

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Cancer is the leading cause of death worldwide, and the global cancer burden is continuously increasing worldwide [123]. The most common treatment for cancer has long been surgery with a curative intent [4]. In 2015, there were 15.2 million new cases of cancer worldwide, over 80% of which required surgery [5]. Thus, the delivery of safe, affordable, and timely cancer surgery is an important health issue for global and national cancer control.
Lifestyle factors, including smoking, alcohol consumption, and physical activity, are known modifiable risk factors associated with age to first chronic disease [6]. Previous studies have reported that lifestyle factors are associated with the incidence of several diseases, including new-onset atrial fibrillation, diabetes mellitus, and kidney stone disease [789]. Moreover, lifestyle is a modifiable risk factor for increased all-cause mortality in the adult population [10]. Remarkably, half of all cancer risks could be influenced by lifestyle factors, including alcohol consumption, smoking, and physical activity [11]. Although lifestyle is an important and modifiable risk factor for health-related outcomes, no study has focused on the impact of preoperative lifestyle habits on mortality in patients who underwent cancer surgery.
Therefore, this study aimed to examine whether preoperative lifestyle factors are associated with mortality after cancer surgery.
METHODS
Study design and ethical statements
This study involved human participants, and all procedures were conducted in accordance with the guidelines provided by the Institutional Review Board (IRB) of the Seoul National University Bundang Hospital (No. X-2105-686-904). The National Health Insurance Service (NHIS) provided data after approval of the study protocol (NHIS-2022-1-336). The requirement for informed consent was waived by the IRB because data analyses were performed retrospectively using anonymous data derived from the South Korean NHIS database.
Data source
The NHIS database was used for data extraction. As a single public health insurance database in South Korea, NHIS contains and manages data on disease diagnoses and prescriptions for procedures and drugs. Disease diagnoses were registered using the International Classification of Diseases, External 10th Revision (ICD-10 codes). Additionally, the NHIS database contains demographic and socioeconomic status-related information for all patients in South Korea.
Study population
We initially included all adult patients (aged ≥18 years) who were admitted to the hospital and underwent major cancer surgery with curative intent from January 1, 2016, to December 31, 2018. Major cancers included lung, gastric, colorectal, esophageal, small bowel, liver, pancreatic, bile duct, and gallbladder cancers. In South Korea, patients with cancer should be registered in the NHIS database to receive financial coverage for treatment expenses. Particularly, the government supports most (approximately 95%) of the costs of treatment for patients with cancer. Among the patients who underwent major cancer surgery, we included those who had undergone standardized health examinations in the year prior to cancer surgery. In South Korea, NHIS subscribers aged ≥40 years are recommended to undergo standardized health examinations every 2 years [12].
Lifestyle factors in cancer surgery
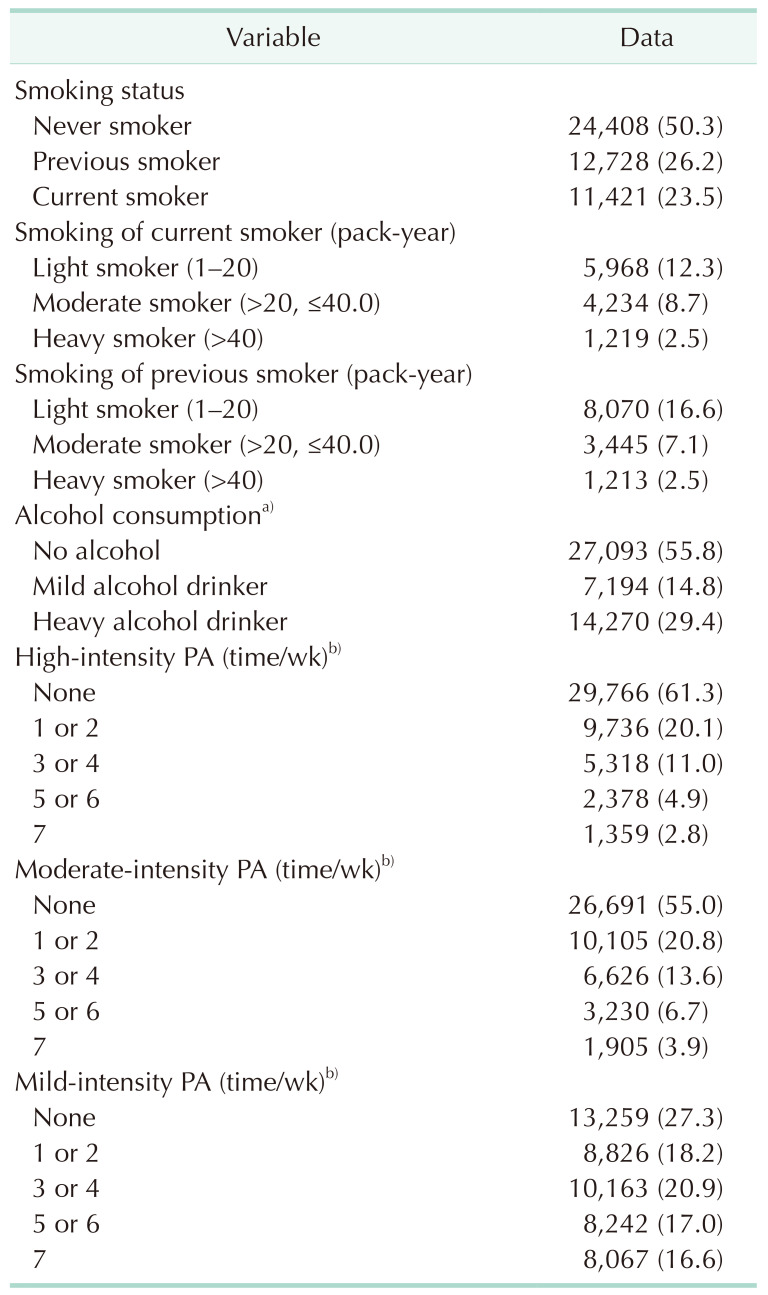
Three lifestyle factors were evaluated before intensive care unit admission: smoking status, alcohol consumption, and physical activity. Information regarding lifestyle factors was obtained through voluntary responses to questionnaires on standardized health examinations. Smoking status was classified into 3 groups: (1) never smokers, (2) previous smokers, and (3) current smokers. In addition, the smoking pack-years of current and previous smokers were calculated to reflect the cumulative smoking amounts of both current and previous smokers. Based on a previous study [13], 0.1–20.0, 20.1–40.0, and >40.0 pack-years were used to classify current and previous smokers as light, moderate, and heavy smokers. Based on previous reports [1415], alcohol consumption was divided into 3 groups: nondrinkers, mild drinkers, and heavy drinkers. The mild drinker group was defined as people with an alcohol consumption of ≤210 g/week in male and ≤140 g/week in female, whereas the heavy drinker group was defined as alcohol consumption of >210 g/week in male and >140 g/week in female. Physical activity was divided into 3 types according to its intensity: intensive, moderate, and mild. Intensive physical activity was defined as strenuous exercise for >20 minutes, and moderate physical activity was defined as moderate exercise without breathlessness for >30 minutes. Mild physical activity was defined as walking for >30 minutes. Each exercise frequency was divided into 4 groups: no exercise, 1 or 2 times per week, 3 or 4 times per week, 5 or 6 times per week, and 7 times per week.
Study endpoint
This study had 2 primary endpoints: 90-day mortality and 1-year postoperative all-cause mortality. Mortality was defined as death within 90 days or one year after the date of major cancer surgery.
Covariates
The covariates were collected according to the criteria of our previous study [16]. Demographic information such as age, sex, and body mass index was collected. Socioeconomic status-related information, employment status, residence, and household income levels were collected. The NHIS contains the patients’ household income levels to determine the insurance premiums for the year, and approximately 67% of medical expenses are subsidized by the government [17]. However, individuals from low-income households are enrolled in the medical aid program, in which the government covers nearly all medical expenses to minimize the financial burden of medical costs. Patients were divided into 5 groups based on quartile ratios: Q1–Q4 and medical aid program groups. Residences were classified as urban (Seoul and other metropolitan cities) or rural (all other areas). Surgical cases of video-assisted laparoscopic surgery and laparoscopy were collected as covariates. The Charlson comorbidity index was calculated using the ICD-10 codes to determine the comorbidity status of patients (Supplementary Table 1). All individuals with disabilities must be registered in the NHIS database to receive benefits from South Korea’s social welfare system. In the database, patients were divided into 6 groups according to the severity of disability. We divided patients into 2 severity groups; patients with grades 1–3 disabilities were assigned to the severe disability group, whereas those with grades 4–6 were assigned to the mild-to-moderate disability group.
Statistical analysis
The clinicopathological characteristics of patients are presented as numbers with percentages for categorical variables and mean values with standard deviation (SD) for continuous variables. We constructed a multivariable logistic regression model for 90-day mortality after cancer surgery, and all covariates were included in the model for adjustment. The Hosmer-Lemeshow test was used to check whether the model of fit in the model was appropriate, and the results were presented as odds ratios (OR) with 95% confidence intervals (CI). Moreover, we constructed a multivariable Cox regression model for 1-year all-cause mortality after cancer surgery as a time-to-event analysis. All covariates were included in the model for adjustment, and the results are presented as hazard ratios (HR) with 95% CIs. Log-log plots were used to confirm that the central assumption of the Cox proportional hazards model was satisfied. The smoking pack-years of smokers were included in another multivariable model to avoid multicollinearity with smoking status. Additionally, we performed subgroup analyses according to the type of cancer surgery because smoking and alcohol are risk factors for different types of cancer [18]. The issue regarding multicollinearity between variables in the multivariable model was not observed with a criterion of variance inflation factors <2.0. All statistical analyses were performed using R software (ver. 4.0.3, R Foundation for Statistical Computing), and P-values of <0.05 were considered statistically significant.
RESULTS
Study population
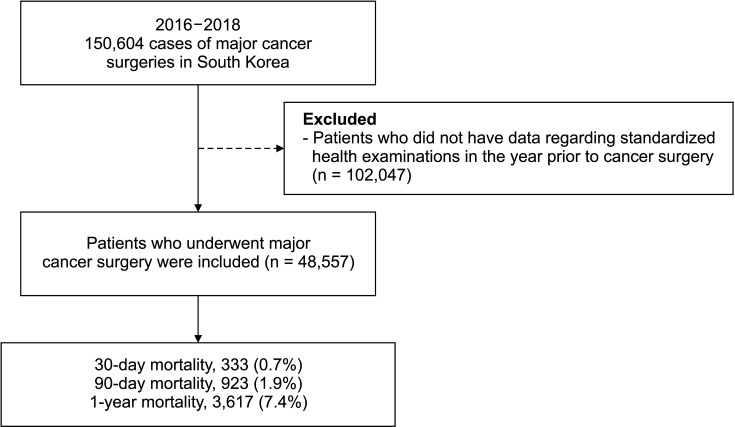
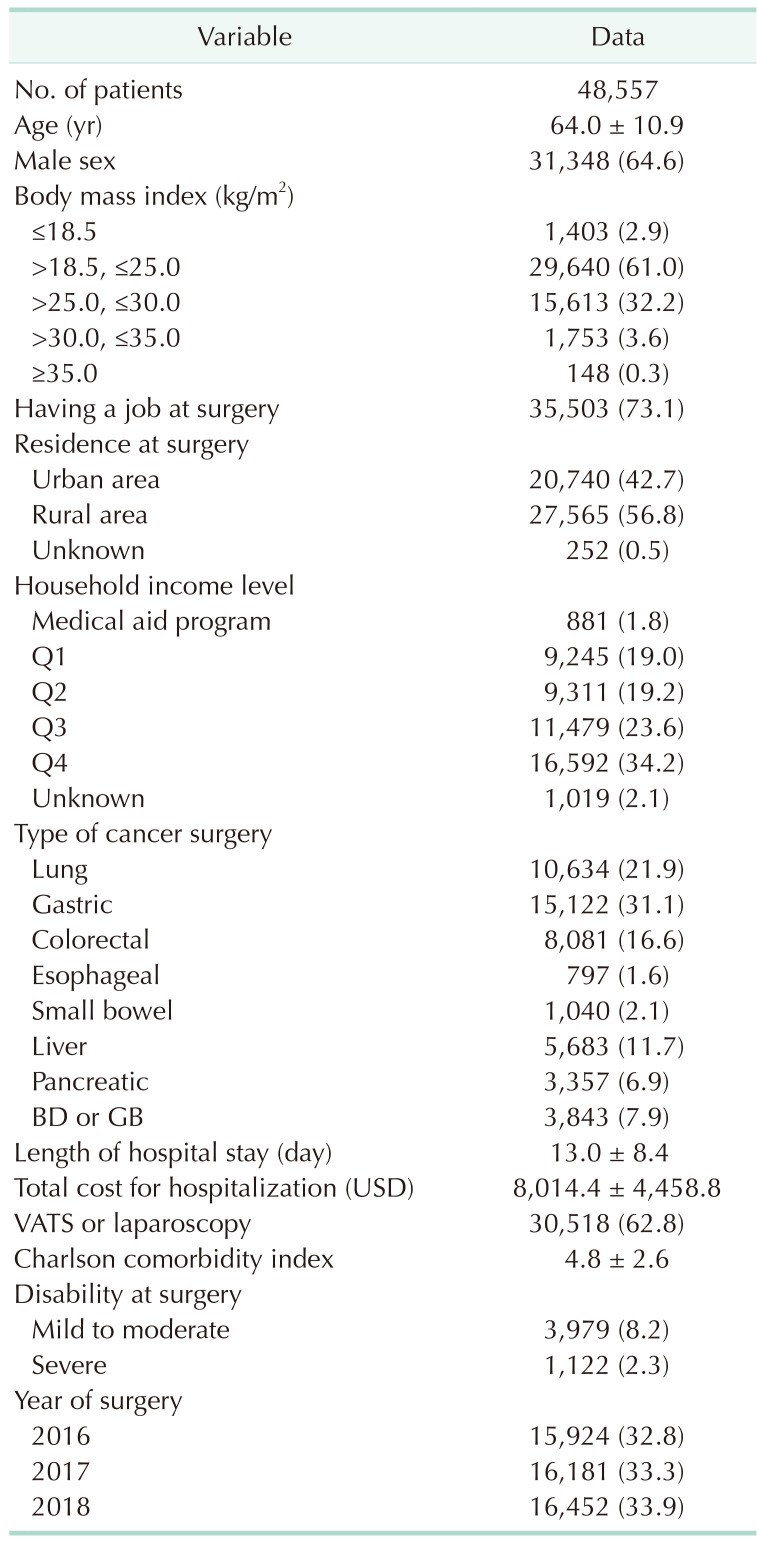
From January 1, 2016, to December 31, 2018, there were 150,604 cases of major cancer surgeries in South Korea. After excluding 102,047 patients who did not have data regarding standardized health examinations in the year prior to cancer surgery, 48,557 patients who underwent major cancer surgery were included in the final analysis. Among them, 333 (0.7%), 923 (1.9%), and 3,617 (7.4%) died within 30 days, 90 days, and 1 year after cancer surgery, respectively, as shown in Fig. 1. Table 1 shows the clinicopathological characteristics of patients. The mean age was 64.0 years (SD, 10.9 years), and 31,348 patients (64.6%) were male. The mean length of hospital stay was 13.0 (SD, 8.4) days, and the mean total cost of hospitalization was 8,014.4 US dollars (SD, 4,458.8 US dollars). The results of the standardized health examinations are presented in Table 2.
Survival analyses for 90-day mortality
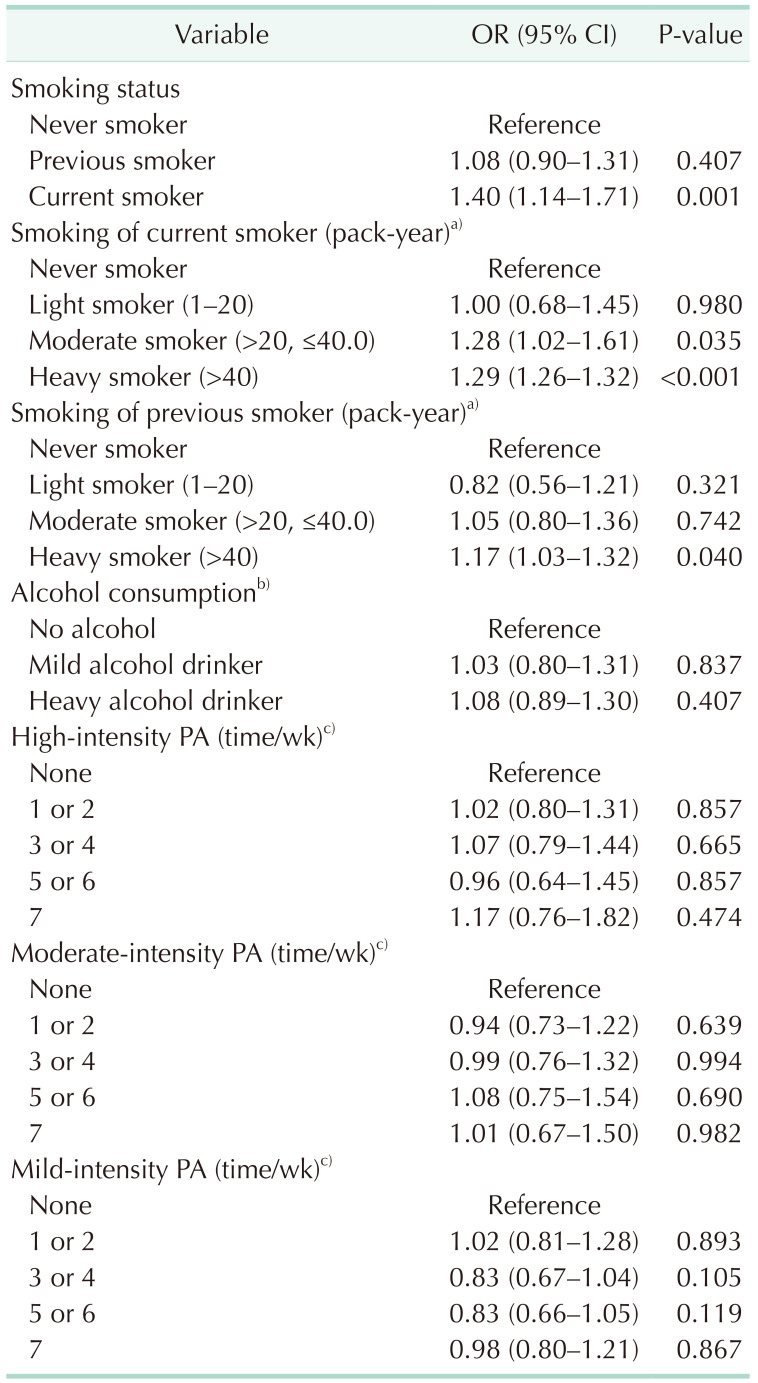
Table 3 shows the results of the multivariable model for 90-day mortality after cancer surgery. Compared to never smokers, current smokers showed 1.40-fold higher odds of 90-day mortality after cancer surgery (OR, 1.40; 95% CI–1.14, 1.71; P = 0.001). Compared to never smokers, the 20.1–40 pack-year (moderate smokers) and >40 pack-year (heavy smokers) groups of current smokers showed 1.28-fold (OR, 1.28; 95% CI, 1.02–1.61; P = 0.035) and 1.29-fold (OR, 1.29; 95% CI–1.26, 1.32; P < 0.001) higher odds of 90-day mortality after cancer surgery, respectively. Furthermore, compared to never smokers, the >40 pack-year (heavy smokers) group of previous smokers showed 1.28-fold (OR, 1.17; 95% CI–1.03, 1.32; P = 0.040) higher odds of 90-day mortality after cancer surgery. Additionally, alcohol consumption and physical activity were not associated with 90-day mortality after cancer surgery. The ORs with 95% CIs of other covariates for 90-day mortality are presented in Supplementary Table 2.
Survival analyses for 1-year mortality
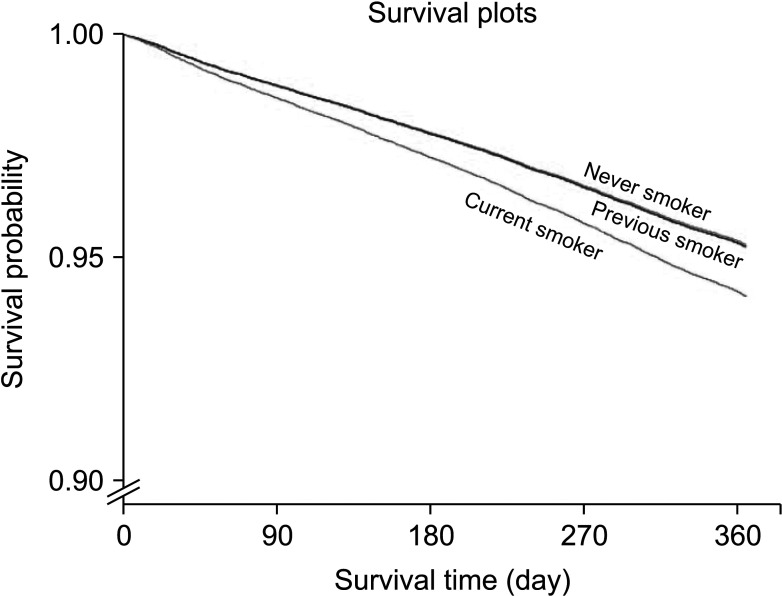
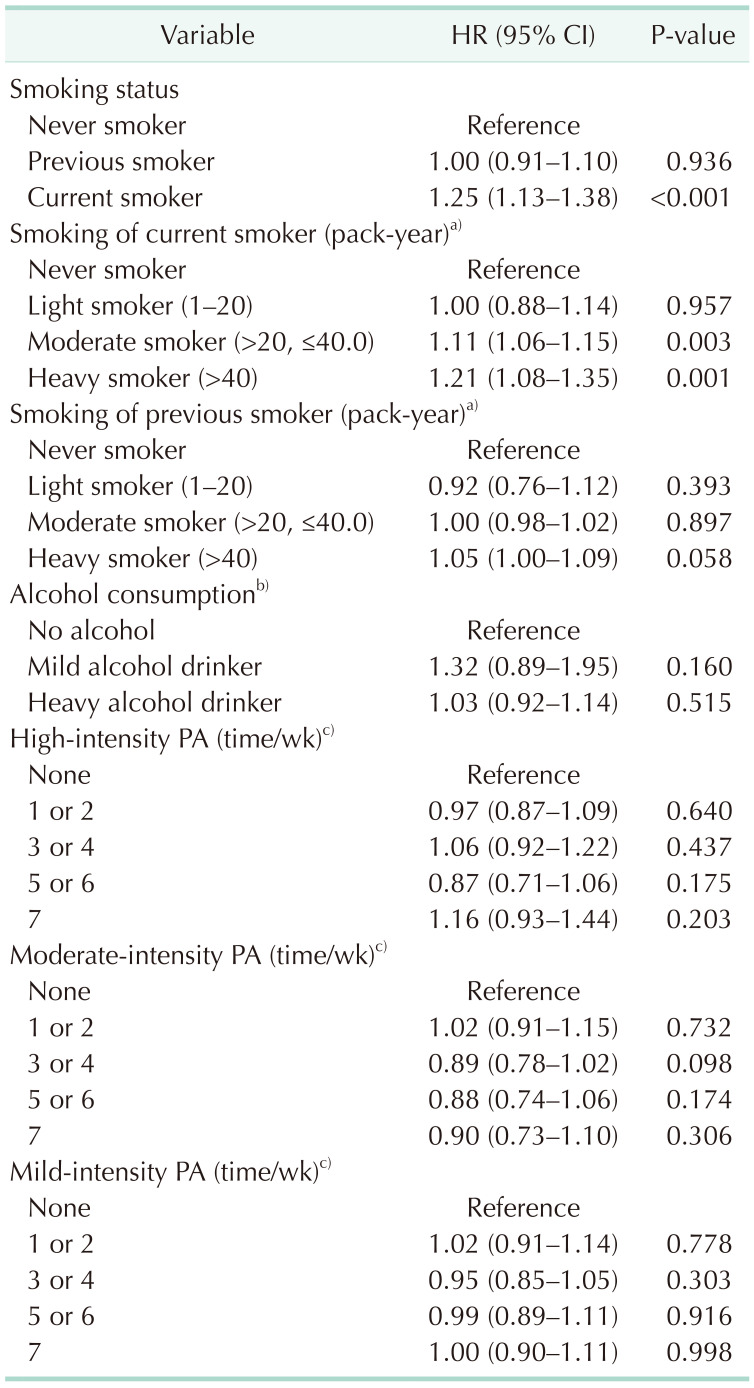
Table 4 shows the results of the multivariable Cox model for 1-year mortality after cancer surgery. Compared with never smokers, current smokers showed 1.25-fold higher odds of 1-year mortality after cancer surgery (HR, 1.25; 95% CI, 1.13–1.38; P < 0.001). Compared to never smokers, 20.1–40 pack-year (moderate smokers) and >40 pack-year (heavy smokers) groups of current smokers showed 1.11-fold (OR, 1.11; 95% CI, 1.06–1.15; P = 0.003) and 1.21-fold (OR, 1.21; 95% CI–1.08, 1.35; P = 0.001) higher odds of 1-year mortality after cancer surgery, respectively. Additionally, alcohol consumption and physical activity were not associated with 1-year mortality after cancer surgery. The HRs with 95% CIs of other covariates for 1-year mortality are shown in Supplementary Table 3. Survival plots derived from the multivariable Cox regression model according to smoking status are shown in Fig. 2.
Subgroup analyses
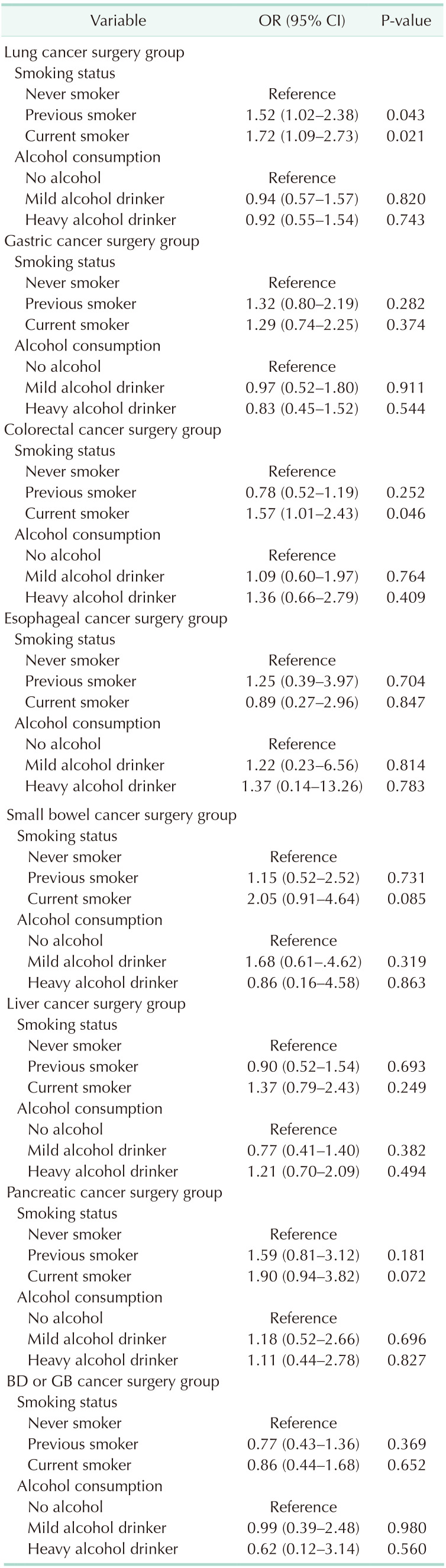
Table 5 shows the results of subgroup analyses for 90-day mortality. Compared to never smokers, current smokers showed higher 90-day mortality in the lung cancer surgery group (OR, 1.72; 95% CI, 1.09–2.73; P = 0.021) and colorectal cancer surgery group (OR, 1.57; 95% CI, 1.01–2.43; P = 0.046). Compared to never smokers, previous smokers showed higher 90-day mortality in the lung cancer surgery group (OR, 1.52; 95% CI–1.02, 2.38; P = 0.043). Alcohol consumption was not associated with 90-day mortality after each cancer surgery.
DISCUSSION
This population-based cohort study showed that, among preoperative lifestyle factors, current smoking status was associated with increased 90-day and 1-year mortality rates after major cancer surgery in South Korea. These associations were more evident in the moderate and heavy smoker groups on considering cumulative smoking amounts. However, preoperative alcohol consumption and physical activity levels were not associated with mortality after cancer surgery, suggesting that current smoking may be a risk factor for increased mortality after cancer surgery.
Previous studies reported that current smoking increased in-hospital mortality by approximately 20% and major postoperative complications by 40% [19]. A previous meta-analysis reported that current smoking during cancer treatment, including surgery, radiation, and systemic treatment, is associated with increased overall and cancer-specific mortality [20]. In addition to this literature, we reported that current smoking was associated with increased short- and long-term mortality after major cancer surgery.
Moreover, it was more evident in the moderate and heavy smoker groups on considering cumulative smoking amounts. A previous study reported that the duration and intensity of smoking should be considered together, using pack-years, in determining the risk of developing smoking-related diseases [21]. For example, it was reported that lifetime smoking exposure, measured in pack-years, was more useful than the current smoking status in evaluating mortality risk in patients with breast cancer [22]. Lifetime smoking exposure in pack-years was also used as a prognostic factor for long-term survival outcomes among patients with non-small cell lung cancer [23]. Our results also showed that the light smoker group of current smokers was not associated with 90-day mortality after cancer surgery, while the heavy smoker group of previous smokers was significantly associated on considering lifetime pack-years of smoking. Therefore, preoperative lifetime exposure to smoking might be a better indicator for predicting postoperative mortality in patients who underwent cancer surgery.
The results of alcohol consumption reported herein should be interpreted with caution. Neither mild nor heavy alcohol consumption was associated with mortality after major cancer surgery. However, the relationship between preoperative alcohol consumption and postoperative mortality has not yet been identified. A meta-analysis reported that preoperative alcohol consumption was associated with increased postoperative complications, including postoperative morbidity, infections, wound complications, pulmonary complications, prolonged hospital stay, and admission to the intensive care unit [24]. However, another prospective observational study reported that preoperative alcohol consumption is not associated with postoperative complications [25]. In patients with colorectal cancer, alcohol consumption was not associated with postoperative complications after colorectal cancer surgery [26]. While previous studies have focused on the relationship between preoperative alcohol consumption and the occurrence of postoperative complications [242526], we showed that preoperative alcohol consumption was associated with neither short- nor long-term mortality after major cancer surgery.
The nonsignificant relationship between preoperative physical activity and mortality after cancer surgery was also important in this study. As physical activity is known to decrease all-cause and cancer-specific mortality in the general adult population [27], it is an important and modifiable factor in patients with cancer. Moreover, physically active individuals have been reported to have a faster self-assessed physical recovery after colorectal cancer surgery [28], cholecystectomy [29], and lung cancer resection [30]. However, previous studies did not focus on mortality after cancer surgery [282930], whereas we focused on the relationship between preoperative physical activity and mortality after major cancer surgery. Therefore, further studies are needed to confirm the relationship between preoperative physical levels and surgical outcomes after cancer surgery.
This study had some limitations. First, each tumor stage among patients with major cancer was not evaluated, because the NHIS database did not have information on the tumor stage at cancer surgery, yet it could affect mortality after cancer surgery. Second, NHIS subscribers aged ≥40 years are recommended to undergo standardized health examinations every 2 years [12]; therefore, the study population included relatively older patients with a mean age of 64.0 years (SD, 10.9 years). If we critically included patients aged <40 years who underwent major cancer surgery, the results may have been different. Third, there might be some residual confounders in this study, which might have affected the results of multivariable modeling. Finally, the generalizability of the results of this study may be limited because the environment or health policies for patients with cancer differ by country.
In conclusion, we showed that, among preoperative lifestyle factors, current smoking status was associated with increased 90-day and 1-year mortality rates after major cancer surgery in South Korea, though preoperative alcohol consumption and physical activity levels were not.
 XML Download
XML Download