

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Dental resorption is a challenge in diagnosis and treatment planning for dentists due to the complexity of the process, and it can lead to complex dental treatments or even extraction [12]. Root resorption is classified in relation to the affected root surface as external or internal [2345]. One of the subtypes of external root resorption is external cervical resorption (ECR). As its name indicates, ECR occurs itself in the cervical aspect of the tooth, initiating in the external aspect of the root cementum [26]. As it progresses, the resorption extends around the pulp canal in an apico-coronal and circumferential direction, destroying dentin, cementum, and enamel due to its aggressive nature [5]. The loss of dental root tissue from teeth affected by ECR was found to reach 58% in the most advanced cases [6]. If the diagnosis is made in the early stages of resorption, the prognosis for the tooth is better, since the amount of remaining intact tooth structure has a significant influence on the prognosis [7].
Even though the exact etiology of ECR remains unclear, it has been associated with trauma, orthodontics, surgery, periodontal therapy, occlusal dysfunction, and intracoronal bleaching [238]. The literature indicates that ECR can be multifactorial since more than 1 predisposing factor is identified in many cases [9]. It can be speculated that all clinical procedures that can cause damage to the cementum, compression of the periodontal ligament, hypoxia and chronic irritation at the root can be initial causes of the development of ECR.
In 1999, Heithersay [10] proposed a classification of ECR into 4 classes based on severity. According to this classification, lesions can vary from class 1 to class 4, with the first stage corresponding to a small and shallow defect close to the cervical region of the tooth, and the most advanced stage to a large defect that extends beyond the coronal third of the root. This classification provides important information to professionals and researchers concerning ECR extension, even though it is based on the 2-dimensional (2D) radiographic presentation [5].
Currently, cone-beam computed tomography (CBCT) is widely used in dentistry. In ECR cases, it enables a detailed assessment of ECR and its geometric proportions within the tooth without overlapping structures or geometric distortion. CBCT allows a correct visualization of the resorption defect, as well as accurate observations of the lesion’s entry point and its correct stage of progression, which help the professional to establish the treatment plan. Some studies that have compared the diagnostic effectiveness between sets of periapical radiographs with dissociation of images and CBCT have shown that the analysis using CBCT was significantly better than the analysis using 2D images [35811]. In 2018, Patel et al. [12] developed a new classification that was based on 3D aspects of ECR. This new classification takes into account the ECR height, circumferential spread, and proximity to the root canal. Therefore, it seems to provide a more accurate assessment of the preoperative condition of ECR than the Heithersay classification when 3D examinations are used, and may help improve clinicians’ treatment planning and management of lesions [13]. To the best of our knowledge, only 1 study has evaluated ECR cases based on a 3D classification proposed by Jebril et al. [14].
Furthermore, few studies have evaluated the prevalence and characteristics of ECR [46915]. Those studies showed prevalence from 0.08% to 2.3% and reported that maxillary anterior teeth were more frequently affected, with no predilection for patients’ age and sex [46915]. Nevertheless, the actual prevalence and predilection of ECR according to sex and age remain unclear, since the studies did not report the total population evaluated or the data considering the total population. Instead, they analyzed only data from ECR cases, so their results consist of the sex and age distribution among ECR cases. Due to the importance of knowing the prevalence and characteristics of ECR so that professionals can make an early diagnosis and because these factors can vary among different populations, the aim of this study was to assess the prevalence and characteristics of ECR regarding sex, age, tooth, degree, and portal of entry in a Brazilian subpopulation using CBCT scans.
Go to : 
MATERIALS AND METHODS
Study sample
This cross-sectional observational study followed the STROBE checklist and was started after approval by the Institutional Research Ethics Committee of the Piracicaba Dental School, University of Campinas (UNICAMP, protocol #4.086.759).
CBCT scans from a database of a private clinic that were requested for endodontic reasons from September 2018 to February 2020 were evaluated. First, 2,789 scans were selected and the following exclusion criteria were applied: scans performed using low-resolution protocols, scans that had movement artifacts, and/or scans that had teeth with root fractures. After applying the exclusion criteria, 1,313 scans were used in the present study (Figure 1), 883 of which were from female patients and 430 from male patients, with a mean age of 55.2 years. The scans were acquired using a PreXion 3D (Terarecon, San Mateo, CA, USA) CBCT unit with a high-resolution protocol (90 kVp, 4 mA, field of view [FOV] 5 × 5 cm, 0.1 mm voxel resolution, and 360º scan). All permanent teeth included in the FOV were analyzed.
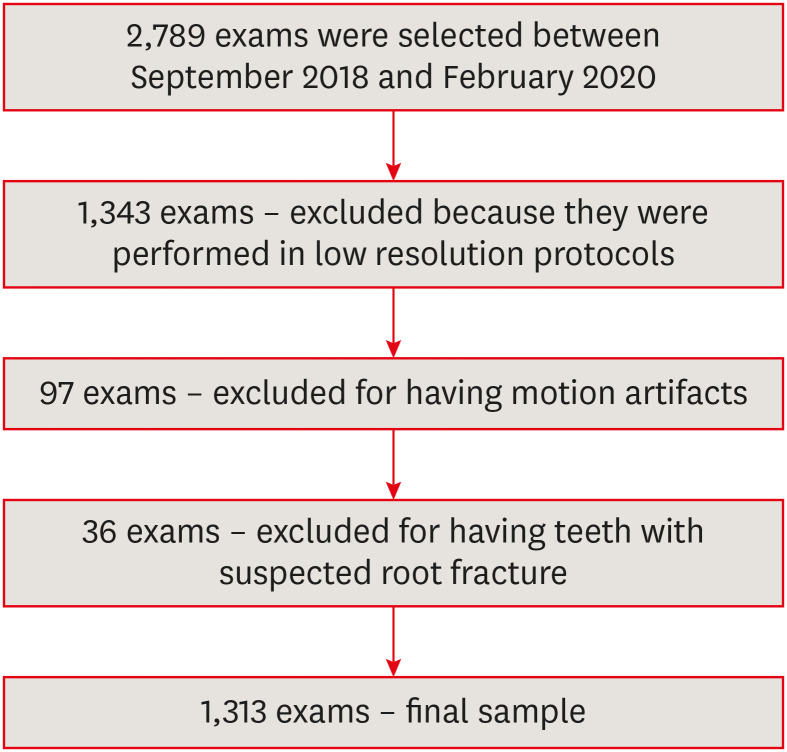
Image assessment
1. Prevalence of ECR
The 1,313 CBCT scans were evaluated to diagnose ECR by one oral radiologist, with 5 years of experience and blinded regarding the characteristics of the sample, in a dimmed-light room using the RadiAnt DICOM viewer software (Medixant, Poznan, Poland). The assessment was conducted using multiplanar reconstruction and the use of enhancement tools, such as brightness, contrast, and zoom, was allowed. All teeth included in the FOV were analyzed. An ECR lesion was considered to be a predominantly hypodense image with diffuse margins, which started from cervical aspect of the tooth and could extend from the crown to the apical third of the root of the affected tooth. Lesions with those characteristics showing hyperdense calcified areas were also considered ECR since a mottled or cloudy appearance can occur as a result of ossification in the “reparative” phase [2]. For each tooth that could be evaluated, the sex and age of the patient were recorded. In addition, the evaluator indicated whether ECR was present or absent for each tooth. In cases of initial ECR, the evaluator excluded the possibility of caries by observing the limits of the lesion and the periodontal status. Thirty days after the completion of the evaluation, a reassessment of 10% of the sample (randomly selected) was performed to assess intra-observer agreement.
2. Characterization of the cases
Subsequently, the scans with the presence of ECR were assessed under the same conditions and software used in the first step to characterize the cases. The cases were classified according to the 3D classification [12] (Figure 2). The height of the lesions was scored as (1) supracrestal, if it was located above the bone crest; (2) subcrestal, if it extended into the coronal third of the radicular dentin; (3) extending into the middle third of the radicular dentin; or (4) extending into the apical third of the radicular dentin. The circumference of the lesions was rated as smaller than 90o (A), between 90o and 180o (B), between 180o and 270o (C), or greater than 270o (D), considering the 360° extent of the root in the axial plane. The proximity of the lesions to the root canal was graded as within the dentin (d) or showing pulp involvement (p). To evaluate the height of the lesion, sagittal and coronal CBCT views were used. To evaluate lesion circumference and proximity to the root canal, the axial CBCT view corresponding to the largest dimension of ECR was used.
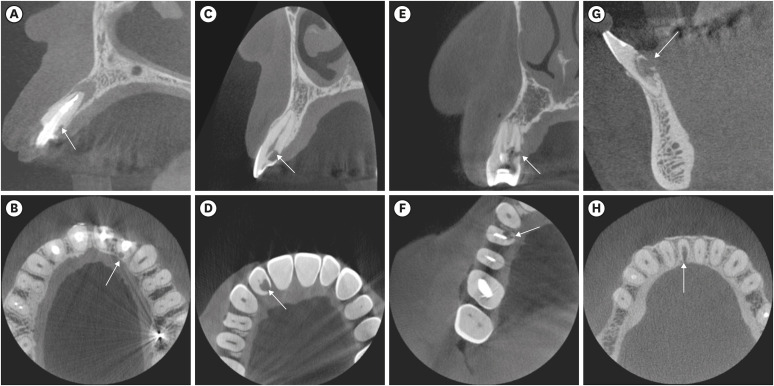
The ECR cases were also evaluated regarding the portal of entry (buccal, lingual/palatal, or proximal) (Figure 3).

Fifteen days after the completion of the evaluation, a reassessment of 20% of the sample (randomly selected) was executed under the same conditions to assess intra-observer agreement.
3. Statistical analysis
The statistical analysis was performed using SPSS version 23.0 (IBM Corp., Armonk, NY, USA). The prevalence and characteristics of ECR were described as frequencies and percentages. Intra-observer agreement was analyzed using the kappa test and interpreted based on Landis and Koch [16]. The level of significance adopted was 5%. The null hypothesis was that there would be no association between the presence of ECR and the factors studied. A power analysis was conducted considering the sample size and the prevalence of ECR for the analysis of the prevalence; and the χ2 value and the degrees of freedom for the χ2 test. All analyses achieved a statistical power of 85%.
Go to :
RESULTS
A total of 6,240 teeth were analyzed. The demographic distribution of the sample according to sex, age, and tooth is summarized in Table 1. Of those, 84 teeth (1.35%) were diagnosed as being affected by ECR, out of which 40 (47.62%) teeth were in male patients, whereas 44 (52.38%) were in female patients (Table 2).
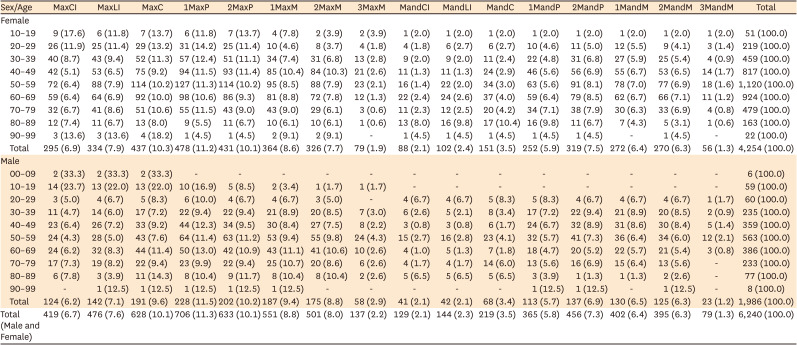
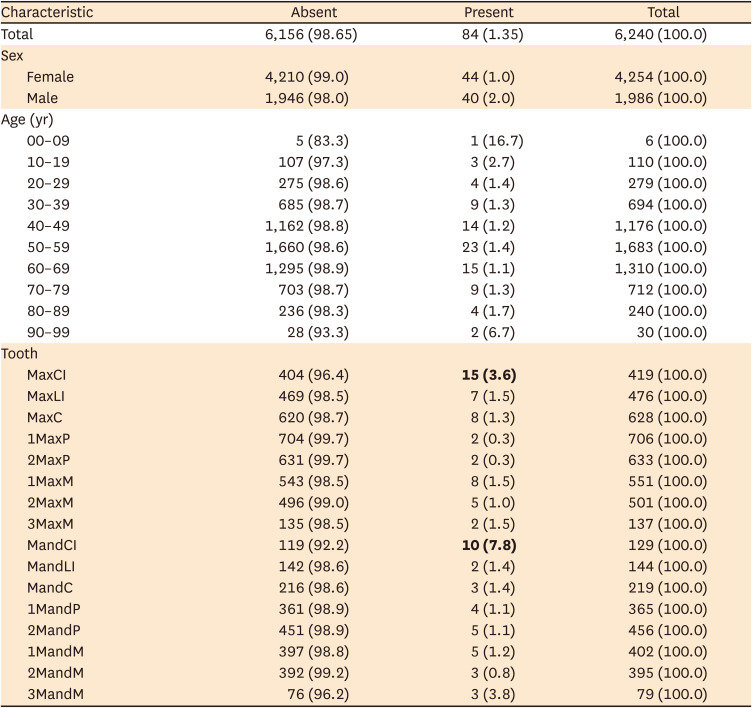
Table 1
Characterization of the sample acquired by high-resolution cone-beam computed tomography according to teeth, sex and age
Values are presented as number (%).
MaxCI, maxillary central incisor; MaxLI, maxillary lateral incisor; MaxC, maxillary canine; 1MaxP, first maxillary premolar; 2MaxP, second maxillary premolar; 1MaxM, first maxillary molar; 2MaxM, second maxillary molar; 3MaxM, third maxillary molar; MandCI, mandibular central incisor; MandLI, mandibular lateral incisor; MandC, mandibular canine; 1MandP, first mandibular premolar; 2MandP, second mandibular premolar; 1 MandM, first mandibular molar; 2 MandM, second mandibular molar; 3 MandM, third mandibular molar.
![]()
Table 2
Distribution of the presence and absence of external cervical resorption according to sex, age, and affected tooth
Values are presented as number (%). p = 0.002 for sex, p = 0.122 for age, and p < 0.001 for tooth, according to the χ2 test. Bold numbers indicate significant difference from the others.
MaxCI, maxillary central incisor; MaxLI, maxillary lateral incisor; MaxC, maxillary canine; 1MaxP, first maxillary premolar; 2MaxP, second maxillary premolar; 1MaxM, first maxillary molar; 2MaxM, second maxillary molar; 3MaxM, third maxillary molar; MandCI, mandibular central incisor; MandLI, mandibular lateral incisor; MandC, mandibular canine; 1MandP, first mandibular premolar; 2MandP, second mandibular premolar; 1 MandM, first mandibular molar; 2 MandM, second mandibular molar; 3 MandM, third mandibular molar.
![]()
Table 2 shows the distribution of the presence and absence of ECR according to sex, age and affected tooth. Of 1,986 male patients, 2.0% had ECR, while of 4,254 female patients, 1.0% had ECR. A significant association between the presence of ECR and sex, with a higher prevalence in males than in females according to the χ2 test (p = 0.002). There was no significant association between the presence of ECR and age (p = 0.147).
Of the teeth with ECR, 17.8% were maxillary central incisors and 11.9% were mandibular central incisors. Considering the prevalence within each tooth, the most commonly affected teeth were the mandibular central incisors (7.8%) followed by the maxillary central incisors (3.6%) (Table 2). Those teeth were more frequently affected by ECR than the others, and the type of tooth was significantly associated with the presence of ECR (p < 0.001). The less commonly affected teeth were the maxillary premolars.
For the portal of entry, 44% of the cases were on the proximal surface, whereas 40.5% were on the lingual/palatal surface, and 15.5% were on the buccal surfaces (Table 3). The portal of entry did not show an association with the type of tooth (p = 0.296).
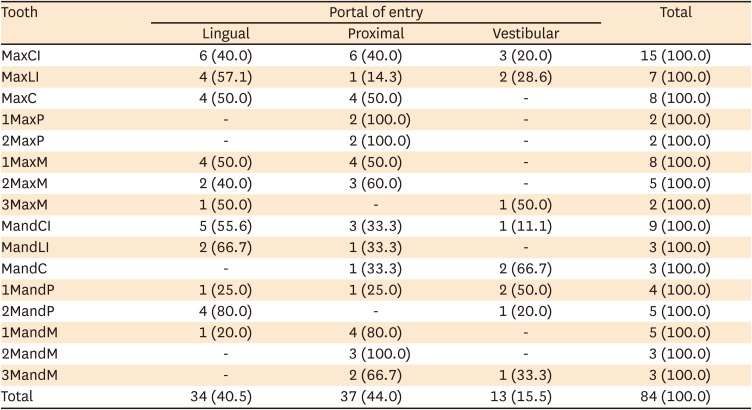
Table 3
Distribution of external cervical resorption according to the tooth and portal of entry
Values are presented as number (%). p = 0.296, according to the χ2 test.
MaxCI, maxillary central incisor; MaxLI, maxillary lateral incisor; MaxC, maxillary canine; 1MaxP, first maxillary premolar; 2MaxP, second maxillary premolar; 1MaxM, first maxillary molar; 2MaxM, second maxillary molar; 3MaxM, third maxillary molar; MandCI, mandibular central incisor; MandLI, mandibular lateral incisor; MandC, mandibular canine; 1MandP, first mandibular premolar; 2MandP, second mandibular premolar; 1 MandM, first mandibular molar; 2 MandM, second mandibular molar; 3 MandM, third mandibular molar.
![]()
The sample distribution according to the 3D classification, tooth type, and port of entry is exhibited in Table 4. The classification 4Dp was the most frequently found with 15 cases, followed by the classification 3Bp, with 12 cases. The least commonly found classifications were 1Ad, 1Bd, 1Bp, and 3Dp, with 1 case each. Considering only the height of the lesion, height 3 (mid-third of the root) was the most frequently found.
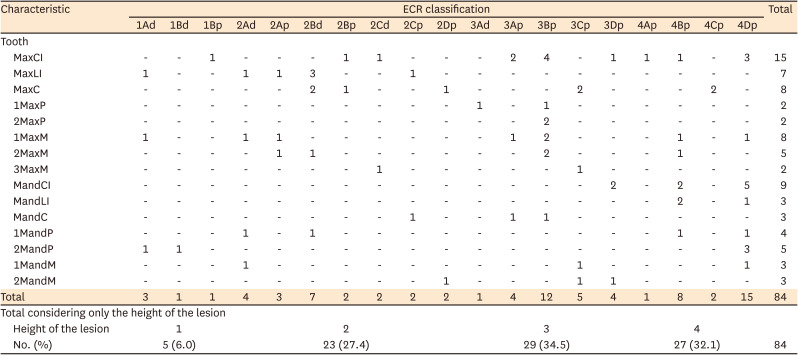
Table 4
Distribution of the 3-dimensional classification of external cervical resorption (ECR) according to the tooth
MaxCI, maxillary central incisor; MaxLI, maxillary lateral incisor; MaxC, maxillary canine; 1MaxP, first maxillary premolar; 2MaxP, second maxillary premolar; 1MaxM, first maxillary molar; 2MaxM, second maxillary molar; 3MaxM, third maxillary molar; MandCI, mandibular central incisor; MandLI, mandibular lateral incisor; MandC, mandibular canine; 1MandP, first mandibular premolar; 2MandP, second mandibular premolar; 1 MandM, first mandibular molar; 2 MandM, second mandibular molar; 3 MandM, third mandibular molar.
![]()
The intra-observer agreement was excellent for the diagnosis of ECR, portal of entry, and 3D classification (kappa = 1.0, 0.907, and 1.0, respectively).
Go to :
DISCUSSION
The prognosis and management of teeth affected by ECR are influenced significantly by the stage of progression; therefore, early diagnosis should be achieved. Since CBCT was introduced and entered into widespread use in dentistry, the authors of the present study had the impression that the prevalence of ECR had increased [17]. Assuming that the cause of such an impression was probably the ability to evaluate teeth in all their aspects in 3D examinations, the authors researched the literature to find reports of the prevalence of ECR using CBCT for diagnosis in order to better understand its actual aspects. To our surprise, we found few studies that evaluated the prevalence of ECR, with reported prevalence rates ranging from 0.08% to 2.3% [46]. However, those previous studies did not detail the sample regarding the number of CBCT scans, the teeth evaluated, or patients’ demographic data because their aim was to evaluate the characteristics of ECR rather than its prevalence. Therefore, we conducted an epidemiological study with a robust sample, constituting 1,313 CBCT scans in which 6,240 teeth were retrospectively analyzed, and found a prevalence of ECR of 1.35%. This prevalence is in accordance with the reports of 2 previous studies, although the details of the present study and the previous ones are different [57].
This epidemiological study showed that ECR has a wide age distribution and is more prevalent in male patients (2.0%). Because traumatic injuries are a possible cause for the development of resorption, the higher prevalence in males could be attributed to more aggressive contact sports and activities of males in comparison with females [910]. Previous studies have shown higher proportions in female patients [491015]. However, there is an important difference in the methodology used in these previous studies, in which only affected teeth were evaluated. Therefore, their study design allowed a comparison to be made between the proportion of male and female patients with ECR instead of the prevalence within each sex. The fact that those studies did not report the total of men and women evaluated precludes an understanding of the predilection of ECR by sex, as was demonstrated by the present results.
The majority of patients that had teeth affected by ECR were between 40 and 69 years old; however, the sample also had more CBCT scans in these age groups, so none of the age groups had a significantly higher prevalence than the others. Two recent studies found an average age similar to our study [515]. Conversely, most of the patients in the study by Mavridou et al. [9] were between 15 and 54 years old, and in Heithersay’s study [10] the patients were between 20 and 50 years old. This age difference may be due to the age range and distribution of the sample studied [910]. Another difference between the present study and these 2 previous studies is the population studied. In the present study, only patients from a Brazilian subpopulation were evaluated. Because the causes of ECR seem to encompass factors associated with population characteristics and habits, such as occlusal dysfunction, orthodontics, periodontal therapy, surgery and intracoronal bleaching, future studies considering other populations and using the 3D classification are encouraged.
A recent study found the highest prevalence of ECR in upper incisors, where the central and lateral incisors were considered as a single group [5]. In our findings, we did not group teeth, because we instead aimed to determine the actual prevalence of ECR for each tooth, and found the most affected teeth were the mandibular central incisors, followed by the maxillary central incisors. The higher prevalence in anterior teeth corroborates other studies [491015]. This characteristic may be related to the likely predisposition of factors that promote resorption, such as traumatic injuries and orthodontic or bleaching procedures, taking place in anterior teeth. It is also important to note that upper canines were affected by ECR in several cases. These teeth undergo a lot of torque movement during orthodontic treatment, which is concentrated in the cervical region and may damage this region, stimulating the development of ECR. Still, the results for first and second maxillary molars (prevalence of 13 cases or 0.7% of 1,849 teeth evaluated) agree with those found by Thönen et al. [18], who evaluated 858 maxillary first and second molars and found a low mid-term occurrence (0.9%). As previously discussed, the main difference between the present study and all other prevalence studies is the sample; the previous studies only included teeth that had resorption and described the distribution of ECR regarding sex, age, and tooth group, which makes some comparisons difficult.
Heithersay, in 1999 [10], devised a classification to categorize ECR according to its size and depth into the root canal. The classification is based on 2D radiographs and categorizes ECR according to the penetration of the lesion into the dentin. With the advent of CBCT, other characteristics of ECR could be evaluated, but they are not included in the Heithersay classification. Because 3D examinations were used in the present study, a 3D classification was adopted to evaluate resorption in a complete way and reach the actual extension of the resorptive process, which dictates the clinical manifestations of the lesion. The use of CBCT in suspected ECR cases is supported by the findings of previous studies, which showed that CBCT was more accurate for scoring ECR than parallax periapical radiographs [311]. This is also in accordance with the European Society of Endodontology 2014 position and the American Association of Endodontists and the American Academy of Oral and Maxillofacial Radiology 2015 position about the use of CBCT in endodontics, which stated that limited-FOV CBCT should be the imaging modality of choice to evaluate resorptive defects and determine appropriate treatment and prognosis [19]. Therefore, CBCT has been the most recommended and accurate examination for ECR diagnosis and evaluation [42021].
Taking into account the lesion height and circumferential spread, the most frequent classification in the present study was 3 (mid-third of the root) and more than 180°, respectively. Although Matny et al. [5], in 2020, did not use the 3D classification, strictly speaking, because the authors also used 2D radiographs, they classified the sample according to the height and circumferential spread in 3D examinations. It was found that most cases had reabsorption extending to the middle and apical thirds of the root and affecting more than 180° of the root, which corroborates our findings. In 2020, Jebril et al. [14] analyzed an ECR sample using the 3D classification and found a greater quantity (3 teeth) with the 2Bp classification. However, that study used a limited sample of 14 teeth. Because the clinical decision on the treatment plan and prognosis depends on the extent of the resorptive defect, class 4 of the Heithersay classification and height degree 4 of the 3D classification, which was the second more prevalent degree in the present study, suggest that the progress should be monitored until extraction of the tooth becomes inevitable as any interventionist approach is discouraged. According to Matny et al. [5], even in lesions classified as classes 1 or 2, the extent of the resorptive defect can reach 28% of the root surface, and lesions classified as class 4 reaches up to 58% loss of root structure. This point reinforces that an early diagnosis is essential for effective management and better prognosis, since an earlier diagnosis means that a greater percentage of healthy dental tissue is preserved, thereby increasing the chances of successful treatment.
The portal of entry is the initiation point of resorption and, for ECR to be initiated, the cementum and periodontal ligament should be damaged or absent [22]. Its evaluation is of importance to the treatment plan. In our study, most ECRs were located at the proximal or lingual/palatal surfaces. Matny et al. [5] found a prevalence of 42% at the lingual/palatal portal of the entry surface, which is very similar to our results. Resorptive defects initiated on the lingual/palatal surface are considered difficult to access and therefore might not be possible to treat [5].
The percentage of re-sampling used to evaluate intra-examiner agreement was different in the 2 steps of the study (10% for the prevalence of ECR and 20% for the characterization of ECR) due to the difference in the samples. Since 6,240 teeth were used to study the prevalence of ECR and 10% of them constituted a sufficient re-sampling to analyze intra-examiner agreement, the authors did not utilize higher percentages. Instead, since only 84 teeth were analyzed to characterize ECR, a higher percentage was required in the re-evaluation to perform the analysis.
One of the limitations of the present study was to be based only on CBCT images, since clinical information of the patients was not available, which also precluded being able to relate the ECR to predisposing factors. Mavridou et al. [9], in 2017, found a series of conditions that could be related to ECR lesions, including orthodontic treatment, trauma, parafunctional habits, poor oral health, malocclusion, and extraction of a neighboring tooth and concluded that multiple predisposing factors were identified in the majority of cases, indicating that ECR may be mainly multifactorial. The early stages of ECR lesions can sometimes be confused with caries lesions [212]. Because the patients’ clinical information was not available in this study, the differentiation between ECR and caries lesions was made only based on images, which could be considered another limitation. However, ECR differs from caries lesions since the ECR contour is slightly irregular [6]. The authors also believe that the fact that they analyzed 3D examinations helped in the differentiation; therefore, they had no doubts regarding the cases that were diagnosed as ECR in the present study.
Finally, it is important to note that ECR is predominantly hypodense due to its resorptive nature; however, it may show hyperdense areas in the reparative phase as a result of ossification of granulomatous tissue [2]. For this reason, both appearances were considered in the present study for the diagnosis of ECR.
Go to :
CONCLUSIONS
The prevalence of ECR was 1.35% in the sample studied. Other important findings were that ECR had a higher prevalence in male patients, there were no age predilection, mandibular and maxillary central incisors were the most commonly affected teeth, extension into the mid-third of the root (height 3 of the 3D classification) was the most frequent stage found, and proximal and lingual/palatal surfaces were the most frequent portals of entry. These findings enable professionals to better understand these aspects of ECR and reinforce the importance of an imaging evaluation for the early detection of ECR lesions.
Go to :
 XML Download
XML Download