSM, 201 patients in the PTGBD group and 201 patients in the early LC group were included in the final analysis.
Definitions
The diagnosis of systemic inflammatory response syndrome (SIRS), characterized by a systemic response to infection or other stimuli, entails the evaluation of laboratory findings and vital signs. Diagnosis of SIRS requires the presence of at least 2 of the following criteria: body temperature of >38℃ or <36℃, heart rate of >90 beats per minute, respiratory rate of >20 breaths per minute or PaCO2of <32 mmHg (4.3 kPa), WBC count of >12,000/mm3 or <4,000/mm3, or >10% immature bands [13]. The selection of these criteria was based on their ease of measurement and their established reliability as indicators of the systemic inflammatory response. The criteria used in this study were derived from standard values established through a comprehensive analysis of a large cohort study and have since been widely acknowledged and implemented in clinical practice. These selected values were deemed suitable for our study, as they offer a dependable and uniform foundation for the identification of SIRS cases.
Septic shock, a critical clinical condition, was defined as the presence of sepsis-induced hypotension that persists despite appropriate fluid resuscitation measures [13]. This definition is consistent with prevailing clinical guidelines and represents a widely adopted approach within the medical field for the diagnosis and treatment of sepsis-associated complications.
In this study, the definition of biliary complication was established in accordance with the widely recognized Strasberg classification system, which serves as a standard method for grading the severity of biliary complications [14]. This classification system incorporates factors such as severity and anatomical site of injury and encompasses various complications including biloma, bile leakage, and bile duct injury.
In this study, complicated cholecystitis referred to cases with preoperative imaging evidence of gangrenous cholecystitis, pericholecystic abscess, hepatic abscess, biliary peritonitis, and emphysematous cholecystitis. In accordance with the guideline, a waiting period of 4–6 weeks following PTGBD was observed before performing LC [2]. This interval between PTGBD and LC was deemed essential as it mitigates the heightened likelihood of complications associated with performing LC soon after PTGBD in patients at high risk. Prior to surgery, the patient underwent preoperative evaluations to assess cardiac and pulmonary function to determine their suitability for the procedure. The specific timing of the surgical intervention was ultimately determined by the surgeon’s discretion and considering the patient’s clinical condition. The primary outcome of interest was surgical outcomes, including the duration of hospitalization and the occurrence of intraoperative or postoperative biliary complications.
Statistical analyses
Statistical analyses were conducted to assess the differences in mean values with interquartile range between the 2 groups using independent t-tests. Differences in numbers and percentages between the groups were examined using the chi-square test or Fisher exact test. To explore the factors associated with postoperative hospital stay, a linear regression model was used. Univariable and multivariable logistic regression models were used to identify the risk factors associated with biliary complications. A linear regression model was used to assess the impact of variables on postoperative hospital stay. Statistical significance was defined as a P-value less than 0.05. Data analysis was conducted using IBM SPSS Statistics for Windows, ver. 25.0 (IBM Corp.).
RESULTS
Clinical characteristics
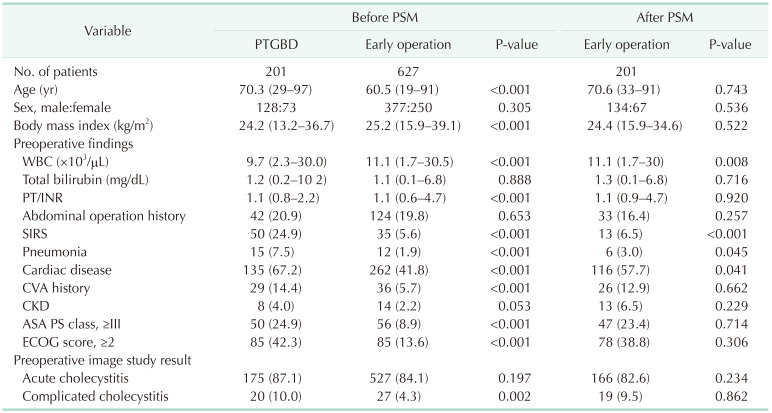
Analysis of the groups prior to PSM several notable differences in the PTGBD compared with the early LC group, as outlined in Table 1. These differences included a significantly higher mean age, lower body mass index (BMI), elevated serum white blood cell count, and higher prothrombin time/international normalized ratio (PT/INR) level. Additionally, the PTGBD group exhibited a higher prevalence of comorbidities, as evidenced by higher rates of SIRS, pneumonia, and cardiac disease and a larger proportion of complicated cholecystitis cases. Moreover, the PTGBD group displayed higher American Society of Anesthesiologists (ASA) physical status (PS) class and Eastern Cooperative Oncology Group (ECOG) scores. PSM was performed to address potential selection bias inherent in our retrospective analysis by accounting for covariates that were presumed to be determinants of such bias. The covariates used for matching were age, sex, BMI, high ASA PS class, high ECOG score, and presence of complicated cholecystitis. After PSM, no statistically significant differences in baseline demographic or clinical variables were observed between groups, except preoperative morbidity.
Postoperative outcomes
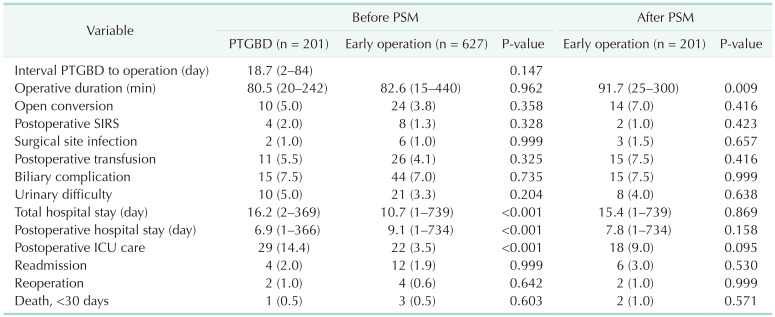
We compared postoperative outcomes between patients who underwent PTGBD and those who underwent early LC, considering their demographics and perioperative characteristics, as outlined in Table 2. In patients who underwent PTGBD, the median interval between PTGBD and LC was 18.7 days (range, 2–84 days). The early LC group exhibited a longer operation time compared with the PTGBD group (91.7 minutes vs. 82.6 minutes, P = 0.009). No significant differences were observed between the 2 groups regarding other postoperative complications, including open conversion rate (5.0% vs. 7.0%, P = 0.416), surgical site infection (1.0% vs. 1.5%, P = 0.657), postoperative transfusion (5.5% vs. 7.5%, P = 0.416), and biliary complication (7.5% vs. 7.5%, P = 0.999). The variables pertaining to hospitalization duration exhibited statistically significant differences between the 2 groups (P < 0.001). However, after PSM, no significant differences in these variables were observed between the groups. Furthermore, there were no significant differences in the reoperation rate (2.0% vs. 3.0%, P = 0.530) or 30-day mortality following LC (0.5% vs. 1.0%, P = 0.571).
Risk factor analysis for hospitalization duration and biliary complication
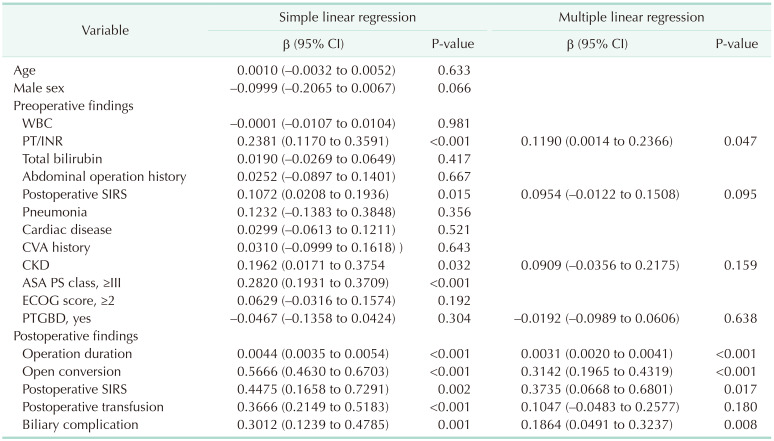
We conducted a risk factor analysis for hospitalization duration using linear regression models (Table 3). In the univariable analyses, several factors, including preoperative serum PT/INR, SIRS, chronic kidney disease, high ASA PS class, operation duration, open surgery, postoperative SIRS, transfusion, and biliary complication, were significantly associated with hospitalization duration. Furthermore, in the multiple linear regression model, preoperative serum PT/INR, operation duration, open surgery, postoperative SIRS, and biliary complication were significant risk factors for hospitalization duration. Preoperative PTGBD was not significantly associated with hospitalization duration in either the simple or multiple linear regression model (P = 0.304, P = 0.638).
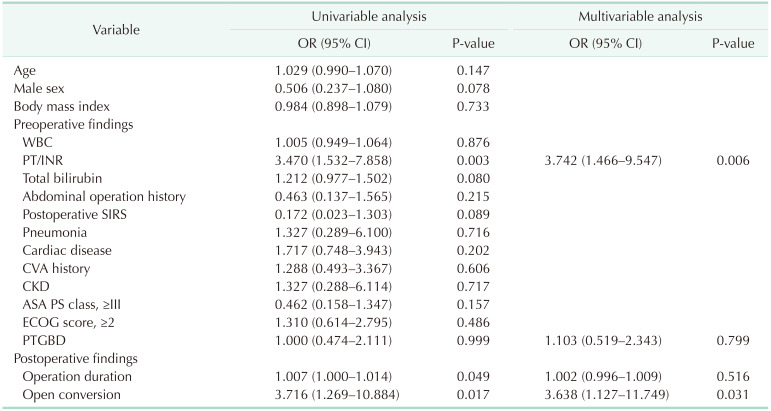
We also conducted a risk factor analysis for biliary complications (Table 4). In the univariable analyses, preoperative serum PT/INR, operation duration, and open conversion showed statistical significance. In multivariable analysis, preoperative serum PT/INR (odds ratio [OR], 3.742; 95% confidence inteval [CI], 1.466–9.547; P = 0.006) and open conversion (OR, 3.638; 95% CI, 1.127–11.749; P = 0.031) were independent prognostic factors of biliary complication. PTGBD was not significantly associated with biliary complication in either univariable or multivariable logistic regression models (P = 0.999, P = 0.799).
DISCUSSION
Surgical intervention for moderate-to-severe AC carries inherent risks of bile duct injury and prolonged hospitalization. The Tokyo Guidelines has been instrumental in assisting clinicians in navigating these challenges by providing recommendations for relatively early surgical intervention [2]. However, like the previous Tokyo Guidelines (TG13 and TG18), there is ongoing debate surrounding these recommendations. In our study, we assessed the feasibility of early surgery for moderate-to-severe AC based on these recommendations. Our analysis demonstrated no significant differences in postoperative complications and length of hospital stay between the early LC group and the PTGBD group. These findings are in line with the TG18, supporting the consideration of early surgery in well-equipped medical centers. Furthermore, our study revealed that patients who underwent LC following PTGBD experienced comparable surgical outcomes to those who underwent early LC, despite having multiple underlying medical conditions and factors that posed challenges to surgery. This finding highlights the favorable safety profile of LC after PTGBD in the context of advanced medical institutions. Notably, in current practice, it is considered safe to defer surgery until after PTGBD for patients with comorbidities and a higher risk associated with general anesthesia [15].
PTGBD is recognized as an adjunctive measure rather than a definitive solution for AC. Nonetheless, PTGBD has demonstrated the ability to improve patient survival rates and reduce complications associated with AC. In high-risk patients presenting with moderate-to-severe AC, elective LC following PTGBD has been found to yield comparable safety outcomes to early LC [16]. Furthermore, a study reported higher rates of conversion to open surgery, complications during LC, and mortality in the early LC group compared with the PTGBD group [17]. This suggests that the therapeutic efficacy of PTGBD followed by scheduled LC may be superior to that of emergency LC. Notably, numerous benefits have been observed, particularly among older individuals and those with multiple comorbidities [1819]. PTGBD performed prior to scheduled LC has been shown to effectively shorten operative duration, reduce intraoperative bleeding, decrease postoperative hospital stay, lower the rate of open conversion, and mitigate postoperative complications in elderly patients with AC. Based on these findings, PTGBD followed by scheduled LC is recommended as the preferred treatment strategy [20]. Our study findings further support the notion that, despite a higher prevalence of comorbidities in the PTGBD group, the surgical outcomes were not significantly inferior compared with those from early surgery, consistent with previous research. This indicates that performing LC following the correction of risks associated with comorbidities and general anesthesia through PTGBD is a safe approach.
In this study, associations between the two-operation strategy (PTGBD followed by LC and early LC) and postoperative outcomes, namely biliary complication and postoperative hospital stay, were examined using multivariable regression analyses. The analyses were adjusted for potential confounding factors including age, sex, BMI, high ASA PS class, high ECOG score, and complicated cholecystitis. Notably, preoperative WBC, SIRS, pneumonia, and cardiac disease were higher in the PTGBD group. However, these variables were considered unique characteristics of the PTGBD group and were not included in the PSM variables. Following PSM, our analysis revealed that the early LC group had a longer operative time compared with the PTGBD group. Furthermore, our analyses identified preoperative high PT/INR and conversion to open surgery as risk factors for biliary complications, while preoperative high PT/INR, operative time, postoperative SIRS, and biliary complications were identified as risk factors for increased length of hospital stay. Importantly, the presence of PTGBD was not a significant risk factor for biliary complications or increased length of stay. This finding underscores the notion that the severity of the disease itself carries more weight in determining the risk of biliary complications from early LC or LC after PTGBD. Therefore, the decision regarding timing of surgery should prioritize the patient’s comorbidities and their ability to tolerate surgery, rather than solely focusing on the presence of PTGBD.
In our study, the median interval between PTGBD and LC was 18.7 days. However, the optimal interval between PTGBD and LC has not been definitively established, and the current literature reports diverse and conflicting findings. Some studies have indicated that early LC performed within 1 week following PTGBD is both safe and effective, with similar intraoperative outcomes, postoperative complication rates, and rates of conversion to open cholecystectomy [21]. Furthermore, according to several other studies, the recommended timeframe for LC falls within the range of 7 to 26 days after PTGBD, and performing LC for severe AC within 216 hours after PTGBD was found to pose technical challenges and may be more difficult to accomplish successfully [2223]. Nevertheless, another study has reported that the interval between PTGBD and surgery has minimal impact on perioperative outcomes [24]. In a study focusing on grade II AC, early PTGBD did not improve surgical difficulty, and timing of subsequent LC was not correlated with surgical difficulties or postoperative outcomes [25]. Hence, the forthcoming revision of the TG guideline or the integration of recently published studies will likely play a crucial role in determining the outcome of this matter.
Numerous studies have investigated the use of LC and PTGBD in the management of moderate-to-severe AC, extending beyond the recommendations provided by the TG guidelines. Notably, in a recent study focusing on patients with moderate-to-severe AC after PTGBD, implementation of an aggressive approach involving subtotal cholecystectomy demonstrated an enhanced completion rate of laparoscopic surgery. Based on their findings, the authors concluded that laparoscopic subtotal cholecystectomy represents a viable and secure treatment option with favorable feasibility [26]. Another study aimed to develop a scoring system for predicting the need for a bailout procedure during LC following PTGBD and to assess the association between the scoring system and perioperative complications [27]. The objective was to provide a valuable tool for identifying patients at higher risk of requiring a bailout procedure and to evaluate the impact of the scoring system on perioperative outcomes. Furthermore, there have been studies focusing on non-surgical interventions. One such intervention is percutaneous transhepatic gallbladder aspiration, which is considered a simpler method for gallbladder drainage compared with PTGBD [28]. However, percutaneous transhepatic gallbladder aspiration has been associated with a higher risk of failure compared with PTGBD. Nevertheless, it offers advantages such as not requiring X-ray fluoroscopy and post-procedure catheter management. Several recent studies have explored novel approaches in the management of AC. One study investigated the use of cholangiography via PTGBD as a preoperative technique for accurate delineation of biliary anatomy [29]. This approach aims to enhance surgical planning and optimize outcomes for patients undergoing subsequent interventions. Another study focused on the efficacy of gallstone release following PTGBD in cases of impacted gallstones associated with AC [30]. The findings of these studies contribute to the expanding knowledge and potential therapeutic options for the management of AC. The findings of these studies may help contribute to the development of new treatment guidelines in the management of AC. The incorporation of these outcomes into clinical practice guidelines can enhance decision-making and improve patient care in the field of AC management. Further research and validation are necessary to establish the robustness and applicability of these findings in guiding clinical recommendations.
This study has several limitations that should be considered. First, it was a retrospective analysis of a specific cohort in the Republic of Korea, limiting the generalizability of the results to other countries. Therefore, future prospective large-scale studies are warranted to validate our findings. Second, while we used PSM to mitigate potential confounders, it is important to acknowledge the possibility of unaccounted variables (such as preoperative WBC, SIRS, pneumonia, and cardiac disease) influencing the outcomes. Third, in this study, the incidence of biliary complications was found to be low, and the total number of cases was relatively small. Due to the limited number of cases and a multitude of variables in the regression analysis, there are certain limitations in conducting the regression analysis. It is acknowledged that a larger sample size is necessary to attain more robust and reliable results from regression analysis. A small sample size can render the estimates unstable and less reliable, thereby necessitating a larger sample to strengthen the statistical findings. Next, this study did not directly analyze the difference between PTGBD and upfront surgery according to the patient’s overall condition, such as ASA PS class and ECOG; therefore, it is not possible to show accurate results regarding this morbidity with surgical outcomes. Finally, the wide range of time intervals between PTGBD and LC in the PTGBD group may introduce variability that could affect the accuracy of the results. Despite these limitations, we believe that this study offers valuable clinical insights by minimizing selection bias inherent in retrospective analyses with PSM.
In conclusion, our findings suggest that early LC is generally a feasible approach for most cases of moderate-to-severe AC. In patients with underlying diseases and a risk of complications associated with general anesthesia, consideration should be given to PTGBD as an alternative strategy. To thoroughly examine the optimal interval between PTGBD and LC, a large-scale prospective study is warranted. The continuous evaluation of recent treatment strategies is crucial and is expected to contribute to improved patient outcomes and prognosis.
 XML Download
XML Download