

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
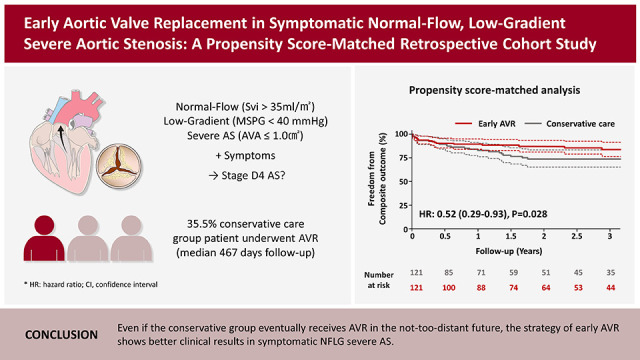
Severe aortic stenosis (AS) is associated with a high mortality rate if left untreated after symptoms begin. Aortic valve replacement (AVR) is strongly recommended for patients with symptomatic severe AS.1)2) Severe AS is defined as an aortic valve area (AVA) <1.0 cm2 and a mean transaortic pressure gradient (PG) ≥40 mmHg (or peak transaortic jet velocity [Vmax] ≥4 m/s), which are derived from echocardiographic measurement. However, there is often discrepancy between echocardiographic criteria for grading of AS severity, and one-third of patients with severe AS receive discordant gradings.3)4) Current guidelines and expert consensus classify low-gradient AS into several categories according to left ventricular (LV) ejection fraction (EF) and stroke volume (SV) index. Among low-gradient AS patients, those with normal-flow, low-gradient (NFLG) severe AS are often recognized as moderate AS.1)2)5) Nevertheless, recent studies have shown that the number of symptomatic NFLG AS patients is increasing, and have a poor prognosis.6)7) Prolonged LV ejection time, increased systolic blood pressure, and/or reduced systemic arterial compliance may explain the onset of NFLG severe AS.8) NFLG severe AS is a real and frequent entity that should receive special attention. However, the current guidelines offer no specific recommendations for this population because previous studies have reported conflicting results on the efficacy of AVR in patients with NFLG severe AS; consequently, AVR has been underutilized in such individuals.7)9)10)11)12) We aimed to assess the impact of early AVR on clinical outcomes compared to conservative care in symptomatic NFLG severe AS patients. We also aimed to determine which subgroup receives the greatest benefit from early AVR.
METHODS
Ethical statement
The study was approved by the Institutional Review Board of Severance Hospital (4-2022-1242), and the need for informed consent was waived due to the retrospective study design.
Study population
This was a retrospective cohort study performed at a single tertiary hospital in South Korea. Between January 2010 and December 2020, a total of 795 consecutive NFLG severe AS cases (AVA <1.0 cm2, mean transaortic PG <40 mmHg, peak transaortic velocity <4 m/s, and SV index ≥35 mL/m2) was reviewed. Patients without cardinal symptoms (dyspnea, angina, or syncope) (n=155) and those with a history of cardiac surgery (n=311), significant disease of other valve issues (e.g., mitral stenosis with mean PG >5.0 mmHg or any significant regurgitation grade ≥3) (n=32), active malignancies (n=13), or active infective endocarditis (n=3) were excluded. After exclusion, 281 symptomatic NFLG severe AS patients were analyzed. The study population was classified into early AVR and conservative care groups; patients who underwent AVR within 3 months after index echocardiography were classified into the early AVR group. All patient cases were discussed by a multidisciplinary heart team, which decided whether to perform AVR and what type (surgical or transcatheter) of procedure to perform. The index date was defined as the day of index echocardiography. A total of 121 patients was included in the early AVR group, and 1:1 propensity score matching was performed. The matching variables were age, sex, body surface area, body mass index, history of hypertension, diabetes mellitus treated with insulin, chronic kidney disease (stage ≥3), dialysis status, peripheral artery disease, coronary artery disease, old cerebrovascular accident, atrial fibrillation, bicuspid aortic valve, chronic lung disease, chronic liver disease, presence of a pacemaker, and other components of the European System for Cardiac Operative Risk Evaluation (EuroSCORE II) like estimated pulmonary artery systolic pressure or New York Heart Association (NYHA) class.13) Data on baseline characteristics and comorbidities were obtained via medical records. Concomitant multimodal imaging was defined as cardiac computed tomography or transesophageal echocardiography performed within one month after index echocardiography. Several subgroup analyses were performed according to comorbidities and echocardiographic parameters.
Echocardiography
All echocardiographic studies were performed using commercially available equipment, and standard measurements and AS assessments were performed according to current guidelines.14)15) AVA was calculated using the continuity equation formula. The left ventricular outflow tract (LVOT) was assessed in the apical 5-chamber view, and its diameter was measured mid-systole at a point 0.5–1 cm below the aortic annulus on the parasternal long-axis view. The velocity-time integral of the LVOT (VTILVOT) was assessed by pulse-wave Doppler. Assuming a circular geometry of LVOT, SV was calculated using the following formula: LVOT diameter2×0.785×VTILVOT. The highest peak velocity across the aortic valve, the mean transaortic PG, and the VTI of the aortic valve were measured in multiple acoustic windows (apical, suprasternal, or right parasternal) using continuous-wave Doppler. Concomitant valvular regurgitation was classified according to current guidelines.16) All measurements represent an average of 3 cardiac cycles for patients with sinus rhythm or an average of 5 cardiac cycles for patients with atrial fibrillation.
Clinical outcomes
The primary outcome was the composite of all-cause death and unplanned hospitalization for heart failure (HF). The secondary outcomes were individual components of the primary outcome. HF hospitalization was defined as an unplanned urgent admission for management of HF (including intravenous diuretics) lasting ≥24 hours. Patients were censored if primary outcome events occurred. Patients receiving conservative care underwent AVR during follow-up according to the heart team’s discussion and patient preference. Patients who were admitted for planned AVR with symptom and severity progression to classic severe AS were not considered as HF hospitalizations. We also performed 2 additional analyses, comparing (1) the early AVR group with the conservative care group with delayed AVR and (2) the early AVR group with the conservative care group without delayed AVR.
Statistical analyses
Continuous variables are expressed as mean±standard deviation or median (interquartile range) and were compared using Student’s t-test or the Wilcoxon rank-sum test according to distribution. Categorical variables were expressed as number with (percentage) and compared using the χ2 test. The 1:1 propensity score was estimated using logistic regression with all variables in the model and then matched using the greedy nearest-neighbor matching method, in which patients were matched on the logit of the propensity score using a caliper width of 0.2 of the standard deviation. Standardized mean differences were estimated to assess pre- and post-match balance, and <0.2 was considered small.17) Survival rates from clinical outcomes between 2 groups were estimated using the Kaplan-Meier method and compared with the log-rank test. The incidence rates of clinical outcomes were presented as %/year, and 95% confidence intervals (CIs) were calculated. Univariable and multivariable Cox proportional hazards models were used to calculate the hazard ratios (HRs) and 95% CIs for clinical outcomes. In the multivariable model, we included variables that achieved p<0.20 in univariate analyses. Several subgroup analyses were performed according to age, sex, comorbidities, and echocardiographic parameters and represented using forest plots. A density plot was used to show the balance for matched variables in the populations from before and after propensity score–matching. To assess the potential effect of unmeasured confounders, we calculated the E-value, which is defined as the minimum strength of association on the risk ratio scale. A large E-value implies that considerable unmeasured confounding would be needed to explain away an effect estimate, while a small E-value indicates that little unmeasured confounding would be necessary to explain an effect estimate.18)19) All tests were 2-sided, and p<0.05 was considered statistically significant. All statistical analyses were performed using R version 4.1.0 (The R Foundation for Statistical Computing, Vienna, Austria; www.R-project.org).
RESULTS
Baseline characteristics
Table 1 shows the baseline characteristics of the early AVR group and conservative care group before and after propensity score matching. All covariates were appropriately matched (Supplementary Figure 1). The mean age of the matched cohort was 75.8±9.9 years, and 135 participants (55.8%) were female. Dyspnea was the major cardinal symptom, and most patients had NYHA class II dyspnea. The median EuroSCORE was 1.57 (1.03–2.13) in the early AVR group and 1.75 (1.25–2.34) in the conservative care group. In the early AVR group, the interval between index echocardiography and AVR was 8 (5–25) days; 67 patients (55.4%) underwent surgical AVR (SAVR) and 54 (44.6%) underwent transcatheter AVR (TAVR). Concomitant coronary revascularization was performed in 11 patients (9.1%) in the early AVR group.
Table 1
Baseline characteristics of overall and propensity-score matched population
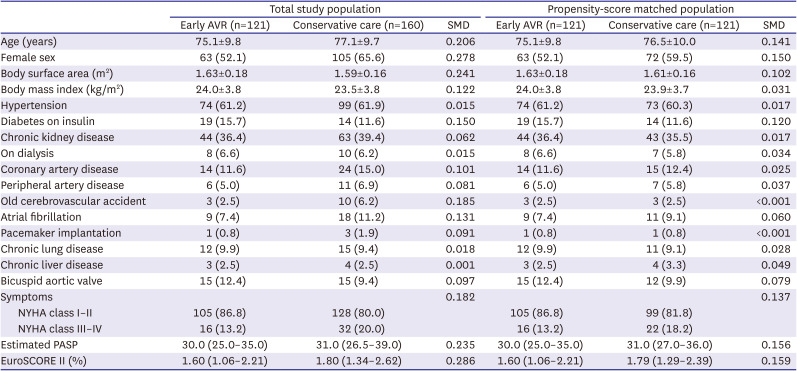
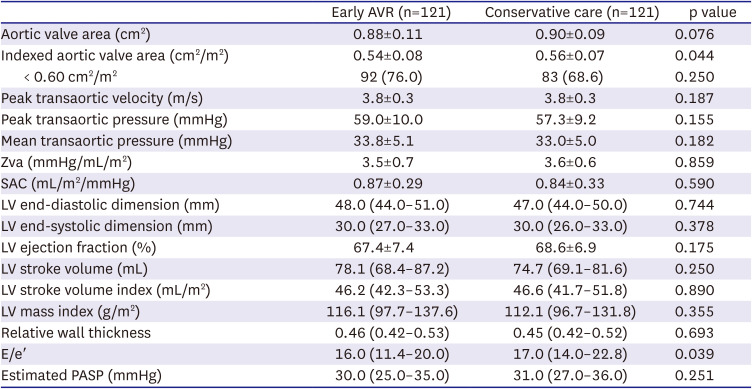
Table 2 shows the echocardiographic characteristics of the 2 groups. Most echocardiographic parameters including AVA, transaortic velocity, transaortic PG, SV index, and LVEF, were similar between the groups. However, indexed AVA (0.54±0.08 vs. 0.56±0.07 cm2/m2, p=0.044) and E/e′ (16.0 [11.4–20.0] vs. 17.0 [14.0–22.8], p=0.039) were lower in the early AVR group than in the conservative care group. Patients in the early AVR group underwent multimodal imaging for in-depth structural or functional evaluation prior to intervention more frequently than patients in the conservative care group (75.2% vs. 21.5%, p<0.001).
Table 2
Echocardiographic parameters
Clinical outcomes
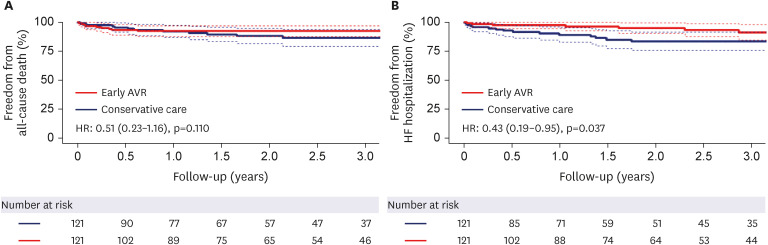
The median follow-up duration was 21.3 (6.5–47.5) months. Table 3 shows the comparisons of clinical events in the early AVR group and the conservative care group. A total of 48 primary outcomes (18 in the early AVR group vs. 30 in the conservative care group) occurred during follow-up. Three patients (2.5%) in the early AVR group died within 30 days after surgery. The numbers of primary outcome events within 3 months after index echocardiography were similar in the 2 groups (7 in the early AVR group vs. 7 in the conservative care group). The early AVR group had a significantly lower incidence of primary outcomes than the conservative care group (5.0 vs. 10.1%/year; HR, 0.52; 95% CI, 0.29–0.93; p=0.028; Figure 1). The E-value for the primary outcome was 2.52. Considering individual outcomes, the early AVR group had a lower incidence of all-cause death than the conservative-care group, but this result did not reach statistical significance (2.5 vs. 5.0%/year; HR, 0.51; 95% CI, 0.23–1.16; p=0.110; Figure 2A). Patients in the early AVR group had a significantly lower incidence of HF hospitalizations than conservative care group patients (2.5 vs. 6.7%/year; HR, 0.43; 95% CI, 0.19–0.95; p=0.037; Figure 2B).
Table 3
Clinical outcomes
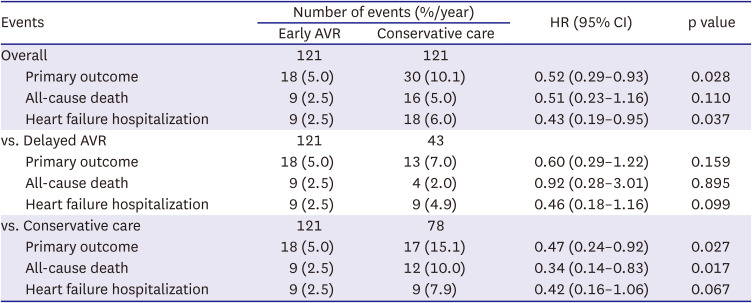
Figure 1
Survival from composite outcomes of all-cause death or heart failure hospitalization.
AVR = aortic valve replacement; HR = hazard ratio.
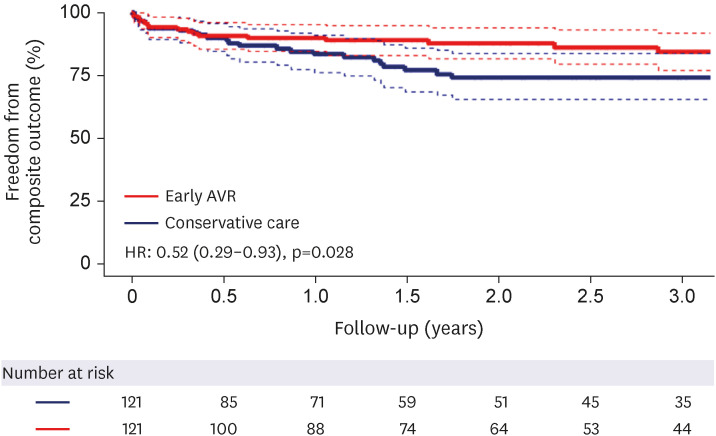
Figure 2
Survival from individual outcomes of all-cause death (A) and heart failure hospitalization (B).
AVR = aortic valve replacement; HR = hazard ratio.
During follow-up, 43 patients (35.5%) in the conservative care group ultimately underwent AVR, and the time interval between indexed echocardiography and AVR was 467 (217–859) days. Progression to high-gradient severe AS (73.3%) was the most common reason for AVR in the conservative care group. Other patients (26.7%) underwent delayed AVR for symptom progression without hemodynamic progression (Supplementary Table 1).
When comparing the early AVR subgroup and delayed AVR subgroup, the former group had a tendency for fewer HF hospitalization events (2.5 vs. 4.9%/year; HR, 0.46; 95% CI, 0.18–1.16; p=0.099). Also, when comparing the early AVR subgroup and conservative care subgroup (excluding patients who underwent delayed AVR), the former group had a significantly lower incidence of the primary outcome (5.0 vs. 15.1%/year; HR, 0.47; 95% CI, 0.24–0.92; p=0.027) and all-cause death (2.5 vs. 7.9%/year; HR, 0.34; 95% CI, 0.14–0.83; p=0.017).
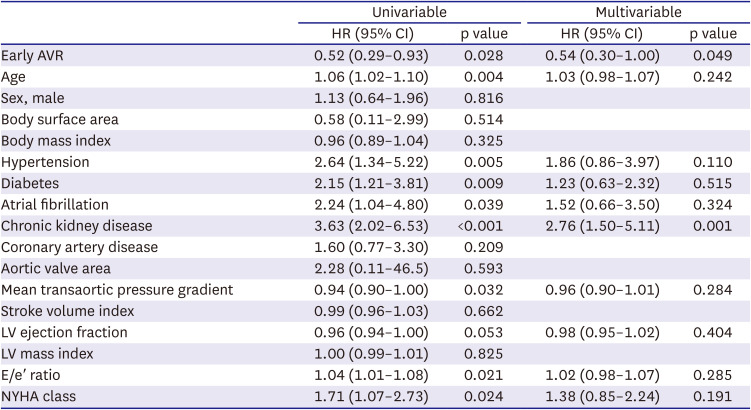
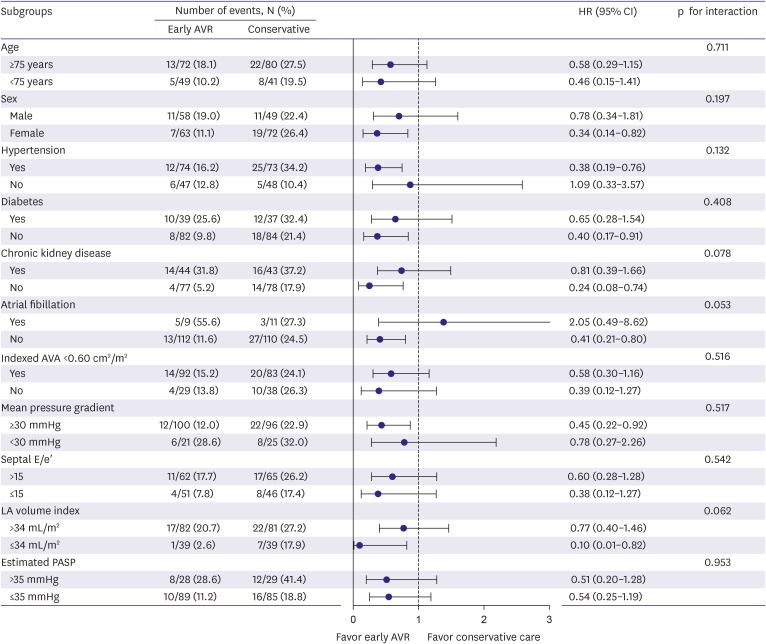
According to multivariable Cox regression modeling, early AVR was independently associated with a lower risk of the primary outcome (adjusted HR, 0.54; 95% CI, 0.30–1.00; p=0.049), while chronic kidney disease was independently associated with a higher risk of the primary outcome (adjusted HR, 2.76; 95% CI, 1.50–5.11; p=0.001; Table 4). Subgroup analysis offered similar results to the main findings (No p value for any interaction was significant). However, the atrial fibrillation subgroup showed a trend toward a greater risk of early AVR (Figure 3). In the multivariable analysis, there was no significant difference between early TAVR and SAVR (adjusted HR, 2.66; 95% CI, 0.63–11.1; p=0.181).
Table 4
Predictors of primary outcomes in Cox regression analysis
DISCUSSION
The main findings of this study are as follows: (1) early AVR was associated with a significantly lower rate of the composite outcome of all-cause death and HF hospitalization; (2) about 33% of patients in the conservative care group eventually underwent AVR during a median 21.3-month follow-up; (3) patients in the conservative care group patients who did not undergo delayed AVR had significantly higher incidence rates of the primary outcome and all-cause death. Even the patients receiving delayed AVR in the conservative group had a higher tendency for HF hospitalization compared to patients in the early AVR group; and (4) subgroup analysis consistently showed the benefits of early AVR in patients with symptomatic NFLG severe AS. These findings provide evidence supporting the potential benefit of early AVR in patients with symptomatic NFLG severe AS.
Unlike the situation with classical high-gradient severe AS, evidence of surgical and TAVR in low-gradient severe AS is limited.1)2) According to current guidelines, NFLG severe AS patients are usually recognized to have only moderate AS, and AVR is not indicated.2) However, recent studies have reported that NFLG severe AS patients have specific characteristics, such as female predominance, small body size, and reduced arterial compliance combined with high blood pressure, which are related to a poor prognosis.7)20)21) Compared to previous studies, our study enrolled patients with similar characteristics, although the mortality rate was low.9)10)11) This might be related to the presence of fewer comorbidities and few ethnic differences in our study population.22)23)
Several previous studies have reported conflicting results on the benefits of early AVR (Supplementary Table 2). Saeed et al.10) documented mortality benefits of AVR in small numbers of a matched population (80 matched pairs) and a higher proportion of NYHA III–IV patients. A study by Zusman et al.11) enrolled a much older population (median age, 83 years) and matched only conservatively treated patients and TAVR patients, yielding a small sample of 94 matched pairs. The meta-analysis by Dayan et al.24) also reported the benefits of AVR in NFLG severe AS. Our study documented a benefit of AVR in the composite outcome but not in all-cause death. These differences have several possible explanations. First, our study population might have received more meticulous follow-up care. In the present study, 43 of 121 patients (35.5%) in the conservative care group underwent delayed AVR, whereas only 2.7% of conservative group patients underwent AVR in the study by Zusman et al.11) Second, as mentioned above, the mortality rate of our study was less than those of previous studies. Thus, our study sample might be too small to show statistical significance in reducing mortality. Additionally, the mortality benefit from AVR might be smaller for NFLG severe AS patients than for those with conventional high-gradient AS because NFLG severe AS might actually be an “intermediate” stage of the condition between moderate and severe AS.25)
Kang et al.9) showed similar mortality rates from AVR to watchful waiting in similar study subjects as ours, but they enrolled a markedly small population of TAVR patients (n = 5) and allowed differences in echocardiographic parameters between the groups. Eleid et al.26) showed that NFLG severe AS patients had favorable survival with standard medical treatment with no benefit or damage from AVR, but the NFLG group had significantly fewer comorbidities.
In addition, neither of these previous studies examined HF hospitalization events. Our study showed significant benefits of early AVR in HF hospitalization. Notably, the conservative care group had a higher rate of HF hospitalization than the early AVR group despite delayed AVR being performed during follow-up. In this study, the conservative group patients without delayed AVR showed higher mortality rates. Although timely performed AVR appeared to reduce adverse outcomes, there was a tendency for more HF hospitalization events. These findings suggest that early AVR performed before advanced cardiac remodeling and comorbidity progression might be helpful in NFLG severe AS patients. Considering composite outcomes of death or HF hospitalization as major primary outcomes in recent cardiology trials, our study has strength in showing the benefit of early AVR in composite outcomes with a well-matched, larger study population.27)28)
We expected to find specific subgroups in which the effect of early AVR was magnified, but we did not. Our subgroup analysis showed consistent benefits of early AVR, and these findings suggest that early AVR might be performed for most symptomatic NFLG severe AS patients. Only the atrial fibrillation subgroup showed a trend that did not favor early AVR, but we included very few patients in this subgroup, so this result should not be over-interpreted. In addition, the beat-to-beat variability and low-flow status of atrial fibrillation might induce bias in AS assessment.29) Finally, we were not able to examine the roles of multimodal imaging because of the small number of subjects who underwent multimodal imaging. Future prospective studies with combined multimodal imaging and larger populations are needed to confirm our findings.
This study has several limitations. First, this was a retrospective study from a single tertiary center in South Korea; thus, it carries inherent limitations and ethnical biases. Second, the selection bias needs to be acknowledged. It is likely that early AVR group members had more advanced aortic valve disease. Third, the severity of AS was only assessed by Doppler echocardiography; multimodal imaging was not performed in many patients, especially in the conservative care group. However, the method of choice for assessing AS severity is Doppler echocardiography, and the role of other imaging modalities in this situation is inconclusive. Fourth, although we considered and matched all available clinical variables from previous studies, there might be unmeasured confounders that affected clinical events. Fifth, although AVA and E/e' were different between the 2 groups, we could not include echocardiographic parameters in the calculation of the propensity score due to the small number of patients. Instead, we performed a multivariable analysis including such echocardiographic variables and the results were consistent. These limitations should be taken into account when interpreting the results. Instead, we performed univariable and multivariable analysis including such echocardiographic variables, and the results showed that early AVR also showed meaningful results. However, despite these limitations, we believe that the results observed in this study are meaningful in addressing unmet clinical needs.
In patients with symptomatic NFLG severe AS, early AVR may improve the composite outcome of all-cause death and HF hospitalization compared to conservative care. Future large-scale prospective studies are needed to confirm these findings.
 XML Download
XML Download