

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Composite resins are the most commonly used material for direct restorations of anterior and posterior teeth [12]. To perform these direct composite restorations, the incremental technique is recommended to reach an acceptable degree of conversion and to reduce the stress generated by polymerization shrinkage, which can cause failures in the bonded interface [34]. However, despite its advantages, the incremental technique is time-consuming and requires longer clinical appointments [14]. In order to decrease the clinical time and facilitate the restorative technique (mainly in posterior teeth), bulk-fill composite resins were introduced as an alternative to conventional composites [35]. These bulk-fill composite resins can be placed in large increments, with thicknesses ranging from 4 to 6 mm, depending on the material, and with no increase in the light-curing time [3].
Composite resins reach high degrees of conversion as a result of a chemical reaction between resinous monomers producing a rigid network of polymers [6]. Adequate polymerization ensures better optical, physical, and mechanical properties, with less release of residual monomers, greater color stability, and greater mechanical and wear resistance [789]. The degree of conversion of composite-based materials is affected by intrinsic and extrinsic factors, such as composite resin composition, the photoinitiator system, temperature, photoactivation time, and the inherent characteristics of the light-curing units (LCUs) (type of light, light tip, irradiance, and light output) [23510111213141516171819]. Therefore, LCUs must emit enough light to guarantee an adequate degree of conversion and good physical and mechanical properties throughout the entire increment. A greater irradiance emitted by the LCU enables a greater conversion degree of the material and deeper light penetration into the restorative material increment [20]. LCU irradiance is defined as the radiant power (mW) received over the target surface area (cm2) [2122]. Insufficient monomer conversion can significantly influence the final properties of the composite resin and result in restoration failure [2324].
In recent years, with advances in dental materials, the newest light-emitting diode (LED) curing devices emit high irradiance, allow easy handling, and have a long life span [25]. However, each brand has different specifications, such as size, weight, price, and, mainly, irradiance. An LCU should produce a light irradiance of at least 500 mW/cm2 for 10 and 20 seconds for incremental activation; however, several studies showed that many devices in dental practice do not reach sufficient irradiance [19262728]. To obtain a satisfactory result of resin polymerization, it is necessary for the device to maintain a high level of intensity and stability in light emission. Several factors—material-related, operator-related, and unit-related—can affect the light transmittance effectiveness and reduce the light output from the tip [24]. Among the LCU-related factors, the type of light, irradiance, beam profile, maintenance, and battery charge are the most important [19242526].
During sequential clinical appointments, it is common for clinicians to operate LCUs using battery power, keeping portable devices close to the patient on the instrument table, without constantly charging the battery or even worrying about the battery level of the portable LCUs throughout the day. It is generally assumed that an LCU compensates for power consumption to ensure that the light output remains at the same level; however, without this electronic compensation, the light output would decrease as the battery charge decreases, potentially affecting the polymerization of resin-based materials [26]. A few studies have evaluated the influence of battery charge levels on LCUs’ irradiance and stability, showing that the irradiance of several LED LCUs decreased as the battery was discharged, mainly for “budget” dental curing lights [2526]. Therefore, it is necessary to use devices that offer adequate irradiance regardless of the unit’s battery level. Thus, the aim of the present study was to evaluate the relationship between the battery level and irradiance of 4 different LED LCUs and how these variables can affect the Vickers hardness of a bulk-fill composite resin. The null hypotheses were that there would be no difference in the irradiance of 4 LCUs according to battery level; and that the battery level of the LCUs would not influence the Vickers hardness of a bulk-fill composite resin.
MATERIALS AND METHODS
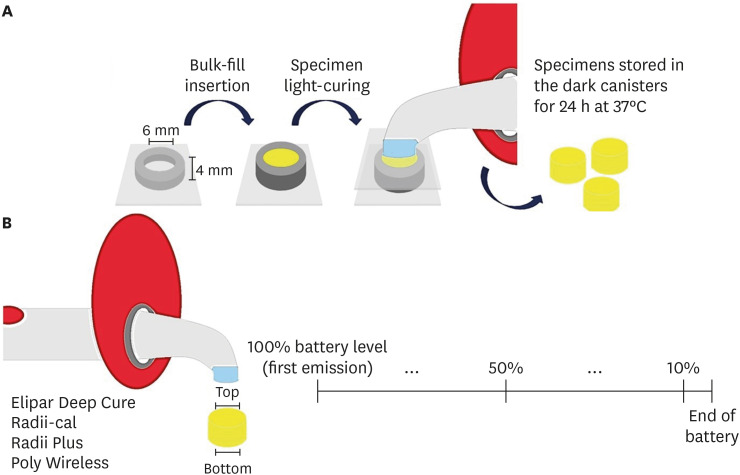
Four new different, fully charged LED LCUs were used in the present study (Table 1). Initially, the light irradiance (mW/cm2) emitted by each fully charged device was measured with the tip in direct contact with the radiometer sensor (Hilux LedMax Hilux, Benlioglu Dental Inc., Ankara, Turkey). Simulating a clinical situation, each LED device was repeatedly used for 20 seconds until the battery was completely discharged, and the irradiance was measured every 10 activations. This procedure was performed 3 times for each device. The light irradiance with the LCUs fully charged and with the battery discharged was determined, as well as the number of irradiations (activations) per charge (20 s/use). The tip diameter of the evaluated LCUs was as follows: Radii Plus and Radii-cal – 10 mm (lens caps); Elipar Deep Cure – 10 mm; and Poly Wireless – 8 mm.
Table 1
Light-emitting diode light-curing unit (LCU) specifications

Disk specimens (n = 10) of a bulk-fill composite resin (Filtek Bulk Fill; 3M Oral Care, St. Paul, MN, USA), shade A1, were made using a cylindrical stainless-steel mold (6 mm in diameter and 4 mm in thickness). The resin was covered with a transparent Mylar strip and a glass slide to remove the excess material. All the LCU tips completely covered the bulk-fill specimens, and the tips were positioned on top of the specimen’s surface. Each specimen was then light-cured with the LCUs fully charged (100% battery level) for 20 seconds and stored in dark canisters for 24 hours at 37ºC. The devices were then used until the battery level decreased by 50%, and other composite resin disk specimens were prepared. The same procedure was repeated when the battery level was at 10% (Figure 1). The battery level measurement was obtained by averaging the number of activations until complete discharge (n = 3). Based on this average number of activations until complete discharge, battery levels of 50% (represented by 50% of the number of activations) and 10% (represented by the remaining 10% number of activations) were determined. To standardize the measurements in the present study, we considered the LCU discharged when the battery level was at 10%.
The Vickers hardness number (VHN) was determined using a hardness tester (HM-210, 810-404A, Mitutoyo Corporation, Kawasaki, Kanagawa, Japan), with a load of 50 g and dwell time of 10 seconds, on the top and bottom surfaces of the resin samples. Three measurements were made per surface, 1 mm from each other for each specimen. The mean VHN and hardness ratio (hardness ratio = hardness of the bottom surface/hardness of the top surface) of the specimens were calculated.
Data analysis was carried out using SigmaPlot 11.0 software (Systat Software Inc., San Jose, CA, USA). The normality and homogeneity of variance of the irradiance and VHN data were evaluated using the Shapiro-Wilk test and Levene test. As the p values were > 0.05, the data were statistically analyzed by parametric tests. Irradiance data with the fully charged and discharged battery were analyzed by repeated-measures 2-way analysis of variance (ANOVA) and the Tukey test. The VHN data were analyzed by 2-way ANOVA, Tukey’s test, and paired t-test. Pearson correlation coefficients were used to determine the significance of correlations between battery level and irradiance, and between battery level and hardness. All analyzes were performed with a significance level of 5% and a power greater than 80%.
RESULTS
The results of the light irradiance of 4 LED LCUs throughout the complete discharge cycle of the battery, as well as the number of activations per charge, are shown in Table 2 and Figure 2. For light irradiance, the results indicated statistically significant differences for the LCUs (p < 0.001), battery charge (fully charged vs. discharged) (p = 0.003) and a double interaction (p < 0.001). Elipar Deep Cure and Poly Wireless showed significant differences in light irradiance when comparing the LCUs with fully charged and discharged batteries. All LCUs evaluated presented significant differences in light irradiance in both conditions (battery fully charged and battery discharged).
Table 2
Irradiances of light-curing unit (LCU) (mean ± standard deviation) according to battery charge and number of activations

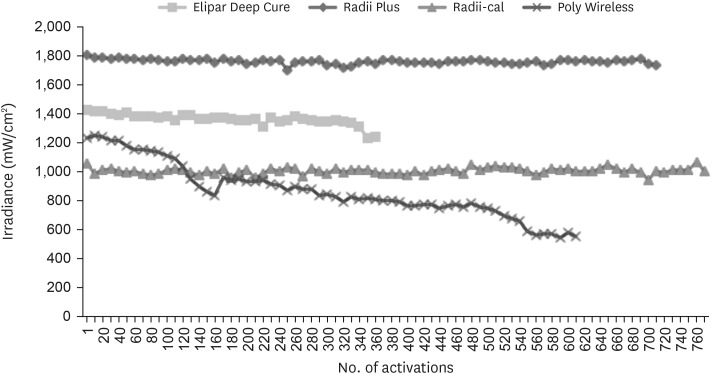
The light irradiance of the Poly Wireless gradually declined from the beginning (baseline irradiance of 1235 mW/cm2) to the end of the battery discharge, reaching a value of 543 mW/cm2 and allowing 610 activations. The Radii Plus presented a first high irradiance reading of 1,805 mW/cm2 with constant irradiance over most of the discharge cycles, reaching an irradiance of 1,771 mW/cm2 at the end of the battery discharge, equivalent to approximately 98% of its initial irradiance. Seven hundred activations were performed with this LCU. Both Elipar Deep Cure and Radii-cal showed irradiance stability throughout the battery discharge, keeping the irradiance above 95% in relation to the initial irradiance (baseline). Elipar Deep Cure allowed 335 activations, while Radii-cal totaled 756 activations.
The results for the VHN on the top and bottom surfaces of the bulk-fill resin are shown in Table 3. For both surfaces, the results indicated statistically significant differences for the LCU (p < 0.001), battery level (p < 0.001), and a double interaction (p < 0.001). On the top surface, there were no significant differences in the VHN for Elipar Deep Cure, regardless of battery level. There were no significant differences in the VHN when the battery level was 100% and 50% in Radii-cal and Radii Plus; however, when the battery dropped to 10%, there was a significant decrease in hardness. For Poly Wireless, significant differences were found in the VHN when the battery level decreased from 100% to 10%. For all battery levels, Elipar Deep Cure showed significantly higher hardness values than Radii-cal. For battery levels of 100% and 50%, the VHN of Radii Plus and Poly Wireless were not significantly different from those of Elipar Deep Cure; however, when the battery level decreased to 10%, Radii Plus and Poly Wireless showed intermediate hardness values.
Table 3
Bulk-fill resin Vickers hardness number (VHN) on the top and bottom surfaces according to the light-curing unit (LCU) and the battery level (100%, 50% and 10%)

At the bottom surfaces, the VHN of the specimens obtained with Radii Plus and Elipar Deep Cure remained constant throughout the battery discharge. For Poly Wireless, the VHN significantly decreased when the battery level dropped from 100% to 50% and 10%, which presented similar hardness. For Radii-cal, the VHN of the specimens significantly decreased with a drop in the battery levels. At all battery levels evaluated, Elipar Deep Cure showed significantly higher hardness values than the other LCUs that were evaluated.
Table 4 presents the bottom-to-top hardness ratios, which were calculated using the hardness data of the top and bottom surfaces. The comparison of the VHN between top and bottom surfaces showed statistically significant differences in all groups, with the exception of Elipar Deep Cure, with battery levels of 100% and 50%. Hardness ratios below 80% were obtained for Radii-cal at a 10% battery level and for Poly Wireless at 50% and 10% battery levels.
Table 4
Bottom/top hardness ratios of bulk-fill resin according to light-curing unit (LCU) and battery level (100%, 50% and 10%)

Moderate positive non-significant correlations were observed between the battery level and hardness at the top (r = 0.443 and p = 0.149) and bottom (r = 0.464 and p = 0.129) surfaces. A strong and positive, but non-significant, correlation was observed between battery level and irradiance (r = 0.990 and p = 0.090).
DISCUSSION
The first null hypothesis, that there would be no difference in the irradiance of the 4 LCUs according to battery level, was rejected. It was observed that there was a significant decrease in irradiance for Elipar Deep Cure and Poly Wireless when the LCUs were compared with their batteries fully charged and discharged; furthermore, for some devices, there was a major relationship between irradiance and battery level.
LCUs emit cold light generated by high-power LEDs, with a narrow emission range in the visible light spectrum (450–490 nm), corresponding to the maximum absorption peak of camphorquinone (468 nm), which is the most common photoinitiator present in resin-based materials [29]. The irradiance of the LCUs at the different battery levels was determined with a radiometer. These devices are often used to measure the irradiance emitted by LCUs, as they are simple and fast, and are widely used to monitor the performance of light sources [3031].
It has been reported that a minimum of 400 mW/cm2 for 40 seconds is required to light-cure a 2 mm layer of composite resin [32]. Considering that current LED curing units are capable of reaching irradiances greater than 800 mW/cm2, this time can be reduced by half [213334]. As in this study, a bulk-fill resin was used and, according to the manufacturer’s recommendations, for LCUs with irradiances of 1000 mW/cm2 or greater, the polymerization time is 20 seconds for increments of 4 mm in thickness. In the assessed LCUs, only Poly Wireless obtained readings below 800 mW/cm2. When the battery was fully charged, it presented irradiance values above 1,200 mW/cm2, whereas the irradiance in the last activations was approximately 500 mW/cm2 (corresponding to about 45% of the initial reading), which could affect the degree of conversion and the mechanical of the resin-based materials [35].
As for the irradiance of the other evaluated LCUs, Radii-cal, Radii Plus, and Elipar Deep Cure showed constant readings of irradiance. Radii Plus and Elipar Deep Cure had the highest readings (1,085 mW/cm2 and 1,429 mW/cm2, respectively), and Radii-cal showed an irradiance of 1,056 mW/cm2. In contrast, the LCUs that had the longest battery life were Radii-cal, followed by Radii Plus and Poly Wireless. Radii-cal and Radii Plus obtained an average of 756 and 700 activations with little variation in irradiance, while Poly Wireless allowed an average of 610 activations with a decrease in irradiance of more than 50% compared to the initial reading. Elipar Deep Cure, on the other hand, allowed an average of 335 activations, which corresponds to less than half of the battery life of the other LCUs analyzed, but with constant light emission. The battery level influenced the irradiance for Poly Wireless more strongly than for the other LCUs. The irradiance started to decrease with the use of the LCU’s battery; this may occur due to the production of a varied voltage line, which affects the stability of the emitted light [36].
The second null hypothesis, that the battery level of the LCUs would not influence the VHN of a bulk-fill composite resin, was also rejected. Bulk-fill composite resins have been used for posterior restorations and can be placed in increments of 4 to 6 mm without having to increase the light-curing time [3]. In addition, bulk-fill composites present higher degree of conversion and lower polymerization shrinkage and contraction stress than conventional composites [12343738]. The depth of cure and degree of conversion, as well as the final physical and mechanical properties of the composite resins, are factors that define clinical success of resin-based direct restorations. Another important factor is the quantity of light transmittance, as well as the attenuation of light throughout the composite resin thickness [10]. This study demonstrated that the bottom surface of the specimens had significantly lower hardness values than the top surface, regardless of the LCU used and the battery level. A greater thickness of the increment is associated with a lower degree of conversion and hardness of the material in deep areas [39]. A hardness ratio of at least 80% between the top and bottom surfaces is considered high [40414243]. In the present study, significant differences were observed between the VHN of the top and bottom surfaces of the specimens in most of the groups; however, despite the significant difference, the hardness ratio was lower than 80% only in 3 of the 12 groups defined by a combination of LCU and battery level, indicating an adequate depth of cure and polymerization.
Although Radii Plus, Radii-cal, and Elipar Deep Cure presented stable irradiance during the discharge of the battery, only Elipar Deep Cure and Radii Plus presented hardness values with little variation for the battery levels evaluated. For Radii-cal, a slight decrease in the hardness values was observed when the battery level was at 10%. Elipar Deep Cure obtained the highest hardness values on the top and bottom surfaces, and also for hardness ratio, which remained above 90% throughout the battery discharge. Radii Plus also showed an adequate effectiveness of cure, with average hardness ratios above 80% for all battery levels. Radii-cal showed a hardness decrease between the top and bottom surfaces of the specimens, with ratios above 80% for battery levels of 100% and 50%. At a 10% battery level, the hardness ratio decreased to 77%. In contrast, the hardness ratio for Poly Wireless was below 80% in half of the discharge cycle, obtaining higher values only when the battery was fully charged.
It is important to keep in mind that these results should be interpreted with caution in clinical situations. In the study, the tip of the LCUs was placed directly in contact with the composite resin and kept perpendicular to the surface of the material, allowing standardization of the distance (0 mm) and positioning (inclination) of the tip. Thus, the light attenuation that occurs when the tip is positioned at different angles was minimized [44]. However, it has been demonstrated that the final properties of bulk-fill resins are only slightly influenced by the loss of light resulting from errors in the positioning and angulation of the light source [4].
Finally, the choice of a LED curing unit with stable light emission and monitoring of the irradiance during the unit’s battery discharge and lifetime contributes to obtaining adequate clinical results in the long-term when using light-cured composites. Periodically checking the irradiance of the LCUs is important, since some devices available lose power in light emission during their lifetime of use; therefore, it would be necessary to monitor devices periodically and replace them as soon as necessary.
Periodically checking the irradiance of LCUs during office hours and their service life is vital for clinical practice. In addition to achieving good results in clinical procedures, clinicians can identify possible decreases in irradiance and place the cordless devices on the charging stand regularly, maintaining the battery fully charged throughout the day. Periodic irradiance checks would also allow monitoring of LCUs’ performance during their service life and help identify when device maintenance or replacement is necessary.
CONCLUSIONS
It can be concluded that although the irradiance was different among LCUs, it decreased in half of the devices along with a reduction in battery level. In addition, the bulk-fill composite resin effectiveness of curing, measured by the hardness ratio, was reduced when the LCU’s battery was discharged.
 XML Download
XML Download