

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
In the early coronavirus disease 2019 (COVID-19) pandemic, the social demand for the early development of vaccines and rapid vaccination was strong due to severe fear of the disease and awareness of the crisis. However, the general public tended to be reluctant to vaccinate as the clinical course of COVID-19 became more familiar, the fatality rate decreased, and some vaccination side effects were known. Furthermore, opinions against the guidelines of policy officials or healthcare workers promoting large-scale vaccinations have increased. Several factors related to vaccine hesitancy among the general public have already been reported, such as misinformation about the COVID-19 vaccine, fear of side effects, and concerns about exacerbating underlying health conditions.123
Although COVID-19 vaccines have reduced the number of deaths and hospitalized patients worldwide, the general public’s hesitation to receive vaccination is a major impediment to dealing with this new infectious disease. The confidence of the general public and medical workers in the vaccine is essential for responding to new infectious diseases, such as COVID-19; therefore, many investigations are underway.45
It is important to educate healthcare personnel for they can communicate well with the general public, who are hesitant to get vaccinated.6 In addition, several studies have pointed out that the emotional support and communication of healthcare personnel for those who are considering vaccination are important components; however, they remain insufficient.678 In addition to the traditional relationship between doctors and patients, the importance of online communication technology in acquring vaccine-related information and promoting large-scale vaccination cannot be ignored.9
The severe acute respirarory syndrome (SARS) and Middle East respiratory syndrome (MERS) outbreaks ended before the development of vaccines for each disease; vaccine development for Ebola disease progressed relatively slowly over several years, while COVID-19 spread rapidly worldwide and the vaccine development process for COVID-19 progressed quicker compared to the previous vaccine development for new infectious diseases.101112 In the past, it took decades to develop a vaccine after the causative agent of infectious diseases was identified; however, in COVID-19, vaccines were expeditiously developed and approved for emergency use within a year after the causative virus was identified.12
Although the fields of immunology and vaccinology have developed remarkably, the problem of vaccine hesitancy during the COVID-19 pandemic has become more obvious. During the sudden COVID-19 pandemic, misinformation was believed to have affected the public and even healthcare workers without sufficient prior research and training preparations.678
Therefore, this study aimed to prepare and establish vaccine strategies and vaccination education plans for new infectious diseases that may occur in the future.
VACCINE DEVELOPMENT STRATEGIES IN THE FUTURE
Rapid COVID-19 vaccine development and confidence in the public
The rapid development of COVID-19 vaccines within a year after the identification of the causative virus was made possible by performing basic research, experience gained from other vaccines, development of innovative vaccine platforms, and activities of the Coalition for Epidemic Preparedness Innovations (CEPI).1112
During the COVID-19 pandemic, messenger ribonucleic acid (mRNA) vaccines have been commercialized. In Korea, mRNA, adenoviral vector, and recombinant vaccines have been approved. However, adverse effects, such as myocarditis and pericarditis, have become one of the factors that make COVID-19 vaccination reluctant, especially in young people.13 The rapid introduction of novel COVID-19 vaccines could prevent the collapse of the healthcare system and reduce deaths; however, the evaluation of the adverse effects of new vaccines before use is inevitably insufficient.
Although novel vaccines have benefits, rare serious adverse effects and breakthrough infections have reduced public confidence in new vaccines.13 Furthermore, emergency use authorization of new vaccines and large-scale vaccinations nationwide have reduced public confidence in new vaccines as resistance from those who do not want to be vaccinated and serious adverse effects have been reported; therefore, reflection and re-evaluation of these are important tasks to deal with new infectious diseases that could pose a threat to us in the future.
Organization should be prepared to develop vaccines against emerging infectious diseases effectively
To immediately develop vaccines for new infectious diseases, further development of basic research on the immunologic response against infectious diseases, sequencing techniques in sequencing, recombinant genetic engineering, nucleic acid vaccines, and structure-based vaccine design is required.12 It is necessary to combine existing experience in vaccine development for other pathogens with the development of emerging infectious disease vaccines.101112 Therefore, regardless of success or failure rate, the data storage, evaluation, and analysis of the vaccine development process for COVID-19 are considered important bases for future vaccine development against emerging infectious diseases. In addition to global coalitions, such as CEPI that finance and coordinate the development of new vaccines, it will also be necessary to create an organization that oversees and plans various processes, including basic research, development, clinical studies, distribution, education, and vaccination at the national level. It is vital for vaccine production companies, academic researchers, and state institutions to cooperate and converge to respond well to newly emerging infectious diseases. Moreover, organization should include social and psychological professionals who can represent and address public confidence in presenting new vaccines. To overcome new infectious diseases, continuous community participation and public trust in vaccination, proactive communication on vaccination, presentation of scientific evidence, and promotion are required.1415
Securing the safety of vaccines and establishing measures to strengthen communication with the general public during public health emergencies
Enhancing the safety of the newly developed vaccine and strengthening bilateral communication through scientific knowledge delivery to secure public trust in the vaccine are important goals to pursue in the face of an infectious disease crisis that requires large-scale vaccination.121617 In establishing or developing strategies for vaccine development, we should anticipate and prepare for safety concerns or possible adverse effects, improve the ability to assess the association between vaccines and adverse effects, and enhance the collaboration of vaccine safety activities.1617 Therefore, conducting large-scale national studies on the adverse effects of vaccination and disclosing the results and information will contribute to increasing public trust in vaccine development and vaccination processes. For example, we should conduct national preemptive surveillance studies on serious neurological or cardiovascular side effects that lead to death, life-threatening conditions, serious disability, or require long-term hospitalization to immediately share accurate information with the public and compare it with previously known vaccine side effects. In addition, efforts are needed to continuously identify and inform the public about the changes in vaccine-related information.1819202122 Thus, preparations for the promotion and education of vaccine-related information, which can be pushed back relative to priority compared with basic research and clinical studies, will be systematically planned and prepared before the pandemic occurs.
Decrease in COVID-19 booster vaccination rates compared to COVID-19 primary vaccination rates in South Korea
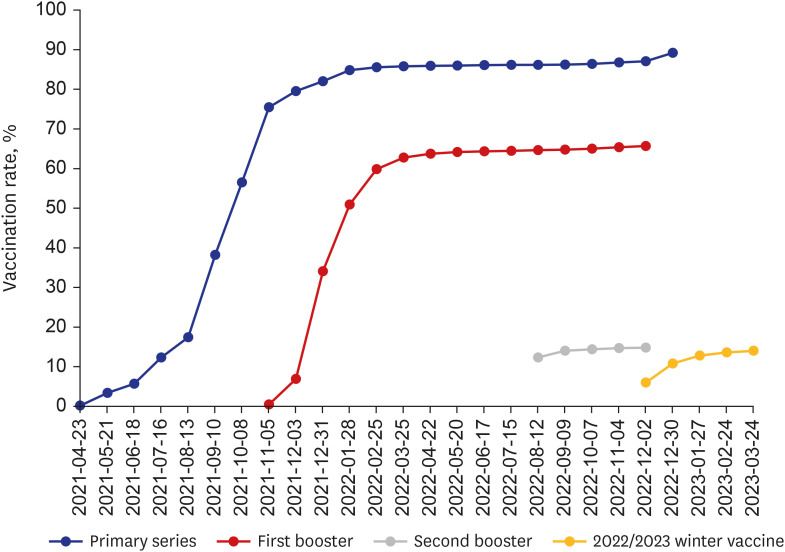
As of September 2022, nearly 86% of South Koreans completed their COVID-19 primary vaccination regimens, including both the first and second doses. However, as of December 9, 2022, only 65.7% and 14.8% of South Koreans had received the first and second COVID-19 booster doses, respectively. The vaccination rate for winter vaccines in the 2022/2023 season including bivalent Omicron-containing COVID-19 vaccines, which began for the high-risk groups in October 2022, was confirmed to be approximately 14.0% at the end of March 2023 (Fig. 1).2324
Fig. 1
Trends in cumulative COVID-19 vaccination rate in Korea. The blue line represents the cumulative percentage of the primary series of COVID-19 vaccination. The red and grey lines represent the rates of the first and second booster vaccinations, respectively. The yellow line represents vaccination rate for winter vaccines in the 2022/2023 season including bivalent Omicron-containing COVID-19 vaccines. Data obtained from Korea Disease Control and Prevention Agency.
COVID-19 = coronavirus disease 2019.
Various factors can be considered for the low rate of COVID-19 booster vaccination in South Korea. Compared to the early days of the COVID-19 pandemic, most South Koreans have already received the primary COVID-19 vaccine series, and fear of COVID-19 has decreased as they or their families or acquaintances have been diagnosed with COVID-19. In addition, some studies have reported a tendency to be reluctant to get vaccinated as fears of progression to severe diseases or deaths from COVID-19 decrease and concerns about side effects of COVID-19 vaccines increase, and this change in perception can be considered a factor for the decreased rate of COVID-19 booster vaccination.25262728
When preparing for countermeasures against emerging infectious diseases in the future, it will be necessary to analyze factors responsible for the drop in COVID-19 booster vaccination rates and find ways to improve them.
SURVEYS ON COVID-19 VACCINE HESITANCY AND LESSONS FOR OTHER EMERGING INFECTIOUS DISEASE CRISES
It is important to understand and respond to the general public’s vaccine avoidance factors, especially investigating vaccine avoidance factors of healthcare workers, who have a strong influence on patient decisions in the process of planning large-scale vaccinations for newly emerging infectious diseases.2930313233343536
Factors associated with COVID-19 vaccine hesitancy
The survey findings and results of vaccine refusal or hesitation factors are summarized in Table 1. In a cross-sectional, nationwide population-based survey conducted in South Korea in 2020, the main reason for vaccine hesitancy was a lack of confidence in the COVID-19 vaccine. Less or no fear of COVID-19, unstable job status, decreased family income, and worsening health status were reported as predictors of vaccine hesitancy. Younger age, lack of religious affiliation, political conservatism, and lower family income have also been associated with vaccine hesitancy. Therefore, efforts to manage the epidemiological and socioeconomic factors associated with a high risk of vaccine hesitancy were important, with enhanced effective communication by providing evidence of vaccine efficacy.25 A previous study revealed a considerable level of COVID-19 vaccine hesitancy in South Korea and emphasized the importance of providing reliable and timely information to the public using social media, although its use has a positive and negative effect on the population’s vaccine decision.26 As global predictors of vaccine hesitancy, a lower perceived risk of getting infected, a lower level of institutional trust, lack of vaccination against influenza, lower levels of perceived severity of COVID-19, and stronger beliefs that the vaccination would cause side effects or be unsafe, have been identified; these predictors can be used to design public health policies or to evaluate subjects’ vaccine hesitancy.27
Table 1
Surveys analyzing vaccine hesitancy or refusal in Korea
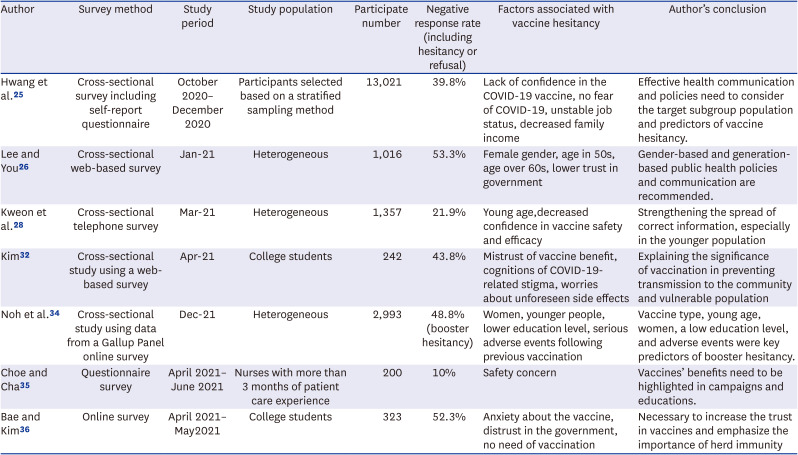
| Author | Survey method | Study period | Study population | Participate number | Negative response rate (including hesitancy or refusal) | Factors associated with vaccine hesitancy | Author’s conclusion |
|---|---|---|---|---|---|---|---|
| Hwang et al.25 | Cross-sectional survey including self-report questionnaire | October 2020–December 2020 | Participants selected based on a stratified sampling method | 13,021 | 39.8% | Lack of confidence in the COVID-19 vaccine, no fear of COVID-19, unstable job status, decreased family income | Effective health communication and policies need to consider the target subgroup population and predictors of vaccine hesitancy. |
| Lee and You26 | Cross-sectional web-based survey | Jan-21 | Heterogeneous | 1,016 | 53.3% | Female gender, age in 50s, age over 60s, lower trust in government | Gender-based and generation-based public health policies and communication are recommended. |
| Kweon et al.28 | Cross-sectional telephone survey | Mar-21 | Heterogeneous | 1,357 | 21.9% | Young age,decreased confidence in vaccine safety and efficacy | Strengthening the spread of correct information, especially in the younger population |
| Kim32 | Cross-sectional study using a web-based survey | Apr-21 | College students | 242 | 43.8% | Mistrust of vaccine benefit, cognitions of COVID-19-related stigma, worries about unforeseen side effects | Explaining the significance of vaccination in preventing transmission to the community and vulnerable population |
| Noh et al.34 | Cross-sectional study using data from a Gallup Panel online survey | Dec-21 | Heterogeneous | 2,993 | 48.8% (booster hesitancy) | Women, younger people, lower education level, serious adverse events following previous vaccination | Vaccine type, young age, women, a low education level, and adverse events were key predictors of booster hesitancy. |
| Choe and Cha35 | questionnaire survey | April 2021–June 2021 | Nurses with more than 3 months of patient care experience | 200 | 10% | Safety concern | Vaccines’ benefits need to be highlighted in campaigns and educations. |
| Bae and Kim36 | Online survey | April 2021–May2021 | College students | 323 | 52.3% | Anxiety about the vaccine, distrust in the government, no need of vaccination | Necessary to increase the trust in vaccines and emphasize the importance of herd immunity |
A telephone survey conducted among 1,357 persons aged > 18 years showed that the COVID-19 vaccine hesitancy rate was 21.9% which was highest among those aged < 30 years (33.4%) and lowest among those aged > 65 years (8.7%). Age and perceived confidence in vaccine safety and efficacy were reported to be associated with vaccine hesitation, and the importance of promoting accurate vaccine-related information was emphasized, especially among young people in this survey.28 In a cross-sectional study using a web-based survey conducted with 242 college students in April 2021, mistrust of vaccine benefits, cognition of COVID-19-related stigma, and worries about unforeseen future negative side effects from vaccination were associated with COVID-19 vaccine hesitancy. It has been mentioned that it is necessary to educate young people or their communities on the need for vaccination to block transmission to elderly or vulnerable groups.32
A cross-sectional online survey investigating the predictors of COVID-19 booster hesitancy among fully vaccinated young adults, women, younger people, those with a lower education level, those who received the mRNA-1273 vaccine type, and those who experienced serious adverse events following previous COVID-19 vaccination were associated with booster hesitancy, mainly due to concerns about safety and doubts about efficacy.3334
In one study on psychological factors influencing nurses’ intention to receive a COVID-19 vaccine, perceived barriers, and safety concerns negatively impacted vaccination intentions. It was emphasized that transparent and reliable information on the effectiveness and safety of vaccines should be disclosed, and their benefits should be well-known through campaigns and educational materials.35 Efforts are being emphasized to promote trust in vaccine safety and the necessity and importance of herd immunity to improve vaccination among young people, such as college students, nationwide.363738394041
Investigating the factors of healthcare workers’ vaccine hesitancy and its implications
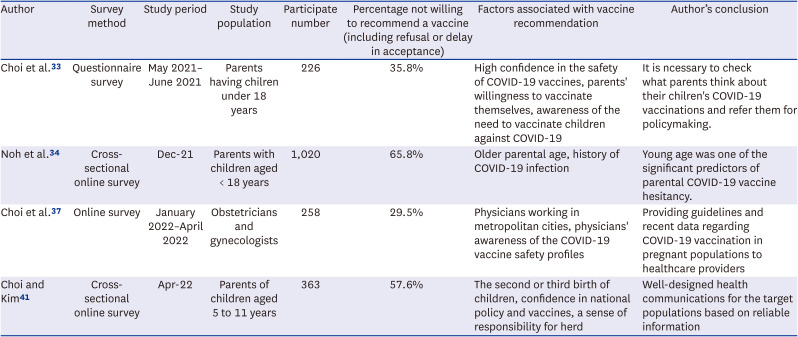
In a nationwide survey study of obstetricians and gynecologists analyzing the attitudes of healthcare providers regarding COVID-19 vaccine recommendations for pregnant women, 182 (70.5%) of 258 participants said that they would recommend that their pregnant patients be vaccinated against COVID-19. In this study, the most important factor in recommending COVID-19 vaccinations for pregnant women was using the “latest information on the safety of vaccines” and the main factor affecting future vaccination recommendations was “government and academic guidelines,” emphasizing the importance of providing the latest information and producing guidelines for pregnant women (Table 2).37
Table 2
Studies on the COVID-19 vaccination intentions in doctors for their patients and in parents for their children in Korea
| Author | Survey method | Study period | Study population | Participate number | Percentage not willing to recommend a vaccine (including refusal or delay in acceptance) | Factors associated with vaccine recommendation | Author’s conclusion |
|---|---|---|---|---|---|---|---|
| Choi et al.33 | questionnaire survey | May 2021–June 2021 | Parents having chilren under 18 years | 226 | 35.8% | High confidence in the safety of COVID-19 vaccines, parents' willingness to vaccinate themselves, awareness of the need to vaccinate children against COVID-19 | It is ncessary to check what parents think about their chilren's COVID-19 vaccinations and refer them for policymaking. |
| Noh et al.34 | Cross-sectional online survey | Dec-21 | Parents with children aged < 18 years | 1,020 | 65.8% | Older parental age, history of COVID-19 infection | Young age was one of the significant predictors of parental COVID-19 vaccine hesitancy. |
| Choi et al.37 | Online survey | January 2022–April 2022 | Obstetricians and gynecologists | 258 | 29.5% | Physicians working in metropolitan cities, physicians' awareness of the COVID-19 vaccine safety profiles | Providing guidelines and recent data regarding COVID-19 vaccination in pregnant populations to healthcare providers |
| Choi and Kim41 | Cross-sectional online survey | Apr-22 | Parents of children aged 5 to 11 years | 363 | 57.6% | The second or third birth of children, confidence in national policy and vaccines, a sense of responsibility for herd | Well-designed health communications for the target populations based on reliable information |
Although healthcare workers have advanced educational backgrounds, clinical experience, and membership in professional medical societies, some choose not to receive the vaccine. If healthcare workers are reluctant to get vaccinated, other members of the public may also be more reluctant. Inadequate vaccination pressure on some unvaccinated healthcare workers can have a more negative impact on their acceptance of vaccinations, and we should understand that healthcare workers can experience a number of rejection factors, such as from the general public. Various factors and situations of vaccine hesitancy should be understood, continuously evaluated, and improved upon.38
Furthermore, healthcare workers who initially decided not to be administered with COVID-19 vaccination have also agreed on COVID-19 vaccination through their colleagues who have positive beliefs about vaccination, thereby increasing access to vaccination program. Since healthcare workers who are hesitant about having vaccination most commonly complain of fear of adverse effects, sufficient education and promotion of their concerns, such as adverse effects targeting healthcare workers who are negative about vaccination, are expected to increase their participation in COVID-19 vaccination.3940
Factors influencing parents’ decisions on whether their children should be vaccinated against COVID-19
In a cross-sectional online survey of COVID-19 vaccination intentions in parents for their children, trust in COVID-19 vaccines and government quarantine policies, solidarity to protect others through vaccination, and anxiety-avoidance behavior to actively avoid COVID-19 were confirmed to be positive factors in parents’ intentions to vaccinate COVID-19 for their children aged 5 to 11 years.41
High confidence in the safety of COVID-19 vaccines, parents’ willingness to vaccinate themselves, and awareness of the need to vaccinate children against COVID-19 were associated with positive factors in intention to vaccinate their children.33
Therefore, the government should consider providing objective information on the risk of COVID-19, evidence-based information and periodic updates on the stability and effectiveness of vaccines in response to infection, false information management, pro-social motivation campaigns, and establishing various channels for interactive communication (Table 2).41
Factors that cause COVID-19 vaccination hesitancy among parents for their children include age, level of education, confidence in the safety of COVID-19 vaccines, parents’ willingness to vaccinate themselves, and COVID-19 infection; therefore, future vaccination policies should be carefully established through precise analysis.3441
ANALYSIS AND PREPARATIONS OF POSSIBLE VACCINE ADVERSE EFFECTS IN THE FUTURE
Controlling vaccine adverse effects and vaccine safety are critical in fighting emerging infectious diseases, such as the COVID-19 pandemic, and in increasing public confidence in vaccination. Vaccine-related injuries or death should be thoroughly investigated and evaluated nationally, and plans for such a goal should be established and prepared before the new infectious disease pandemic begins.42
The Korea Disease Control and Prevention Agency (KDCA) performed public efforts to strengthen the government’s responsibility for adverse events following COVID-19 vaccination. When local public health centers reported cases of adverse events related to COVID-19 vaccines to the KDCA, officials and professional advisors of the KDCA analyzed the cases scientifically, and then compensation costs were calculated individually through a committee meeting based on the results of the damage investigation.
Key adverse effects known in COVID-19 vaccination
Anaphylaxis, thrombotic events, and myocarditis are known to cause serious adverse effects that may lead to death after SARS-CoV-2 vaccination. Several studies have reported the incidence of anaphylaxis, myocarditis, and vaccine-induced immune thrombotic thrombocytopenia.174243 As the adverse effects identified in clinical studies before marketing approval do not represent all adverse effects of the vaccine, it is necessary to identify the vaccine side effects through continuous investigation and research activities and inform the public of new related issues and data.
Post-marketing safety assessment plan for vaccines approved for emergency use
In the pre-COVID period, it required more than four years for the vaccine to be developed after the virus was identified.4445 However, the Pfizer/BioNTech and Moderna COVID-19 vaccines were granted emergency use approval within a year after the viral gene sequence was reported. New vaccines approved for emergency use should be continuously monitored for adverse effects and safety issues even after emergency use authorization. For example, a cross-sectional, web-based survey conducted in December 2021 reported that a history of severe allergic reactions and the use of anticoagulants were closely related to hospital visits or hospitalization due to adverse effects of the COVID-19 vaccines.43
In vaccination-related deaths, investigation and research on postmortem examinations are essential. Therefore, guidelines on the investigation and research of severe life-threatening adverse effects and vaccination-related deaths must be preemptively prepared as one of the precautions for the possible emergence of infectious diseases.
TRAINING METHODS TO INCREASE VACCINATION OF NEWLY DEVELOPED VACCINES
In many cases, people want to be vaccinated because of fear of new infectious diseases; however, if the adverse effects of the vaccine are known and the adverse effects are misinformed, more people may be reluctant to be vaccinated. Therefore, it is important to develop early vaccination strategies, including the promotion of vaccination and disclosure of related information.15
Promoting educational campaigns
Educational campaign should be conducted to inform the public of the importance and effectiveness of vaccination. To this end, government and health organizations can lead the production of advertisements, posters, brochures, and promote them extensively through online media on SNS.
Strengthening the role of the healthcare workers
Healthcare workers should play a role in relieving patients’ concerns during vaccination and should explain the importance and effectiveness of vaccinations. Therefore, healthcare workers should receive training and information on vaccines, and in sharing their experiences and information with patients. The inclusion of vaccine-related education as an essential educational item in regular training courses for healthcare workers could also be a good idea.2930
For the nationwide large-scale vaccination of the latest vaccine against new infectious diseases, it is necessary to prepare specialized online education programs for each occupation, including doctors, nurses, pharmacists, and health officers. For example, if the latest guidelines of new vaccines for pregnant women are delivered to gynecologists in real-time and explained to the patients they are in charge of, the understanding and reliability of the new vaccines could be increased more effectively. In addition, if vaccine-related online education can be conducted for nurses who have retired or have not participated in work for a considerable period of time, it will contribute to the general public’s understanding and trust in new vaccines. Pharmacists and health officers who have a lot of contact with the public are also expected to be able to inform the public of vaccine-related information more accurately through online education and contribute to the success of large-scale vaccinations nationwide.63537
In future measures against new infectious diseases, it will be essential to establish and update online mandatory education programs specialized for each occupation of healthcare workers.
Reinforcement of vaccination facilities and infrastructure
The convenience of vaccination is an important factor, which may increase vaccination rates.1546 Vaccination facilities and infrastructure play an important role in performing large-scale vaccination programs. Therefore, more vaccination facilities, and manuals for efficient, large-scale vaccinations should be available in advance. It is necessary to have written protocols in preparing large-scale vaccination programs against possible infectious diseases in the future by analyzing problems and experiences in the nationwide vaccination process.
Positive compensation system
While mandatory COVID-19 vaccinations and negative incentive have contributed to overcoming the COVID-19 pandemic, some have questioned the effectiveness of these policies as issues of basic rights restrictions or vaccine safety, as well as the effectiveness of positive and negative incentives on COVID-19 vaccinations may vary depending on various situations.4748
While there are some objections to financial support, the effectiveness of positive incentives, such as gifts, vouchers, discounts, and financial support, for future vaccinations against new infectious diseases should also be fully evaluated and considered by health professionals or policymakers.49
COMMUNICATION BASED ON SCIENTIFIC DATA AND RESPONSE TO MISINFORMATION
The spread of misinformation about vaccination through social media may be linked to vaccine hesitancy. False beliefs about vaccines can vary depending on various factors, including age, sex, culture, race, religion, and region, and must be overcome through accurate knowledge transfer based on scientific facts.50
The importance of achieving herd immunity through vaccination
Without vaccinations during the COVID-19 pandemic, more deaths could have occurred in reaching herd immunity, defined as having 50–80% of the population immunized either by being naturally infected with COVID-19 or by vaccination.2351 Early and selective vaccination of individuals at high risk of infection and mortality could be expected to have many preventive effects, and immunological function could be more effectively induced through booster vaccination. Non-pharmaceutical interventions, such as patient isolation, wearing masks, social distancing, and hand hygiene, are known to be effective in preventing COVID-19; however, these methods limit the social and economic activities of the public. Therefore, it is difficult to maintain social distancing or containment policies for a long time nationwide, and rapid vaccine development and large-scale vaccination are required.5253
Transparent disclosure of vaccine effects and adverse effects information during clinical research
Without vaccination during the COVID-19 pandemic, more deaths could have occurred in the process of reaching herd immunity. Although vaccination is known to be an efficient way to herd immunity, several factors make it difficult to proceed with sufficient vaccinations that can lead to herd immunity worldwide. In addition, due to viral mutations or decreased immune function against COVID-19 over time, perfect herd immunity may not be reached, but only transient herd immunity, which may lead to COVID-19 infection again within 6 or 12 months after infection or vaccination.54
The general public was instructed to be immediately vaccinated rather than first giving accurate information about it. Health institutions and pharmaceutical companies should provide transparent and understandable adverse and preventive effects, such as COVID-19 vaccine development schedules, specific data on vaccine safety, and effects in phases 1, 2, and 3 of clinical studies. This transparent disclosure is expected to reduce reluctance to vaccinate, and large-scale vaccinations are expected to proceed more efficiently.55
Continued re-evaluation of new vaccines approved for emergency use to cope with infectious disease crisis
Many people, including healthcare workers, desire rapid vaccination against new infectious diseases; however, they also express doubts and anxiety about the safety and effectiveness of emergency-approved vaccines, which is one of the factors that make vaccination hesitant.
The long-term side effects of the currently approved COVID-19 vaccines remains unknown; therefore, long-term follow-up investigations are required.51 When the results of long-term follow-up investigations of approved vaccines are provided transparently, this will greatly reduce the public's reluctance to administer the vaccine.
OTHER CHALLENGES IN EFFECTIVE VACCINATION STRATEGIES AND EDUCATION FOR EMERGING INFECTIOUS DISEASES
Vaccination strategies for immunocompromised patients
Immunocompromised patients, such as those with malignant tumors of solid organs, hematologic malignancies, organ transplants, autoimmune diseases, or AIDS, are more susceptible to COVID-19.51 However, COVID-19 vaccination rates were lower in patients with chronic medical conditions compared to that in the general population in a nationwide, cross-sectional study.23 Therefore, awareness of a considerable gap between COVID-19 vaccination rates among patients with chronic medical disorders and those of the general population is required, and efforts need to be made to reduce the gap.
Immunocompromised patients were often excluded from COVID-19 vaccine clinical research; therefore, accurate research data targeting these groups remain insufficient. In addition, immunocompromised patients may have a higher mortality rate from COVID-19 than the general public because of the nature of the underlying diseases; therefore, it is necessary to actively evaluate the formation and continuation of immunity after vaccination to establish suitable vaccination guidelines.5156 Efforts to continuously assess and monitor vulnerable groups, including immunocompromised patients, are critical for successfully implementing long-term vaccination strategies against COVID-19.56
Developing a detailed guidance plan that targets different subgroups
Preferences for vaccination may vary depending on age, sex, occupation, and the underlying disease. Because these factors related to vaccine hesitancy vary from one subdivided small group to another, detailed plans for each subgroup should be developed in future vaccination strategies. In addition, appropriate vaccination guidelines for parents should be established based on their children’s age.53545556
DISCUSSION
In the early stages of the new infectious disease crisis, patient isolation, social distancing, containment, and hygiene measures were implemented; however, to end the pandemic, efficient and large-scale vaccinations are essential. Anxiety about vaccines approved for emergency use in the face of an infectious disease crisis, has affected not only the general public but also healthcare workers, making them hesitant to vaccinate. Owing to the easing of the COVID-19 pandemic, vaccinations for collective immunity have not sufficiently progressed worldwide; as a result, the emergence of new outbreaks or resistant viruses is feared.111315
Thus, we must prepare education and promotion plans for administering the newly developed vaccine to the public without much resistance, and to develop effective vaccines against newly emerging infectious diseases. In addition, efforts are needed to secure the necessity, legitimacy, and evidence for rapid vaccination on a large scale at the national level. Scientific evidence and explanatory statements must be prepared to make it easier for the public to understand large-scale vaccination plans.123456
In the early days of the pandemic, people were eager to get vaccinated immediately as increases in mortality were reported. However, if the adverse effects of the vaccine are known and more misinformed than they actually are, there may be an increasing number of people hesitating to get vaccinated. Nevertheless, rather than criticizing those who hesitate to get vaccinated, we should first acknowledge and understand their concerns and fears.253041
Achieving collective immunity through the vaccination of children, adolescents, and adults can be an important strategy to prevent the re-spread of COVID-19 infection in the community and the emergence of another mutation. Therefore, we need to structurally prepare early vaccination strategies to promote vaccination, such as educational campaigns, explanations of adverse effects for the general public, strengthening the role of healthcare workers, sharing experiences with vaccinated people, reinforcement of vaccination facilities and infrastructure, and positive compensation systems. Furthermore, parents’ psychological predispositions that affect their children’s vaccination decisions are important and can be strengthened by sharing vaccine-related education or intervention programs through their children’s educational institutions.343741
Moreover, we must also investigate the vaccine avoidance factors of healthcare workers, who can have a strong influence on patients’ vaccination decisions. Data on vaccine acceptance, rejection, and hesitation among Korean domestic healthcare workers are insufficient. A full understanding of the factors that make healthcare workers reluctant to vaccinate is needed for the success of large-scale vaccinations in the future.637383940
The spread of misinformation about vaccination through social media may be linked to vaccine hesitancy, which may vary on different factors, including age, sex, culture, race, religion, and region. In addition, fake news should be resolved by sharing accurate knowledge based only on scientific facts.2526272834
Many global and national policies have been implemented to end the COVID-19 pandemic; however, there has been inevitable damage and insufficient measures without prior preparation. It is necessary to prepare in advance for cases in which a newly emerging infectious disease can cause a medical crisis. In addition to the development of new vaccines and treatments, educational strategies should be established to promote large-scale vaccination programs and vaccine-awareness campaign to the general public should be performed.
 XML Download
XML Download