

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Endodontic treatment aims to fill in the space previously occupied by the dental pulp of the root canal system. A suitable sealing depends on the filling of the apical or coronal canal region and between the root canal walls. The filling material prevents microbial infiltration, reduces the risk of reinfection, and keeps residual levels of bacteria low [1]. Altogether these factors allow the repair of periradicular tissues, increasing the chances of an efficacious endodontic treatment [2].
One of the side effects of endodontic therapy is postoperative pain. Studies reported that postoperative pain could affect up to 69% of patients [345]. The development of postoperative pain is usually due to acute inflammation caused by the periradicular tissues. It starts a few hours after the endodontic treatment, and may be related to several factors [6]. Knowledge about the causes of postoperative pain from endodontic treatment is essential. Appropriate preventive measures can be adopted to significantly reduce the incidence of this disturbing and clinically undesirable side effect.
Among the factors that are associated with postoperative pain, the following stand out: the number of visits [4], irrigation solution [7], instrumentation protocol [8], the occlusal adjustment [9], and the filling material are also reported to be associated with postoperative pain after endodontic therapy [10]. Cytotoxic effects on periapical tissues have been reported following extrusion of the sealer during root canal filling, which causes periapical inflammation, necrosis, and pain [11]. The chemical composition of sealers also affects the tissue reaction [12].
Regarding the type of endodontic sealer, there are currently several types in the market. They can be classified according to their chemical constitution into zinc oxide eugenol-based sealers, calcium hydroxide-based sealers, epoxy resin-based sealers, and calcium silicate-based sealers (mineral trioxide aggregate [MTA] and bioceramics) [13]. Studies that evaluate postoperative endodontic pain with different endodontic sealers [1415161718] reported controversial results. While some studies found no substantial differences between sealers [14161719], others found significant differences among endodontic sealers [1518]. The intensity of inflammatory reactions in the apical region, and consequent endodontic postoperative pain, depends on several factors, one of which is the sealer composition [12].
Although a recent systematic review has been published, it evaluated only the comparison between epoxy resin-based sealers and calcium silicate-based sealers [20]. Furthermore, the contrasting results found in the endodontic literature on this topic, and the limited evidence, prompted us to explore further the relationship between postoperative pain and different endodontic sealers used to fill root canals. Thus, this review aims to compare all endodontic types of sealer used in the studies through a network meta-analysis. In the face of that, this systematic review and network meta-analysis aimed to answer the following focused research question: “Does the type of endodontic sealer (intervention and comparison) affect the postoperative pain (outcome) in patients who received endodontic treatment (participants)?”
MATERIALS AND METHODS
The methodology described in this study follows the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement [21] and in earlier publications [2223].
Protocol and registration
The study was registered in the PROSPERO database (CRD42020215314), and performed from December 2020 to March 2021 at the Paulo Picanço School of Dentistry, Fortaleza, Brazil.
Information sources and search strategy
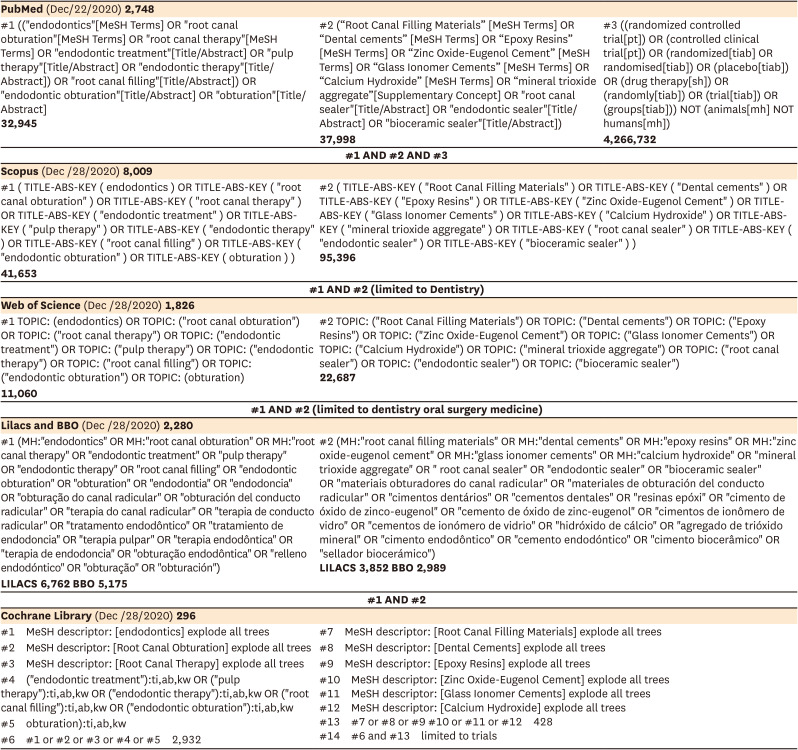
When surveying the PubMed database, the strategy was developed based on the concepts of the patient (patients who received endodontic therapy) and the intervention (different types of endodontic sealers). Within each concept, the controlled vocabulary and free keywords were combined with the Boolean operator “OR.” Then, the concepts were combined with the Boolean operator “AND” to restrict the search. A validated filter for randomized controlled trials (RCTs) was also used for the PubMed database (Table 1). Table 1 also lists other electronic databases used in the search strategy (Web of Science, Scopus, Cochrane Library, Latin American and Caribbean Health Sciences Literature database [LILACS], and Brazilian Library in Dentistry [BBO]). For the Scopus database, a limit for ‘Dentistry’ was used to perform the search; in the same way, a limit to dentistry oral surgery medicine was used to search the Web of Science database (Table 1). The reference lists of all primary studies were hand-searched for additional relevant publications. The link to related articles of each eligible study in the PubMed database was also retrieved for additional publications. No restrictions on publication date or languages were made.
Table 1
Electronic database and search strategy
The grey literature was evaluated by looking up the abstracts of the International Association for Dental Research and their regional divisions (1990–2020), dissertations and theses (ProQuest Dissertations and Theses Fulltext database, Periódicos Capes database), the System for Information on Grey Literature in Europe (SIGLE), and Google Scholar. Ongoing trials were searched in the following clinical trials registries: Current Controlled Trials (www.controlled-trials.com), International Clinical trials registry platform (http://apps.who.int/trialsearch/), the ClinicalTrials.gov (www.clinicaltrials.gov), Rebec (www.rebec.gov.br), and EU Clinical Trials Register (https://www.clinicaltrialsregister.eu).
Eligibility criteria
RCTs that compared postoperative pain in patients who received primary endodontic treatment (in single or 2-visit) in vital or non-vital pulp performed with different endodontic sealers were included. RCTs were excluded if: 1) they used the same endodontic sealer with different filling techniques; 2) patients who received endodontic retreatment; and 3) the study used different sealer brands but the same type of sealer.
Study selection and data collection process
After database screening, the duplicates were removed, and the articles were retrieved according to title and abstracts. Full-text articles were obtained by 2 independent reviewers (C.M.C.M. and J.L.G.), and they were classified according to the eligibility criteria. Pilot-tested, customized extraction forms were used to register details about the studies, such as study design, participants, interventions, and outcomes. Each study received an identification number (study ID), combining the first author’s name and the publication year. Information such as pain evaluation criteria, time of evaluation of pain, tooth type, pulp condition, and number of sessions were collected. The authors were not contacted for further information to avoid recall bias. We collected data about the risk and intensity of pain. During this process, disagreements between the two reviewers were resolved through discussion, and a third reviewer (A.R.) was consulted if needed.
Risk of bias in individual studies
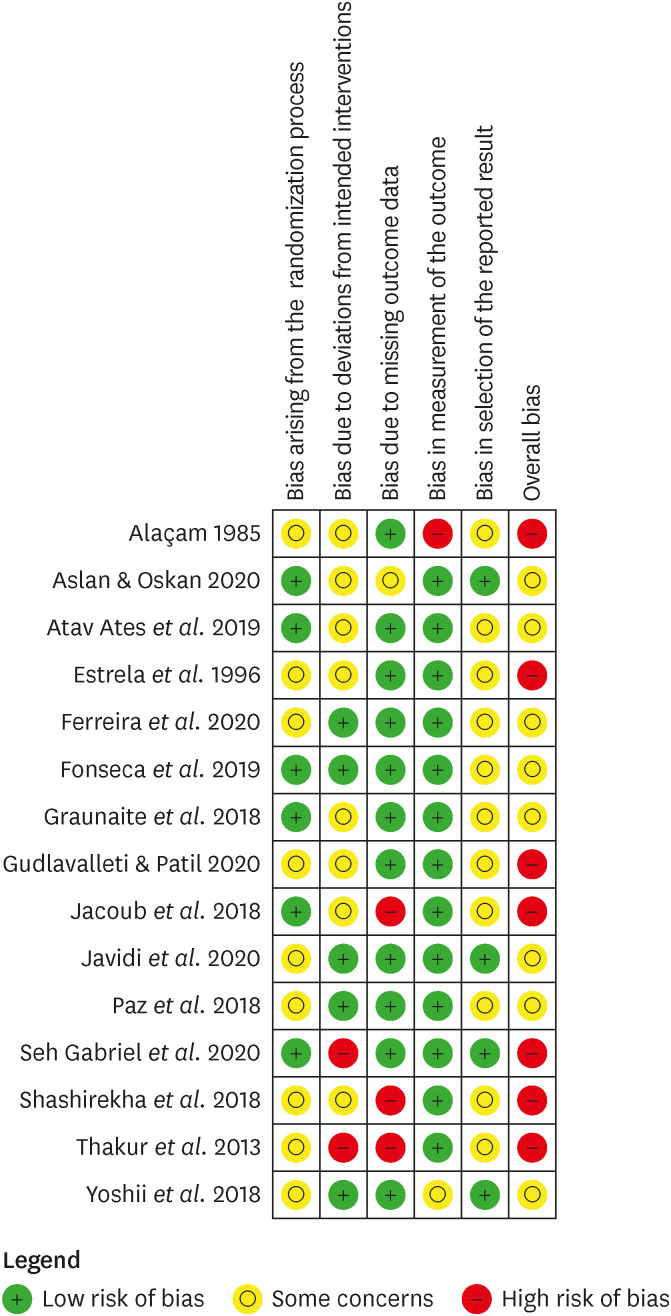
The risk of bias (RoB) of the individual studies was evaluated by 2 independent evaluators (C.M.C.M. and J.L.G.) using the RoB version 2.0 from the Cochrane Collaboration [24]. This tool considered the following items:
• Bias arising from the randomization process,
• Bias due to deviations from intended interventions (effect of the assignment to the intervention),
• Bias due to missing outcome data,
• Bias in the measurement of the outcome,
• Bias in the selection of the reported result and
• Overall bias.
Each domain had its risk of bias classified into ‘low risk of bias,’ ‘some concerns,’ or ‘high risk of bias.’ If the study result was at low risk of bias in all domains, the overall bias was judged as ‘low risk.’ If at least one domain was at ‘some concerns,’ the overall risk of bias was ‘some concerns.’ If several domains were at ‘some concerns’ or at least one domain at ‘high risk,’ the overall domain was at high risk of bias. Any disagreements between the reviewers were solved through discussion and, if needed, by consulting a third reviewer (A.R.).
Summary measures
The endodontic materials evaluated were epoxy resin-based, calcium silicate-based, zinc-oxide eugenol-based, and calcium hydroxide-based sealers. The primary outcome of this study was the risk of postoperative pain (POP) and POP intensity. For each study, we extracted the number of patients with POP and the total number of patients in each study arm 24 hours after endodontic treatment to calculate the risk ratios (RRs) and the 95% confidence intervals (CIs).
Additionally, the total number of participants, and the mean and standard deviation of the intensity of POP (0-10 VAS scale) in each study arm at 24 hours were extracted to calculate the mean difference and the 95% CIs. Transitivity was assumed to occur in all studies, meaning that the different interventions were sufficiently similar to provide valid indirect inferences.
Statistical analysis
Firstly, a traditional meta-analysis of the direct evidence of the risk of postoperative pain 24 hours after endodontic treatment with different endodontic sealers was conducted, deriving a RR and a 95% CI. Heterogeneity was assessed using the Cochran Q test and I2 statistics.
Subsequently, a network meta-analysis (NMA) was performed by using the Bayesian model with the statistical package geMTC in R statistical software (version 3.4.2) and JAGS (http://mcmc-jags.sourceforge.net). The Mixed Treatment Comparison (MTC) methodology, supported by the Markov Chain Monte Carlo hierarchy, was chosen to carry out the NMA. This model allows for the simultaneous comparison of different treatments by incorporating trials with two, three, or more arms. Random effects models with the DerSimonian and Laird variance estimator and the inverse of the variance method were used. The convergence was based on the Brooks Gelman-Rubin criteria with inspection of trace plots, and 20,000 interactions were undertaken for four chains at a thinning interval of 4. Heterogeneity was assessed using the Cochran Q test and I2 statistics.
The network meta-analysis results were displayed in point estimates, 95% credible intervals (95% CrI). The relative ranking for each intervention using the Surface Under the Cumulative Ranking curve (SUCRA), estimated within the Bayesian framework, was calculated whenever significant differences between treatments were observed. A SUCRA value of 100% indicates the treatment is the most effective in the network, while 0% suggests it is the least effective. The larger the SUCRA value, the better the rank of an intervention in the network. All analyses were implemented using the meta and geMTC packages of the R statistical software program.
Assessment of consistency
A further assumption of NMA is consistency, that is, the statistical agreement between the direct and indirect comparisons. The consistency assumption is the statistical manifestation of transitivity and depends on the statistical agreement between different sources of evidence. Statistical inconsistency was checked using posterior plots and Bayesian p values produced using the node-splitting method proposed by Dias et al. [25] and by testing the agreement between direct and indirect evidence. Consistency is observed if the p value of the analysis is more significant than the significance level.
Additionally, a global test was used for loop inconsistency by plotting the posterior mean deviance of the individual data points in the unrelated mean (relative) effects (UME) in the inconsistency model against their posterior mean deviance in the consistency network meta-analysis model. The consistency model fits the data well whenever the data points are in the line of equality.
Small study effects and publication bias
If the comparison included more than ten studies, publication bias was assessed by funnel plot asymmetry for each pairwise comparison. Small-study effects were evaluated by drawing a comparison-adjusted funnel plot that accounts for the fact that different studies compare different sets of interventions.
Assessment of the quality of evidence using the grading of recommendations: assessment, development, and evaluation
The Grading of Recommendations Assessment, Development, and Evaluation (GRADE) approach was followed to appraise the confidence in estimates derived from the network meta-analysis of retention rates following the Puhan et al. [26] approach. RCTs start at high confidence and can be rated down to moderate, low, and very low confidence. This rating is based on indirectness, imprecision, inconsistency (or heterogeneity), and publication bias. If direct and indirect estimates were similar (i.e., coherent), the higher ratings were assigned to the network meta-analysis estimates.
RESULTS
Characteristics of included studies
After the database screening and removal of duplicates, 11,601 articles were identified (Figure 1). After title screening, 85 articles remained; this number was reduced to 17 after careful examination of the abstracts (Figure 1). Two articles were excluded as the same type of endodontic sealer was used in both study groups [2728].
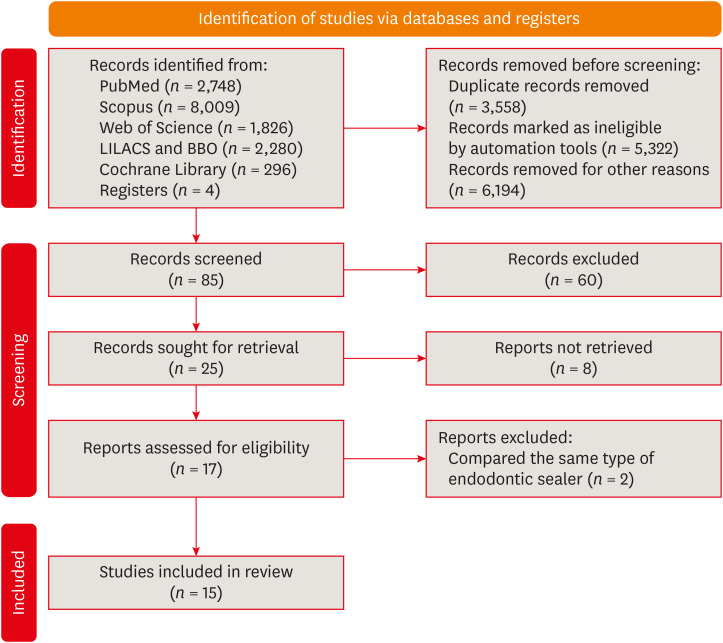
A total of 15 articles remained for qualitative evaluation and are characterized below (Tables 2 and 3). Only one study had a spit-mouth design [29]; the other had a parallel design. The mean age reported was 40.5 years [1416171829303132]; female patients prevailed in all studies that reported the gender of participants [1016171829303132]. Some studies did not report the age [1533343536] or gender of participants [141533343536]. The dropouts varied from 0 to 8 [151617181929303132]. Some studies did not report the dropouts [14343536].
Table 2
Summary of the studies selected for this systematic review: Part 1
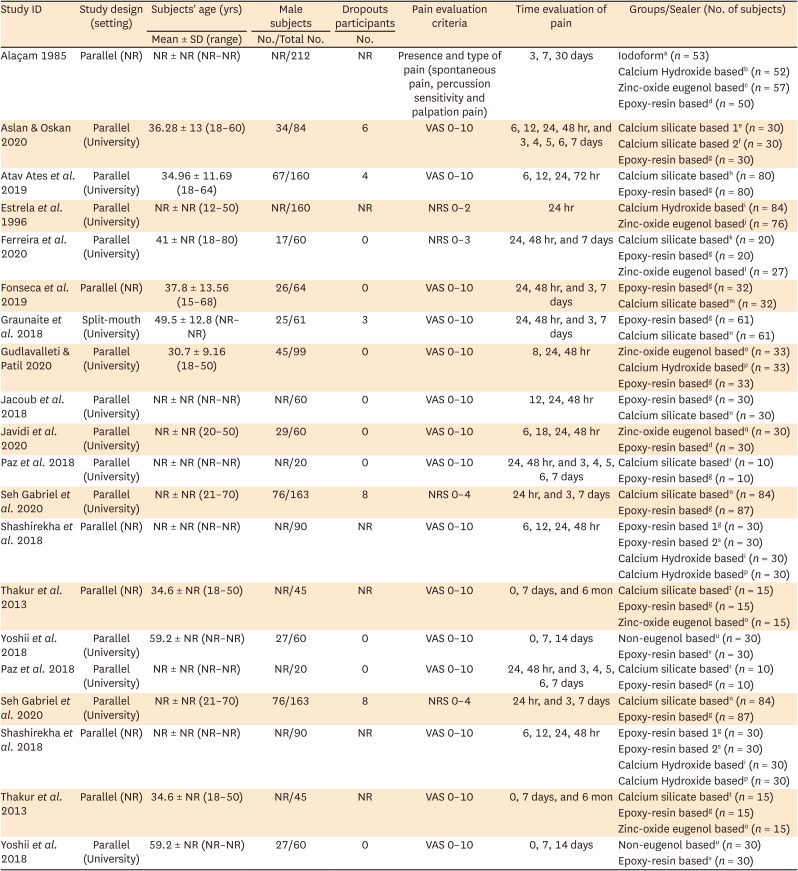
ID, identification; SD, standard deviation; NR, not reported; VAS, visual analog scale (a 10-cm horizontal line with words “no pain” at one end and “worst pain” at the opposite end); NRS, numerical rating scale.
Manufacturer information is followed as: aIodoform paste, NR; bOx-para, NR; cEndomethasone, Septodont, Saint-Maur-des-Fossés, France; dAH26, Dentsply Maillefer, Ballaigue, Vaud, Switzerland; eEndoseal MTA, Maruchi, Wonju, Korea; fEndoSequence BC Sealer, Brasseler, Savannah, GA, USA; gAH Plus, Dentsply Maillefer, Ballaigue, Vaud, Switzerland; hIRoot SP, Innovative BioCeramix Inc, Vancouver, BC, Canada; ISealapex, Kerr, Brea, CA, USA; jFillcanal, Dermo Laboratório Ltda. Rio de Janeiro, RJ, Brazil; kMTA Fillapex, Angelus, Londrina, PR, Brazil; lEndofill, Dentsply, Petrópolis Ind. e Com., Rio de Janeiro, Brazil; mSealerplus BC, MKLife Medical and Dental Products, Porto Alegre, RS, Brazil; nTotal Fill BC, FKG Dentaire SA, La Chaux-de-Fonds, Switzerland; oTubli-Seal EWT, SybronEndo, Glendora, CA, USA; pApexit Plus, Ivoclar Vivadent, Schaan, Liechtenstein; qDeveloped in the Dental Material Research Center, Mashhad University of Medical Sciences, Mashhad, Iran; rBioRoot RCS, Septodont, Saint-Maur-des-Fossés, France; sResino Seal, Amrith Chemicals and Mineral Agency, India; tProRoot MTA, Dentsply Tulsa, Johnson City, TN, USA; uCanals N, Showa Yakuhin Kako Co., Ltd., Tokyo, Japan; vHybrid Root Seal, Sun Medical, Moriyama, Japan.
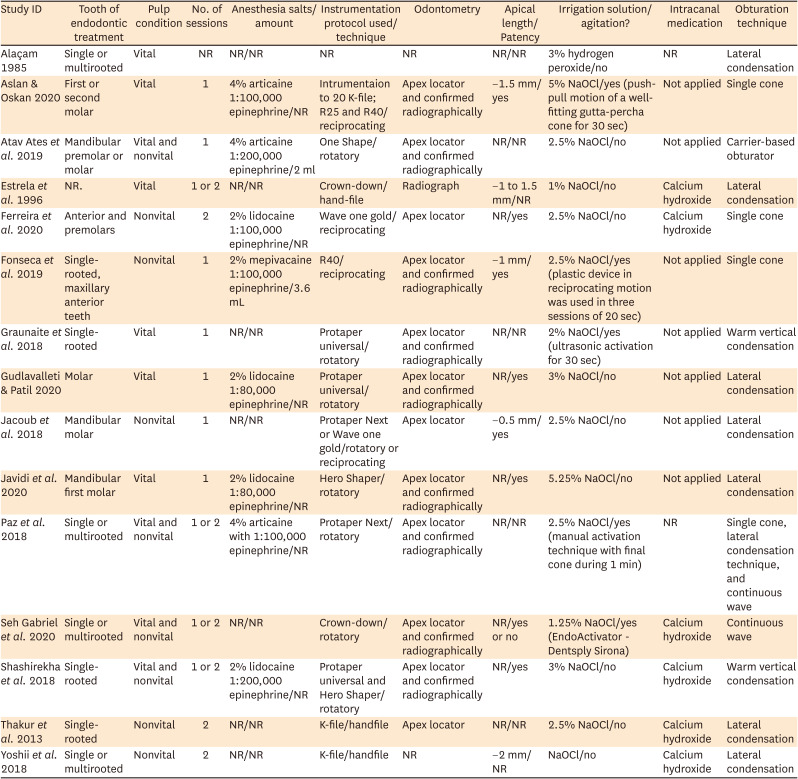
Table 3
Summary of the studies selected for this systematic review: Part 2
Most studies used visual analogic scale (VAS) 0–10 to evaluate the postoperative pain [1014151617182930313334]. However, the numerical rating scale (NRS) was used in three studies [193235]. Both scales were limited to tooth pain. The pain was predominantly evaluated 24 hours after treatment [101516171819293132333435]. Some studies evaluated the pain at 7 days [1415161719293032]. Longer periods were also evaluated, being that one study evaluated the pain after one month [36] and another at six months [14].
The most used sealers in the studies were epoxy-resin based, calcium silicate-based, zinc-oxide eugenol based, and calcium hydroxide based (Table 2). The tooth in which the endodontic treatment was performed varied a lot among studies (single or multirooted, anterior or posterior, maxillary, or mandibular teeth). The vitality of the pulp before treatment was also different in the studies included; in 6 studies, the pulp was vital [101718293536], and in 5, the pulp was nonvital [1416303233]. Both pulpal conditions were included in the remaining 4 studies [15193134].
In most studies, the endodontic treatment was performed in 1 session [10161718293133]. Some studies used 1 or 2 clinical sessions [15193435]. However, some studies performed the therapy in 2 sessions [143032]. Only one study did not report this information [36]. When intracanal medication was applied, calcium hydroxide was used [141930323435].
The 2% lidocaine was the anesthetic salt most used in the studies [10183234], followed by 4% articaine [151731]. Some studies did not inform the local anesthetic [14192930333536]. Manual K-files, rotatory or reciprocating instruments were used for the endodontic therapy, since one study did not report this information [36]. Most studies conducted odontometry with an apex locator and confirmed it radiographically [101516171819293134]. The apical length varied from −0.5 to −2 mm from apices [1617303335]. The odontometry method was not reported in 2 studies [3036]. Patency maintenance was reported in some studies [101617183334].
Regarding the endodontic irrigant, sodium hypochlorite (1% to 5.25%) was used in most studies. Only one study used 3% hydrogen peroxide [36]. Most studies did not utilize any form of irrigant agitation, but manual agitation with de final cone [1517], plastic device in reciprocating motion [16], sonic [19] and ultrasonic activation [29] were used in final irrigation. The filling techniques varied, including lateral compaction, vertical compaction, single cone, continuous wave, and the carrier-based obturator (Table 3).
Risk of bias within studies
Evidence network
Figure 3 displays the evidence networks of the risk (Figure 3A) and intensity (Figure 3B) of the postoperative pain at 24 hours. Four endodontic sealers (epoxy resin-based, calcium silicate-based, zinc-oxide-based, and calcium hydroxide-based sealers), represented by each node, were used in the eligible studies. The strategies connected by a line represent direct comparisons, with the number of pairs (from RCTs) reflected by their thickness and the number of patients represented by the node size.
Figure 3
Network plot presenting the trial data contributing evidence comparing different endodontic sealers. (A) Risk of postoperative pain: 7 trials, 4 groups, 701 participants. (B) Intensity of postoperative pain: 12 trials, 5 groups, 1,319 participants. The size of the nodes represents how many times the exercise appears in any comparison about that treatment and the width of the edges represents the total sample size in the comparisons it connects.
ER, epoxy resin; CS, calcium silicate; CH, calcium hydroxide; ZOE, zinc-oxide eugenol.
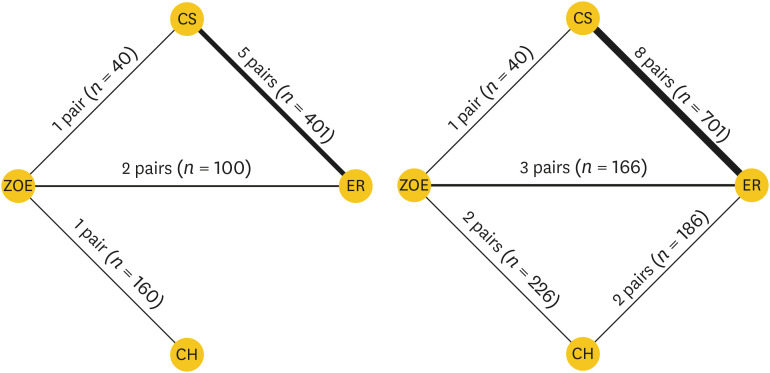
In the risk of POP evidence network (Figure 3A), 7 studies were included, with 6 being 2-arm and only one 3-arm study [16]. There were direct comparisons for four of the 6 pairwise comparisons, and only the pairs of calcium hydroxide/calcium silicate and calcium hydroxide/epoxy resin did not have direct evidence. A total of 641 patients were included in this network, with 149 events.
Twelve studies were included in the intensity of POP evidence network (Figure 3B). These were ten 10-arm and only two 3-arm studies [1629]. There was direct evidence for 5 pairwise comparisons (except for the pair calcium hydroxide/calcium silicate). A total of 1,160 patients were evaluated in the evidence network.
Synthesis of the network results
1. Risk of postoperative pain
Traditional pairwise meta-analyses for all possible pairs can be found in Figure 4. The pair calcium silicate/epoxy resin had the highest number of studies (n = 5), followed by the pair zinc-oxide eugenol (ZOE)/epoxy resin (n = 2), and the pairs calcium hydroxide/ZOE and ZOE/calcium silicate with only 1 RCT included. No significant differences were observed between the endodontic materials in the direct comparison studies. No heterogeneity was found in the pairwise comparisons with more than two studies (I2 = 0%; p > 0.05).
Figure 4
Traditional pairwise meta-analysis for all possible pairs for the risk of postoperative pain.
RR, risk ratio; CI, confidence interval.

Table 4 summarizes the indirect and pooled estimates for the study comparisons. In line with the direct evidence, MTC values did not observe any difference among the endodontic materials as the 95% CI of all comparisons incorporates the null value of 1. Inconsistency between direct and indirect evidence was not observed with the node splitting method and the global assessment for loop inconsistency (Figure 5).
Table 4
GRADE summary of findings and table for different outcomes
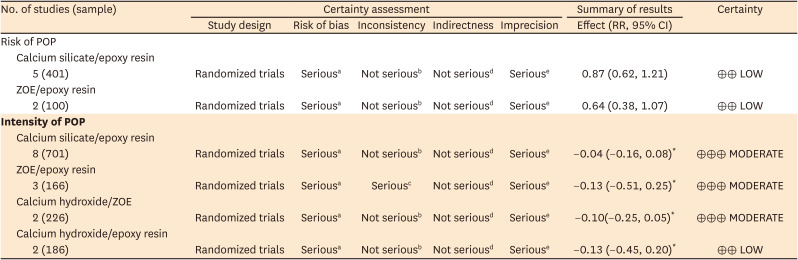
Note: GRADE Working Group grades of evidence. High certainty: We are very confident that the true effect lies close to that of the estimate of the effect. Moderate certainty: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low certainty: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect. Very low certainty: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect.
GRADE, Grading of Recommendations Assessment, Development, and Evaluation; RR, risk ratio; CI, confidence interval; POP, postoperative pain; ZOE, zinc-oxide eugenol; PICO, Population, Intervention, Comparator and Outcomes.
*Summary of results of ‘Intensity of POP’ is presented as effect mean difference with 95% CI.
aMost of the studies are at high/unclear risk of bias; bSimilar effect estimates among different studies, overlap of 95% CI, low I2, and nonsignificant p value; cDifferent effect estimates among different studies, overlap of 95% CI, high I2, and nonsignificant p value; d The evidence comes from adults undergoing root canal treatment, and we can apply to the patients of our PICO question; e95% CI cross-the line of null effect (1.0)—rated down one level due imprecision.
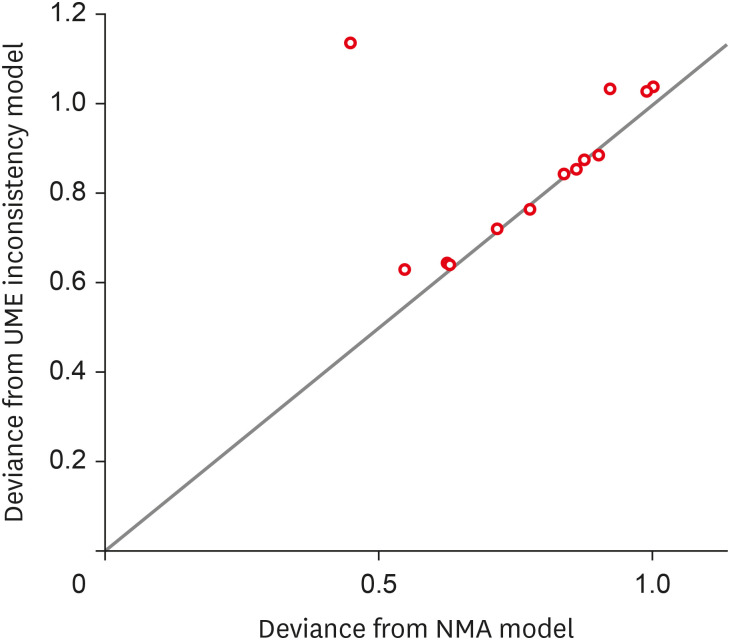
Figure 5
Global assessment for loop inconsistency for risk of postoperative pain. This plot represents each data points’ contribution to the residual deviance for the NMA with consistency (horizontal axis) and the UME inconsistency models (vertical axis) along with the line of equality. The points on the equality line mean there is no improvement in model fit when using the inconsistency model, suggesting no evidence of inconsistency. Points above the equality line represent minor residual deviance for the consistency model, indicating a better fit in the NMA consistency model. Points below the equality line mean they have a better fit in the UME inconsistency model.
NMA, network meta-analysis; UME, unrelated mean effect.
As no significant difference was found in the pairwise comparisons, SUCRA values were not calculated, since they could lead to a misunderstanding of the study findings. SUCRA provides valuable information only when differences between treatments are detected.
2. Intensity of postoperative pain
Traditional pairwise meta-analyses for all possible pairs can be found in Figure 6. The calcium silicate/epoxy resin pair was the one with the highest number of studies (n = 8), followed by the ZOE/epoxy resin pair (n = 3) and the calcium hydroxide/ZOE and calcium hydroxide/epoxy resin pairs with 2 studies. The ZOE/calcium silicate pair had only 1 RCT included. No significant differences were observed between the endodontic materials in the direct comparison studies.
Figure 6
Traditional pairwise meta-analysis for all possible pairs for the intensity of postoperative pain.
SD, standard deviation; MD, mean difference; CI, confidence interval.
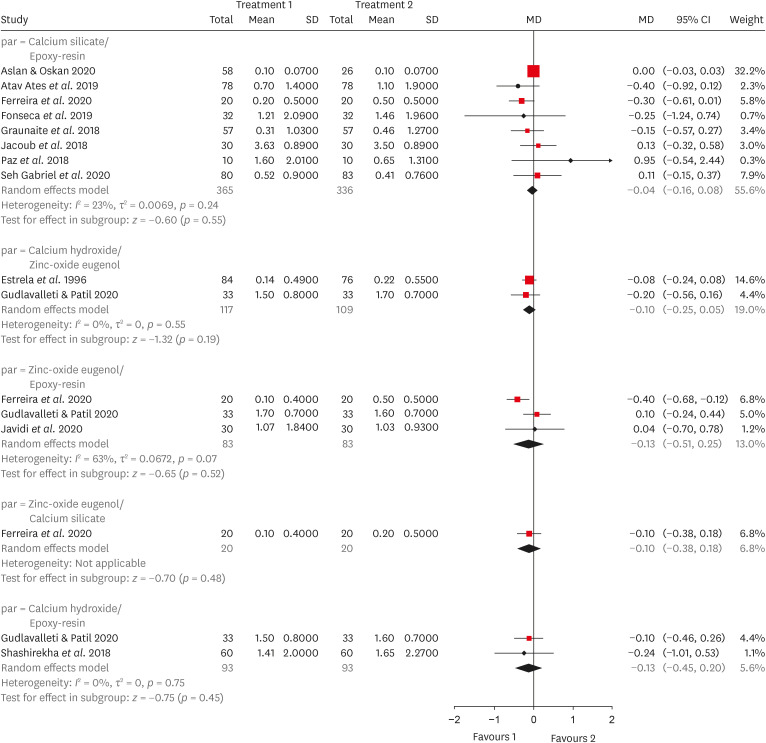
In the calcium silicate and epoxy-resin pairwise comparison, the mean difference was −0.04, varying from −0.16 to 0.08. In the zinc-oxide-eugenol and epoxy-resin pairwise comparison, the mean difference was −0.13, varying from −0.51 to 0.25 (Figure 6).
No heterogeneity was found in the pairwise comparisons with 2 or 8 studies (I2 = 0%; p > 0.05; I2 = 23%; p > 0.05, respectively). A moderate heterogeneity was found in pairwise comparisons ZOE/epoxy resin (I2 = 63%; p > 0.05).
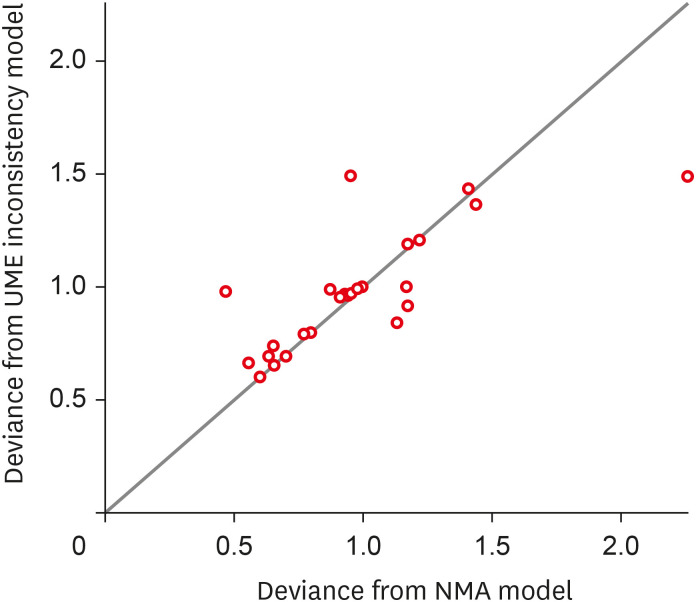
SUCRA values were not calculated as no significant differences were observed in the pairwise comparisons. No inconsistency was confirmed with the node splitting method or the global assessment for loop inconsistency (Figure 7).
Figure 7
Node splitting method and the global assessment for loop inconsistency for postoperative pain intensity. This plot represents each data points’ contribution to the residual deviance for the NMA with consistency (horizontal axis) and the UME inconsistency models (vertical axis) along with the line of equality. The points on the equality line mean there is no improvement in model fit when using the inconsistency model, suggesting no evidence of inconsistency. Points above the equality line represent minor residual deviance for the consistency model, indicating a better fit in the NMA consistency model. Points below the equality line mean they have a better fit in the UME inconsistency model.
NMA, network meta-analysis; UME, unrelated mean effect.
Synthesis of certainty of the evidence
As regards the quality of the evidence for the network evidence can be seen in Table 4. The certainty of the evidence is evaluated for each pairwise comparison for each outcome. In most of the pairwise comparisons in the risk of pain network evidence, the certainty of the evidence was graded as low because most studies were judged to be at high risk of bias due to imprecision. However, the calcium hydroxide vs. calcium silicate and calcium hydroxide vs. epoxy resin pairs were graded as very low (high risk of bias, imprecision, and indirectness).
Regarding pain intensity, the certainty of the evidence was graded as moderate since most studies presented high/unclear risk of bias. The pair of calcium hydroxide vs. epoxy resin was graded as low because of the studies’ high/unclear risk of bias and indirectness.
DISCUSSION
This systematic review aimed to answer whether different sealers are related to lower pain risk and intensity after root canal treatment. The meta-analysis showed differences in the risk and intensity of postoperative pain when different endodontic sealers were used in root canal filling.
The physical and biological properties of filling materials must always be considered when choosing an endodontic sealer. There are currently several types of endodontic sealers on the market. They have been classified according to their chemical constitution into zinc oxide eugenol-based, calcium hydroxide-based, epoxy resin-based, and calcium silicate-based sealers (MTA and bioceramics) [37]. ZOE-based sealers are the oldest used in endodontic treatment. Zinc oxide is a valuable component of these sealers, and highly effective as an antimicrobial agent [37]. In addition to their antibacterial effect, the calcium hydroxide-based sealers have a different osteogenic-cementogenic potential which favors the tissue regenerative capacity by leaching calcium and hydroxyl ions into the surrounding tissues [38]. Resin-based sealers have launched marketing claiming their adhesive properties. Bioceramic sealers (calcium silicate-based) have recently been established [37]. These sealers have positive biological effects with low damage to vital tissues [39].
Regarding the type of sealer used, the resin sealer was chosen by most eligible studies was AH-Plus (Dentsply Maillefer, Ballaigues, Switzerland) [14151617181929323334], which is slightly cytotoxic, as it releases monomers such as bisphenol A diglycidyl ether and its extrusion can delay periapical healing [40]. On the other hand, the silicate-based sealers used in the eligible studies (Total FillBC, Sealer Plus BC, iRoot SP EndoSequence BC, and Endoseal MTA) do not have resin in their composition, have a shorter setting time, better cell viability and cell migration capability when compared to AH-Plus [40]. However, Paz et al. [15] showed that patients who received root canal treatment with the Single cone plus calcium silicate-based sealer referred postoperative pain more frequently than those with epoxy resin-based sealer, which reveals conflicting results.
Another study that compared a nano-sized zinc-oxide eugenol powder particles (NZOE) sealer with a resin-based sealer (AH26) showed that the use of NZOE sealer was associated with significantly lesser pain than the use of AH26 in studied patients. This result can be explained due to the mild-to-moderate irritating effects of AH26 when freshly prepared, and the toxicity is due to the release of a small amount of formaldehyde, epoxide bisphenol resin, or amines during the chemical setting process [41].
When endodontic sealers are placed in the root canals, they may leach or be extruded to the periodontal tissues, apical foramina, and lateral root canals. They can potentially affect the healing process of the periodontium. When this happens, a local inflammatory reaction may occur soon after root canal filling, releasing several chemical mediators of the inflammation resulting in postoperative pain [42].
The most severe pain occurs up to 24 hours after filling of the root canal, and it decreases over time [28]; this was why we chose this period to perform the network meta-analysis, as the studies reported different periods. In due course of time, the extruded sealer is wholly removed, creating a space that eventually promotes healing, reducing pain and inflammation symptoms [43]. The problem with limiting pain evaluation to 24 hours is that there could be other reasons for pain, such as injection [44], clamp trauma to soft tissues [45], biting pain (occlusion) [9], and temporomandibular pain [46].
Many studies included in this review did not assess the risk of postoperative pain [1417183031333436], however, this data could be easily obtained and reported. All meta-analyses for all possible pairs for the risk of postoperative pain (calcium silicate/epoxy resin, ZOE/calcium silicate, ZOE/epoxy resin, and calcium hydroxide/ZOE) showed no difference between sealers (Figure 4), which agrees with the data of a previous systematic review [20].
The intensity of inflammatory reaction and the intensity of pain is affected by different factors. Some authors claim that the type of endodontic sealer can be one of these factors [47]. However, the present study did not observe any differences in the postoperative pain intensity when different endodontic sealers were used to fill the root canal, as shown in Figure 6, which should be interpreted with caution as most of the eligible studies included in this systematic review were classified as at some concerns or high risk of bias and have drawn attention to the conduction of RCTs with better methodology.
Although there are conflicting results in the literature regarding postoperative pain resulting from filling with different endodontic sealers, most studies show no difference in the risk and intensity of postoperative pain [1819293335], which agrees with the results of this systematic review. Although 15 studies were included, most compared epoxy resin-based and calcium silicate-based sealers [1516171929313233], showing the need for further studies to assess postoperative pain with other sealers.
In this systematic review, most eligible studies were classified at some concerns about the randomization process’s item bias. This is problematic because adequate randomization balances known and unknown prognostic factors in allocating treatments. In addition to randomization, allocation concealment is also essential, and it protects the randomization process so that the assigned treatment is unknown before the patient is enrolled in the study. Proper management of these 2 domains minimizes selection bias [24]. There is evidence that improper conduction of these steps in RCTs increases the likelihood of systematic errors [48]; studies with poor methodological quality tend to overestimate the results, favoring the intervention in the test group [49].
Another concern related to the primary eligible articles was the poor report of the outcome result [50]. Ideally, a study protocol should be published a priori so that readers may check whether the researchers selected one specific result or statistics based on the significance of the results. When the effect estimate that is fully reported in a publication has been chosen from among multiple measurements or analyses (e.g., trialists perform multiple adjusted analyses yet only report that which yielded the most favorable effect estimate) [24], the study may be at some concerns or high risk of bias in the selection of the reported results.
All these factors, along with imprecision of the effect estimates, reduce the overall results’ reliability and explain why the certainty of the evidence was graded as low for the risk of postoperative pain. In general, results are imprecise when studies include relatively few patients and report few events and thus have a wide CI around the estimated effect. Regarding the postoperative pain intensity, the certainty of the evidence was graded as moderate because imprecision was not observed, but even so, the results had concerns regarding the risk of bias in the studies.
Apart from the risk of bias of the studies, other aspects deserve discussion. It is difficult to ascribe the risk and intensity of pain to any specific factor in clinical research of endodontic therapy because root canal treatment comprises a complex of procedures involving anesthesia technique, endodontic access, chemo-mechanical debridement, and root canal filling. There are many protocol variations within trials, and perhaps they may play a more critical role in postoperative pain than the endodontic filling material itself.
Among the variations observed, we can cite: 1) the endodontic treatment timeframe. The procedure in the eligible studies was done in a single- or multiple-visit therapy. Earlier investigators have already described lower pain intensity in single-visit therapies [515253]; 2) the irrigation device. The negative apical pressure irrigation device can significantly decrease post-endodontic pain intensity when compared to conventional needle irrigation [5455]; 3) the pulp condition. Teeth with vital pulp produce a higher risk and intensity of postoperative pain than teeth with necrotic pulp tissue [56]; 4) endodontic filling technique. Alonso-Ezpeleta et al. [57] demonstrated that the Thermafil technique showed higher postoperative pain levels compared to cold lateral compaction of gutta-percha and the backfill-Thermafil technique. The probable reason for postoperative pain with the Thermafil technique might be the extrusion of gutta-percha; 5) the teeth of endodontic treatment. Pain after endodontic treatment is mainly related to multirooted teeth and could be attributed to the variations in root canal morphology [58] and the inaccessible auxiliary canals; 6) the patient’s gender. Some studies have shown that men and women differ in their responses to pain and point out that women are at a substantially greater risk for many clinical pain conditions, such as tooth pain [5960].
Although a previous systematic review evaluated postoperative pain by comparing epoxy resin-based sealers and calcium silicate-based sealers after endodontic treatment [20], other sealers were also studied; thus, this systematic review includes all possible comparisons evaluated in RCTs of endodontic materials using a Bayesian network meta-analysis, which is especially important because there are different endodontic sealers available on the dental market.
A network meta-analysis explores all available direct and indirect evidence, producing more accurate intervention effects estimates than a single direct or indirect estimate [6162]. In addition, network meta-analysis can provide information for pairwise comparisons of interventions that have never been evaluated in individually randomized trials. The simultaneous comparison of all interventions of interest in the same analysis allows the estimation of their relative ranking for a given result [63].
Another systematic review evaluated the in vitro and in vivo biocompatibility of root canal sealers including the commercially available sealers [64]. Although they showed that root canal sealers exhibit variable toxic potential at the cellular and tissue level, RCTs were carried out after the publication of this review. Therefore, we could not compare the level of evidence produced by clinical trials and in vitro and in vivo studies.
Conducting a well-designed RCT with large sample size and power is recommended to detect an essential clinical difference in the risk and intensity of postoperative pain after root canal filling with different endodontic sealers.
Another aspect that deserves attention is the measurement of the postoperative pain outcome. Each person’s pain threshold is unique and heavily dependent on their cultural, individual, and economic background [65]. Therefore, the postoperative pain may vary significantly within studies as they are conducted in different populations. The 0–10 VAS pain scale was the most used in the studies surveyed, but 0–3 NRS was also used. The decision to use VAS or NRS pain scales should consider the type of pain (acute or chronic), temporal aspects of pain reporting (duration and frequency), and target disease study population, among other factors. Another important consideration is the implementation of NRS or VAS since in-clinic settings allow for close supervision of instrument administration, ensuring proper data collection, while outpatient settings provide little or no control over instrument administration. The VAS instrument is a valid and reliable method widely used in the endodontic literature [35466]. It is best managed in a clinical setting, while the NRS instrument can be used effectively in both environments [67]. Although patients prefer the verbal rating scale because it is more straightforward than other scales, it is considered the least sensitive of the scales. The numerical rating scale is more efficient, relatively easy to interpret, and presents greater statistical sensitivity [68].
The ratings of the quality of the evidence for the network evidence varied from very low to moderate for each pairwise comparison for each outcome. The reasons for that were the high risk of bias and imprecision. The proportion of information from studies at high risk of bias is sufficient to affect the interpretation of results. In general, results are imprecise when studies include relatively few patients and few events and thus have a wide CI around the estimated effect. In this case, one may judge the quality of the evidence lower than it would be considered because of the resulting uncertainty about the results [69].
Every systematic review has the limitation that the research question is very specific, which makes it difficult to assess other factors that may be related to postoperative pain, so the objective of the clinical studies included in this review was to evaluate only postoperative pain in teeth filled with different endodontic sealers, not considering the different factors that could be evaluated. Taking that into consideration, different systematic reviews with specific questions about each factor that can lead to endodontic postoperative pain should be performed.
CONCLUSIONS
No significant difference (with low certainty of the evidence) was detected in the risk of postoperative pain in the comparisons between eugenol-based, calcium hydroxide-based, epoxy resin-based, and calcium silicate-based endodontic sealers. Similarly, no difference in postoperative pain intensity was observed between these comparisons, but the certainty of the evidence for this outcome was graded as moderate. As several factors may be related to endodontic postoperative pain, further systematic reviews with specific questions about these factors should be performed.
 XML Download
XML Download