

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Inflammatory periapical lesions, a common sequela to pulp necrosis, represent a defensive host response to microbial invasion of the root canal system [12]. Histologically, inflammation is characterized by the presence of fibrous connective and granulation tissue, proliferating epithelium, and various types of inflammatory cells [3]. These cells primarily include lymphocytes, plasma cells, macrophages, and polymorphonuclear neutrophils (PMNs) [45]. The histological difference between acute and chronic inflammation lies in the presence of leukocytes within the tissue. In cases of acute inflammation, PMNs predominate, while macrophages and lymphocytes are more prevalent in chronic inflammation [67].
Pain management during and after root canal treatment is one of the most important aspects of endodontic practice [8]. Postoperative pain, which is extremely unpleasant for patients, has been reported to occur at frequencies between 3% and 58% [9]. Various methods have been used to manage postoperative pain, including cryotherapy. The term “cryotherapy” originates from the Greek word “cryos,” meaning cold. Both physiological and clinical evidence suggest that cold therapy, in its various forms, can reduce nerve conductivity time, hemorrhage, edema, and local inflammation. Cryotherapy has been demonstrated to be effective at alleviating musculoskeletal pain, muscle spasms, and connective tissue distension [101112].
Endodontic cryotherapy is conducted through intracanal irrigation following the cleaning, disinfection, and shaping of the root canal system. An in vitro study demonstrated that continuous irrigation with a cold saline solution at 2.5°C, coupled with negative pressure, could decrease the extraradicular temperature by over 10ºC [12]. In vivo studies have indicated that endodontic cryotherapy can alleviate postoperative symptoms in patients with symptomatic irreversible pulpitis, pulp necrosis, and symptomatic apical periodontitis [1012131415].
Lipopolysaccharide (LPS) is a component found in the outer membrane of Gram-negative bacteria. Its primary virulence factor is a potent endotoxin that triggers a sustained inflammatory response [16]. When LPS is present in connective tissue, even in low doses, it acts as a chemoattractant for neutrophils and prompts the release of pro-inflammatory cytokines. These cytokines activate the neuroimmune and neuroendocrine systems, leading to disease [17]. To counteract this, anti-inflammatory mediators such as interleukin 10 are produced, serving as compensatory mechanisms to mitigate excessive inflammation [161819]. In the past, endodontic cryotherapy has typically been administered for periods of 4 to 5 minutes, a recommendation drawn from the existing medical literature. However, limited information exists regarding the standardization of key factors such as the duration of therapy, method of administration, type of cold agent used, cellular mechanisms, and specific cells involved in the process. The present study was conducted to shed light on how the duration of cryotherapy impacts the suppression of acute inflammatory response in an animal model.
This study employed this animal model to assess the effectiveness of cryotherapy, applied for durations of 1 and 5 minutes, in reducing acute inflammation caused by catheter insertion of LPS. The null hypothesis proposed no difference in the effectiveness of cryotherapy, whether applied for 1 or 5 minutes. In contrast, the alternative hypothesis suggested that a 5-minute application of cryotherapy would be more effective than a 1-minute application.
Go to : 
MATERIALS AND METHODS
The study received Institutional Review Board (IRB) University of Baja California (UABC), approval under the IRB number 305-2545.
For this study, 6 Wistar rats, aged between 4 to 6 months and weighing between 200 to 280 g, were utilized. The rats were anesthetized through an intraperitoneal injection of xylazine (10 mg/kg) (Xilacina, PiSA BioPharm, Albany, NY, USA) and ketamine (25 mg/kg) (Ketamina, Cheminova Remedies Pvt. Ltd., Hyderabad, India). Prior to catheter insertion, the area was disinfected using an iodine solution. An acute inflammatory response was induced via subcutaneous injection of 0.5 mL/kg body weight of iron-containing Escherichia coli LPS (Sigma-Aldrich, St. Louis, MO, USA) into the rat dorsum. The injection was performed at the center of the animal along the midline (dorsal and ventral).
Pilot studies conducted on a separate group of rats revealed acute inflammation of the connective tissue at 45 minutes post-injection. For the present study, 5 specific sites were selected on each rat for examination: the rostral-dorsal, mid-dorsal, caudal-dorsal, rostral-ventral, and caudal-ventral areas (Figure 1). The rats were then divided into 3 control groups and 2 experimental groups.
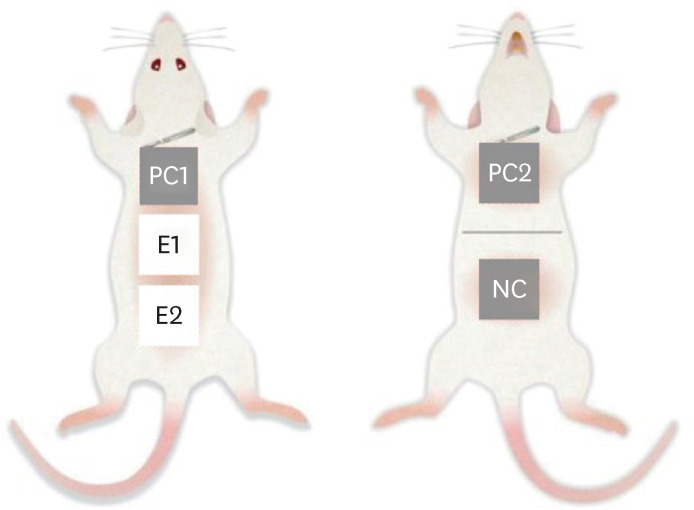
1. Negative control group (NC): This consisted of healthy connective tissue from the caudal-ventral area that underwent no treatment.
2. Positive control group 1 (PC1): The rostral-dorsal area received an injection of LPS, but no subsequent treatment was applied.
3. Positive control group 2 (PC2): The rostral-ventral area received an injection of LPS and a catheter was inserted, but no subsequent treatment was applied.
4. Experimental group 1 (E1): Following LPS injection and catheter insertion to the mid-dorsal area, cryotherapy was applied for 1 minute.
5. Experimental group 2 (E2): Following LPS injection and catheter insertion to the caudal-dorsal area, cryotherapy was applied for 5 minutes.
The following outlines the protocol for the E1 and E2. A catheter (14-G, 48 mm long, BD Insyte, Becton Dickinson, Franklin Lakes, NJ, USA) was inserted laterally above the subcutaneous tissue. The catheter was then connected to a venoclysis device and implanted 45 minutes after injection of the LPS suspension. The injection site was either the mid-dorsal or caudal area of the rat, determined after meticulous dissection. Subsequently, a continuous flow of saline solution, maintained at 2.5°C, was administered for either 1 or 5 minutes.
Sample collection and processing
Immediately after the application of cryotherapy, the animals were sacrificed using a 1-mL intraperitoneal injection of pentobarbital. Tissue samples, measuring 3 × 3 cm, were then preserved in 10% formalin (Hycel, Houston, TX, USA).
Histopathological analysis
The processed samples were stained with hematoxylin and eosin for examination under light microscopy. The histological analysis involved identifying neutrophils and assessing the degree of inflammation. The cellular analysis entailed identifying and counting PMNs, as well as determining the presence or absence of hemorrhage.
Statistical analysis
The degree of acute inflammation, the presence of hemorrhage, and the presence of PMNs were categorized using an ordinal scale (absent, mild, moderate, or intense). This scale was based on the degree of inflammation, as indicated by the presence of neutrophils both alone and with other inflammatory cells, observed under high-power field microscopy. The scale was adapted from the modified International ISO standard 10993-10. The categories were defined as follows: absent (0), mild (1–50), moderate (51–100), and intense (greater than 100). These ratings were then compared across groups using the linear-by-linear association test, also known as the ordinal (linear) χ2 test. Additionally, the type of inflammation was compared among groups using the χ2 test.
Go to :
RESULTS
For each group, Table 1 presents the percentage (%) of specimens exhibiting the various degrees of inflammation and presence of hemorrhage. The type of inflammation varied significantly among the groups (p = 0.001). The NC exhibited minimal inflammation, while the PC1 and PC2 displayed a mixed pattern of acute inflammation and hemorrhage (Figure 2). When cryotherapy was applied for 5 minutes, 60% of the subjects showed no signs of acute inflammation, while 40% exhibited moderate acute inflammation. The PC1 and PC2 and the group receiving cryotherapy for 1 minute demonstrated a significantly higher degree of inflammation (p = 0.0002) than the group receiving 5 minutes of cryotherapy. PMNs were virtually absent in the NC and in the samples that had received 5 minutes of cryotherapy. However, a significant increase was noted in cell count in the PC1 and PC2 and in the samples treated with 1 minute of cryotherapy. No significant differences were observed among groups in terms of hemorrhage, which was entirely absent in the NC and in the group receiving 5 minutes of cryotherapy (Figure 3).

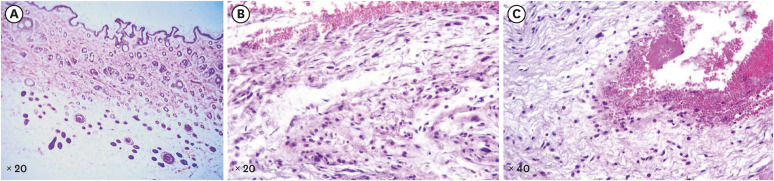 | Figure 2(A) Negative control showing the absence of inflammation. (B) Positive control showing the presence of hemorrhage and inflammation. (C) Presence of inflammation and abundant hemorrhage.
|
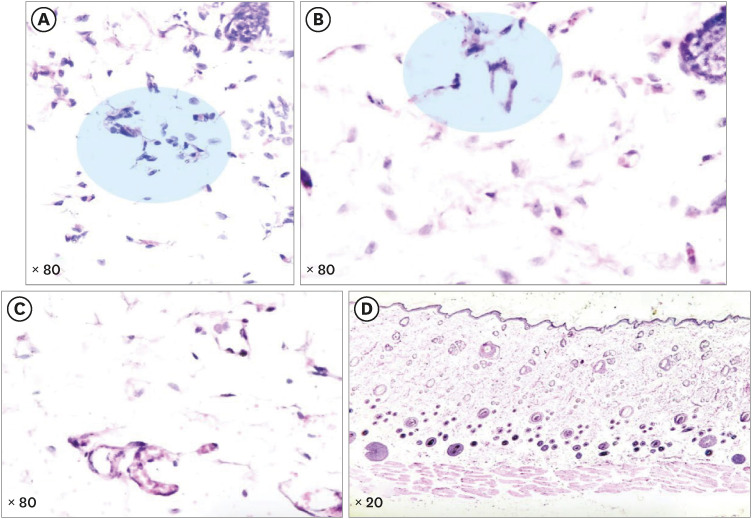 | Figure 3(A, B) Negative control showing the presence of fibroblasts and a few neutrophils. (C) Presence of a few neutrophils in an experimental group 2 (E2) sample. (D) Absence of inflammation or hemorrhage in an E2 sample.
|
Table 1
Percentage (%) of specimens per group and category, detailing the presence and degree of inflammation, hemorrhage, and neutrophils
![]()
Go to :
DISCUSSION
Patients who experience pain are typically prescribed anti-inflammatory medications following their treatment. However, a growing number of patients have medical contraindications, such as gastrointestinal complications or other health issues, that restrict the use of these medications. Therefore, alternative methods of postoperative pain management are crucial for these individuals.
Cryotherapy has recently emerged as an alternative method for managing postoperative pain in endodontics. Numerous studies suggest that the temperature of the intracanal irrigant used, along with the duration of its application, are important considerations in effective pain management.
Numerous studies have demonstrated the efficacy of intracanal, intraoral, and extraoral cryotherapy in reducing postoperative pain during endodontic treatment. This applies to teeth with either vital or necrotic pulp, as well as teeth with symptomatic apical periodontitis or normal periapical tissues [101213141520]. Intracanal cryotherapy is a cost-effective and easily administered treatment. This is because the clinician already has access to the root canal system during the procedure, and the treatment time is only minimally extended.
The mechanism of action and efficacy of cryotherapy have been documented, but standardization is still lacking regarding factors such as the duration of therapy in connective tissue [2122]. In the present study, adult rats were infused with a subcutaneous LPS suspension, followed by the application of cryotherapy at 2 different time intervals (1 and 5 minutes). To assess the degree of inflammation, tissue samples were obtained immediately after the application of cryotherapy, and histological analysis was performed. Prior to the experimental design of the present study, pilot studies were conducted on 6 rats. This pilot investigation revealed that acute inflammation was induced in the connective tissue 45 minutes after LPS infusion. This contrasted with the inflammation observed following catheter insertion and in healthy, non-infused tissue. The findings indicated that due to its invasive nature, the mere application of the catheter initiated an inflammatory process, albeit typically of a mild degree. The samples from the E1 and E2 comprised tissue in which inflammation had been induced and catheters had been implanted for the administration of 1- and 5-minute cryotherapy sessions. We found that administering a cold sterile saline solution, maintained at 2.5ºC for 5 minutes, reduced acute inflammation more effectively than a 1-minute cryotherapy session. According to prior studies, the difference between saline solution administered at 2.5°C through a catheter and the extraradicular temperature of 8.37°C, as previously demonstrated [12], should not produce different clinical outcomes in cryotherapy [121314].
Based on the findings of this in vivo study, we recommend administering a cold saline solution for 5 minutes as a method to alleviate acute inflammation.
The localized impact of cryotherapy can be attributed to a reduction in tissue temperature [21]. This decrease in temperature leads to vasoconstriction and a subsequent reduction in edema [22]. Vasoconstriction also lowers cellular metabolism, thereby reducing oxygen levels, which in turn limits the generation of tissue free radicals and cellular demand [212223]. The reduction in cellular demand decreases cellular recruitment and the production of pro-inflammatory mediators, which ultimately lessens the inflammatory process. In the present study, we noted a reduction in the accumulation of acute inflammatory cells in the E1 and E2, which was most dramatic when cryotherapy was applied for 5 minutes.
Regarding the effects of cryotherapy in endodontics, recent systematic reviews with meta-analyses have produced contradictory results. This discrepancy is likely due to the inclusion of randomized controlled trials with methodological deficiencies [24] or those deemed to provide low-quality evidence [25]. According to quantitative analysis, intracanal cryotherapy does not seem to significantly reduce post-endodontic pain [26]. However, another systematic review found that intracanal cryotherapy effectively reduced postoperative pain in teeth with symptomatic apical periodontitis [27]. The variation in results of studies across these systematic reviews could be attributed to differences in the endodontic techniques employed, the initial pulpal diagnosis, and (most notably) the presence or absence of symptomatic apical periodontitis versus normal apical tissues. Despite the lack of high-quality evidence, the benefits of intracanal cryotherapy have been extended to primary teeth, where it is seen as a simple, cost-effective, and non-toxic treatment for managing post-endodontic pain [28].
In a clinical setting, cryotherapy is typically administered after the completion of cleaning and shaping procedures, but before the application of intracanal medication or obturation. In previous endodontic clinical trials, cryotherapy was applied for 4 to 5 minutes, as suggested by medical studies. However, those trials did not evaluate whether shorter durations would be similarly effective, or whether longer periods would further decrease postoperative pain and inflammation. The present study was designed to determine whether a brief, 1-minute application of cryotherapy could be as effective as a 5-minute application in reducing connective tissue inflammation caused by LPS and catheter insertion. Future research will delve into the mechanisms behind the observed effects, examining aspects such as gene expression, cytokine production, and protein expression. This study did not include an analysis of cell-specific markers or the use of immunohistochemistry to identify inflammatory cells, which could be a focus of future research.
Go to :
 XML Download
XML Download