

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The assessment of daily functioning is an important factor in the diagnosis and prognosis of dementia. Loss of everyday function is a major diagnostic factor that differentiates mild cognitive impairment (MCI) from dementia.1 The MCI stage is associated with subtle decrements in everyday functioning.2345 However, a greater degree of everyday functional impairment in MCI is associated with faster subsequent cognitive decline and conversion to dementia.67 Further, older adults without cognitive impairment who experience subtle everyday functional difficulties are also at elevated risk of progressing to MCI.89
Although several questionnaires have been developed to measure the everyday functional abilities, most of them have important limitations. They consist of a small number of items that are not sufficient to assess mild impairments in everyday functioning and represent too simplistically the disparate abilities in daily functioning into one global index.10 The Everyday Cognition (ECog)11 was developed as a psychometrically rigorous tool to assess everyday functional abilities in older adults across a wide range of abilities. Specifically, the ECog measures everyday functional abilities relevant to specific neuropsychological domains.11 Its validity has been evaluated by examining its relationship with objective measures of neuropsychological function and neurobiological markers of disease including structural neuroimaging findings.121314
The ECog has been used in a variety of clinical and research contexts, including large-scale longitudinal studies such as the Alzheimer’s Disease Neuroimaging Initiative (ADNI).15 The ECog is known to be sensitive to subtle and mild everyday functional changes in MCI.241116 In addition, the ECog can predict disease progression from MCI to dementia6717 as well as from normal cognition to MCI.8 It also demonstrates good discrimination between Alzheimer’s disease (AD) and frontotemporal dementia,18 and it has been shown to be a valid measure of everyday function in other degenerative diseases such as Huntington’s disease19 and Parkinson’s disease (PD).20 Recently, it is also used to screen subjective cognitive decline.212223
The original version of the ECog11 consists of 39 items, covering one global factor and six cognitively relevant domains such as memory, language, visuospatial abilities, and three executive domains (including planning, organization, and divided attention). The short version of ECog (ECog-12)24 was also developed using an item response theory (IRT) analysis and consists of 12 items (including 2 items from each of the 6 cognitive domains of ECog). Tomaszewski Farias et al.,24 who developed a short version of the ECog, explained that their goal was to reduce the number of items in the original ECog while retaining its good psychometric properties.
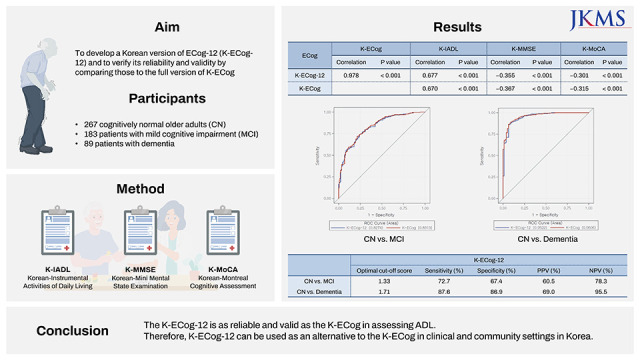
The Korean version of ECog (K-ECog)25 was standardized in 2019 and has been used in clinical and research fields.2627 However, there has been a need for a shortened version since the 39 items in the K-ECog were too long for clinical use. The purpose of this study was to develop a Korean version of ECog-12 (K-ECog-12) and to verify its reliability and validity by comparing those to the full version of K-ECog to see if it can be used as an alternative to the K-ECog.
METHODS
Participants
The participants were 267 cognitively normal older adults (CN), 183 patients with mild cognitive impairment (MCI), and 89 patients with early stage of dementia. As the ECog is an informant-rated questionnaire, the caregivers of all participants also participated in the study. Healthy older adult participants were recruited through community outreach. Participants who fulfilled Christensen’s health screening criteria28 and showed normal performance on the Korean-Mini Mental State Examination (K-MMSE)29 were included in the healthy group. Participants with MCI or dementia were selected from among patients who visited the department of neurology of university hospitals.
All patients underwent a clinical diagnostic workup for dementia evaluation, which included a comprehensive neuropsychological test battery and brain imaging studies. The clinical diagnoses of MCI and dementia were based on the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-V).30 Cognitive impairment was defined as a decline in performance by at least 1.0 standard deviation (SD) below the normal norms.31 The activities of daily living (ADL) status of patients was assessed based on the Korean version of the Instrumental Activities of Daily Living (K-IADL).32 The MCI and dementia groups included patients with a Clinical Dementia Rating (CDR)33 global score of 0.5 and 1.0, respectively. The MCI included patients with mild neurocognitive disorder (NCD) due to AD (n = 135, 73.8%), mild vascular NCD (n = 20, 10.9%), mild NCD due to PD (n = 12, 6.6%), and unspecified mild NCD (n = 16, 8.7%). The dementia group included patients with major NCD due to AD (n = 76, 85.4%), major vascular NCD (n = 12, 13.5%), and major NCD due to multiple etiologies (n = 1, 1.1%). To assess test–retest reliability, 51 participants selected from the CN group were re-administered the K-ECog after a 4-week interval.
Materials
K-ECog
The ECog-1224 consists of 12 items, including 2 items from each of the six cognitive domains of the ECog. To identify appropriate items to be included in an abbreviated ECog, Tomaszewski Farias et al.24 examined the estimates of item difficulty of all 39 items in the full version ECog using an IRT analysis. Based on the IRT results, Tomaszewski Farias et al.24 selected the two items in each ECog domain that had the highest and lowest item difficulty estimates.
To newly select the items that comprise the K-ECog-12 and to compare the reliability and validity of the K-ECog-12 with the K-ECog, the full version K-ECog25 was administered to all participants’ informants. We aimed to retain as many items from the original ECog-1224 as possible, but replace items that were not appropriate for Korean older adults due to cultural differences with other items from the K-ECog.
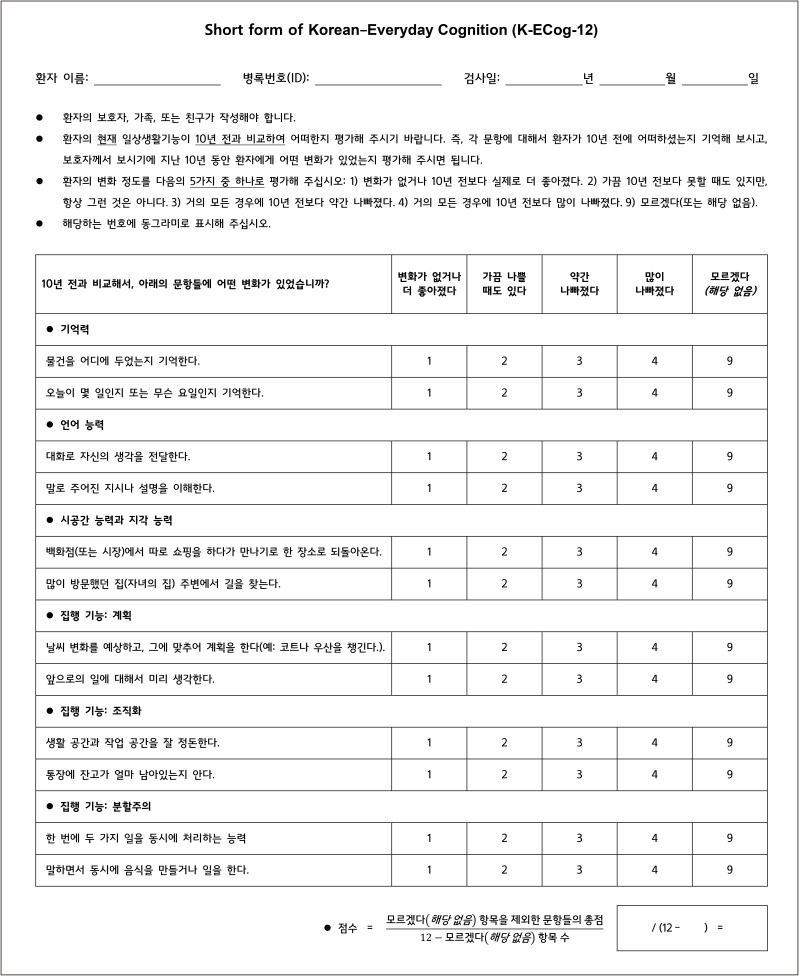
The K-ECog, like the original ECog,11 is an informant-rated measure of cognitively relevant everyday abilities. It consists of 39 items, covering one global factor and six cognitively relevant domain-specific factors. The items include the following: eight for memory, nine for language, seven for visuospatial function, and fifteen for executive function domains (including five items for planning, six items for organization, and four items for divided attention). For each item, informants were asked to compare the participants’ current level of everyday functioning with their level of functioning 10 years earlier. The response options included the following: 1 = better or no change, 2 = occasionally worse, 3 = consistently a little worse, 4 = consistently much worse, and “I don’t know”. The K-ECog global score is the sum of all items divided by the number of items completed (excluding the number of items with “I don’t know” responses), and its values range from 1 to 4.
Neuropsychological measures
The K-MMSE and Korean-Montreal Cognitive Assessment (K-MoCA)34 were administered to all participants, and their informants completed the K-IADL.32 For patients in the MCI and dementia groups, CDR32 and the Global Deterioration Scale (GDS)35 were administered to measure the severity of dementia. The Short form of the Geriatric Depression Scale (SGDS)36 was also given to control for depression levels in all groups.
Statistical analysis
Group differences were examined using one-way analysis of variance (ANOVA). Variables that were found to be significantly different in the ANOVA were further analyzed with post-hoc comparisons using the Bonferroni correction. The IRT analysis was used to select new items from the K-ECog items to replace ECog-12 items that were inappropriate for Korean older adults. Pearson’s χ2 test was used to analyze categorical variables. Internal consistency was assessed using Cronbach’s α coefficient. The test–retest reliability was assessed using Pearson’s correlation coefficient (r). Convergent validity was evaluated by calculating the partial correlation coefficients among the K-ECog-12, K-ECog, K-IADL, K-MMSE, and K-MoCA. Analysis of covariance (ANCOVA) was used to evaluate the differences in K-ECog-12 and K-ECog scores between the three groups (CN, MCI, and dementia); for this analysis, the age, years of education, and depression level of participants were included as covariates. Receiver operating characteristic (ROC) curve analyses were performed to examine the ability of the K-ECog-12 and K-ECog to discriminate across groups while controlling for the effects of age, years of education, and depression level. The optimal cut-off scores, sensitivity, specificity, and positive and negative predictive values of K-ECog-12 were obtained using ROC curve analyses.
ANOVA, reliability analysis, correlation analysis, and ANCOVA were performed using IBM SPSS Statistics 25.0 (IBM Corp., Armonk, NY, USA). IRT analysis was conducted using the R program. The Statistical Analysis Software (SAS) and MedCalc version 19.4 (MedCalc Software, Ostend, Belgium) were used for ROC curve analysis.
RESULTS
Development of K-ECog-12
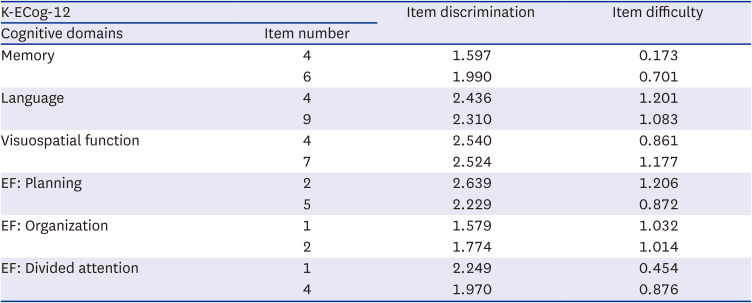
To develop the K-ECog-12, we first selected the items corresponding to the original ECog-12 from the 39 items in K-ECog. We found that one of the 12 items had an “I don’t know” response for 29.3% of all participants, while the rest of the items had 12.6% or less. The item with the highest “I don’t know” response rate of 29.3% was “reading a map and helping with directions when someone else is driving” in the visuospatial function domain, with rates of 22.5% for CN, 33.1% for MCI, and 42.7% for dementia. Therefore, we decided that this item was not appropriate for older Koreans, who were less likely to use maps, and decided to keep the remaining 11 items. To select the new item to replace, we performed an analysis similar to the statistical analysis used by Farias et al. to develop ECog-12. We used the generalized partial credit model (GPCM)37 of the polytomous IRT models and selected one item from the visuospatial function domain of K-ECog with a low item difficulty estimate and a low “I don’t know” response rate of 8.7%. As a result, “reading a map and helping with directions when someone else is driving” was replaced with “finding the way back to a meeting spot in the mall or other location.” Similar to how the K-ECog global score is calculated, the K-ECog-12 score was calculated by averaging the scores of the 12 selected items (excluding items with “I don’t know” responses). Table 1 lists item discrimination and difficulty parameters from IRT analysis of each K-ECog-12 item. Appendix 1 lists the items in K-ECog-12.
Table 1
GPCM item parameter estimates of K-ECog-12
Demographic and other characteristics of participants
The demographic characteristics of all group participants are summarized in Table 2. There were no significant differences in sex ratio between groups, but significant differences were observed in age, years of education, depression level, IADL scores, general cognitive function (K-MMSE and K-MoCA scores), and severity of dementia (CDR and GDS scores).
Table 2
Demographic characteristics of the participants

Values are presented as mean ± standard deviation.
CN = cognitively normal older adults, MCI = mild cognitive impairment, SGDS = Short form of the Geriatric Depression Scale, K-IADL = Korean-Instrumental Activities of Daily Living, K-MMSE = Korean-Mini Mental State Examination, K-MoCA = Korean-Montreal Cognitive Assessment, CDR-GS = Clinical Dementia Rating-Global Score, CDR-SB = Clinical Dementia Rating-Sum of Boxes, GDS = Global Deterioration Scale.
Reliability
The Cronbach’s α coefficient was 0.95 for K-ECog-12 and 0.99 for K-ECog. The Pearson’s correlation coefficients for test–retest reliability (mean interval, 31 days; range, 13–42 days) were 0.67 (P < 0.001) for K-ECog-12 and 0.73 (P < 0.001) for K-ECog, with no significant difference between the 2 scales (Fisher’s z = −0.58, P = 0.563).
Validity
The K-ECog-12 were strongly correlated with the K-ECog (r = 0.978, P < 0.001). The K-ECog-12 was also significantly correlated with K-IADL, K-MMSE, and K-MoCA to about the same degree as the K-ECog (Table 3). The K-ECog-12 showed a significant positive correlation with K-IADL (r = 0.677, P < 0.001) and significant negative correlations with K-MMSE (r = −0.355, P < 0.001) and K-MoCA (r = −0.301, P < 0.001). K-ECog also showed a significant correlation with K-IADL (r = 0.670, P < 0.001), K-MMSE (r = −0.367, P < 0.001) and K-MoCA (r = −0.315, P < 0.001). The correlations of K-ECog-12 with the K-IADL, K-MMSE, and K-MoCA were not significantly different from the corresponding correlations of K-ECog (Fisher’s z = −0.20, P = 0.840; Fisher’s z = −0.22, P = 0.825; Fisher’s z = −0.25, P = 0.804).
Table 3
Partial correlation of the K-ECog-12, K-ECog, K-IADL, K-MMSE, and K-MoCA

Values are presented as partial correlation coefficients controlled for age, education, and depression level.
K-ECog-12 = Short version of Korean-Everyday Cognition-12 items, K-ECog = full-length 39 items of Korean-Everyday Cognition, K-IADL = Korean-Instrumental Activities of Daily Living, K-MMSE = Korean-Mini Mental State Examination, K-MoCA = Korean-Montreal Cognitive Assessment.
ANCOVA showed that the between-group differences were significant for both K-ECog-12 (F[2,517] = 98.79, P < 0.001) and K-ECog (F[2,517] = 106.99, P < 0.001). Post-hoc analysis with Bonferroni correction showed that for both scales, the scores of each group were significantly different from those of the other 2 groups (Table 4).
Table 4
Group differences of the K-ECog-12 and K-ECog

ROC curve analysis revealed that K-ECog-12 did not differ from K-ECog in discriminating between the CN, MCI, and dementia groups. Figs. 1 and 2 show ROC graphs for K-ECog-12 and their comparisons with those for K-ECog. In, Fig. 1, the areas under the curve (AUCs) of K-ECog-12 and K-ECog were the same, meaning that there was no difference in the discriminability of the two scales in discriminating between CN and MCI (0.83 vs. 0.83; χ2 = 1.44, P = 0.231) (Fig. 1). No significant difference was also observed between the AUCs of K-ECog-12 and K-ECog (0.95 vs. 0.96; χ2 = 2.94, P = 0.087) in discriminating between CN and dementia (Fig. 2). Table 5 lists the AUC values for K-ECog-12 and K-ECog, as well as the AUC values for K-IADL, K-MMSE, and K-MoCA. The differences in AUCs between K-ECog-12 and K-IADL (0.83 vs. 0.84; χ2 = 1.09, P = 0.298), K-MMSE (0.83 vs. 0.85; χ2 = 0.63, P = 0.426), and K-MoCA (0.83 vs. 0.85; χ2 = 1.26, P = 0.263) were not significant for discriminating between CN and MCI. In discriminating between CN and dementia, the AUC of K-ECog-12 (0.95 vs. 0.98; χ2 = 8.94, P = 0.003) was significantly smaller than that of K-IADL. However, there were no significant differences in AUCs between K-ECog-12 and K-MMSE (0.95 vs. 0.98; χ2 = 2.63, P = 0.105) and K-MoCA (0.95 vs. 0.97; χ2 = 1.25, P = 0.264).
Fig. 1
ROC curves for the K-ECog-12 and K-ECog in the comparison between CN and MCI.
ROC = receiver operating characteristic, K-ECog-12 = Short version of Korean-Everyday Cognition-12 items, K-ECog = full-length 39 items of Korean-Everyday Cognition, CN = cognitively normal older adults, MCI = mild cognitive impairment.
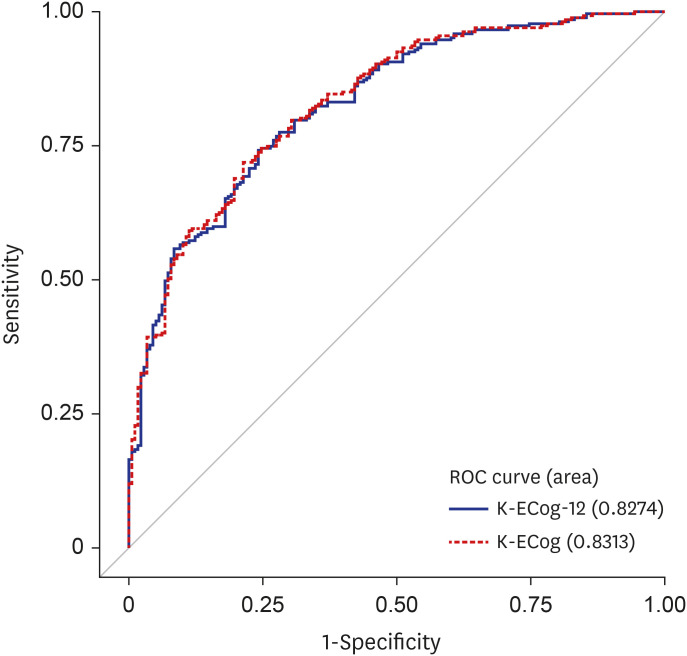
Fig. 2
ROC curves for the K-ECog-12 and K-ECog in comparison between CN and dementia.
ROC = receiver operating characteristic, K-ECog-12 = Short version of Korean-Everyday Cognition-12 items, K-ECog = full-length 39 items of Korean-Everyday Cognition, CN = cognitively normal older adults.
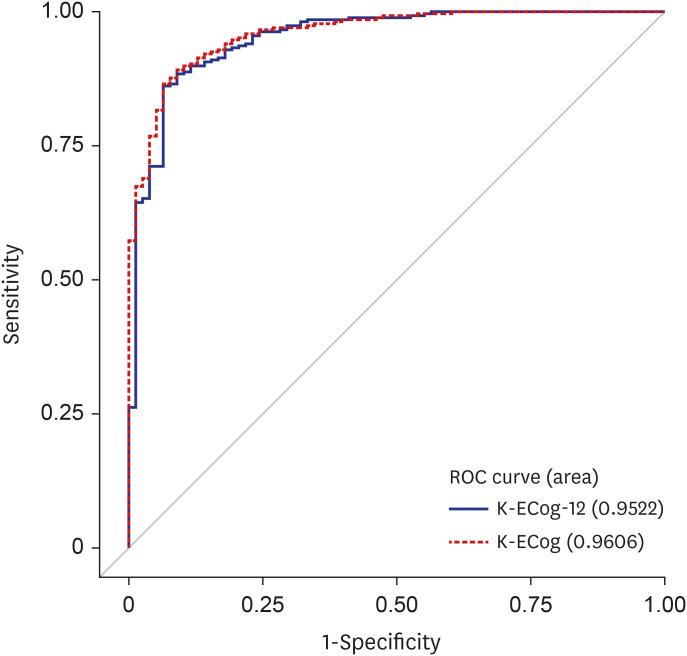
Table 5
AUCs of the K-ECog-12, K-ECog, K-IADL, K-MMSE, and K-MoCA in group comparison

AUC = area under the curve, K-ECog-12 = Short version of Korean-Everyday Cognition-12 items, K-ECog = full-length 39 items of Korean-Everyday Cognition, K-IADL = Korean-Instrumental Activities of Daily Living, K-MMSE = Korean-Mini Mental State Examination, K-MoCA = Korean-Montreal Cognitive Assessment, CI = confidence interval, LL = lower limit, UL = upper limit, CN = cognitively normal older adults, MCI = mild cognitive impairment.
The optimal cut-off scores, sensitivity, specificity, and positive and negative predictive values for each comparison are presented in Table 6. In discriminating between CN and MCI, K-ECog-12 had a sensitivity of 72.7% and a specificity of 67.4% (optimal cut-off score = 1.33). The sensitivity of K-ECog-12 to discriminate between CN and dementia was 87.6% and specificity was 86.9% (optimal cut-off score = 1.71).

DISCUSSION
In this study, we developed a shortened K-ECog-12 consisting of items appropriate for a Korean sample and compared its reliability and validity with the full version of K-ECog. The K-ECog-12 was constructed by replacing one item in the original ECog-12 that was inappropriate for older Koreans who do not use maps frequently and had the highest percentage of “I don’t know” responses with another item. Using IRT analysis, we selected a new item with lower item difficulty estimate and lower “I don’t know” responses in the visuospatial domain to which the item to be replaced belonged. The results showed that the percentage of “I don’t know” responses decreased from 0.6% to 29.3% for the original ECog-12 items to 0.6% to 12.6% for the K-ECog-12 items. It suggests that the K-ECog-12 is more suitable than the original ECog-12 for assessing cognitively related everyday functional abilities in the Korean elderly.
The Cronbach’s α coefficient for the K-ECog-12 was found to be as excellent level38 as K-ECog. In addition, the K-ECog-12 showed significant test-retest reliability that was not different from the K-ECog.
We investigated the convergent validity of the K-ECog-12 by evaluating its relationship with traditional measures of daily function and cognitive function. K-ECog-12 was significantly correlated with another ADL measure, K-IADL and was also significantly correlated with cognitive screening tests such as K-MMSE and K-MoCA. These correlations were not significantly different from the correlations between K-ECog and these measures. These results indicate that the K-ECog-12 has good convergent validity with traditional ADL and cognitive screening measures, with no differences from the full version of the K-ECog.
To determine the discriminability of the K-ECog-12, we examined whether the K-ECog-12 could indicate differences in scores between CN, MCI, and dementia groups. As a result, K-ECog-12 was able to distinguish between the three groups, and significant differences were observed between groups. These results are consistent with those found with K-ECog in previous studies.112425
ROC curve analyses showed that the K-ECog-12 was able to discriminate between cognitively normal and cognitively impaired patients at the same level as the K-ECog. Both scales showed “very good to excellent” diagnostic accuracy39 (AUC, 0.83–0.96). K-ECog-12 was able to significantly discriminate between CN and MCI groups, and its discriminability was not different from that of K-IADL, K-MMSE, and K-MoCA. However, K-ECog-12 was significantly less discriminating than K-IADL in distinguishing between CN and dementia groups, but did not differ from the discriminability of K-MMSE and K-MoCA. This may be because the present study used the K-IADL as a measure of ADL to diagnose whether participants had dementia. However, the fact that the 12-item scale reported by the informant had the same level of discriminability as cognitive screening tests such as the MMSE and MoCA demonstrates the usefulness of the K-ECog-12.
We present the optimal cut-off scores of the K-ECog-12 for use in differentiating MCI and dementia patients from cognitively normal older adults. K-ECog-12 had significantly higher sensitivity (87.6%) and specificity (86.9%) to distinguish CN from dementia patients. The sensitivity (72.7%) of K-ECog-12 for differentiating MCI patients from CN may not seem high, but it is similar to the sensitivity of the K-IADL (73.6%), which has been widely used as a measure of ADL to diagnose dementia.32
In the K-ECog validation study,25 the optimal cut-off scores for distinguishing amnestic MCI and AD patients from cognitively normal older adults were reported to be 1.41 (sensitivity = 70.5%, specificity = 77.5%) and 1.61 (sensitivity = 81.7%, specificity = 93.5%), respectively. However, these results are not directly comparable to the results of the K-ECog-12 due to the different comparison groups. Therefore, we performed further analyses of how well K-ECog-12 distinguishes amnestic MCI (n = 135) and AD (n = 76) patients from CN in the current study participants. On the K-ECog-12, the optimal cut-off scores to distinguish amnestic MCI and AD patients from CN were 1.42 (sensitivity = 72.4%, specificity = 73.4%) and 1.71 (sensitivity = 85.7%, specificity = 86.9%), respectively.
The original ECog-12 was constructed to reflect six cognitively relevant functional domains, but unlike the 39-item full version of the ECog, it was designed to yield only an overall score, not cognitive domain factor scores. As a further analysis, we performed a discriminant analysis to find which items of the K-ECog-12 were most sensitive in detecting functional impairment. The results showed that four items on K-ECog-12 were most effective in discriminating between CN and MCI patients, including “remembering where she/he has placed objects” and “remembering the current date or day of the week” in the memory domain, and “the ability to do two things at once” and “cooking or working and talking at the same time” in the divided attention domain of executive function. This finding is consistent with previous research showing that memory and executive function, particularly divided attention, are impaired in MCI,124041 and demonstrates that everyday functions related to memory and executive function can effectively distinguish between CN and MCI.4243
Overall, these results demonstrated that the K-ECog-12 is as reliable and valid as the K-ECog for identifying early functional dysfunction in everyday life. Traditional ADL scales, including the K-IADL, have been used primarily to differentiate between dementia and non-dementia, making it difficult to detect mild ADL decline. In addition, most items on traditional ADL scales focus on the ADL itself, making it difficult to determine which cognitive impairment is causing difficulty with a particular activity. The ECog-12, however, measures ADL functional ability segmented by the associated neuropsychological cognitive function. Therefore, the K-ECog-12 can provide indirect information about a patient’s cognitive dysfunction, information that cannot be obtained from the K-IADL.
In addition, cognitive screening tests such as the MMSE and MoCA require face-to-face interaction with patients, can be time-consuming, and require a trained examiner to administer the test. However, community health centers and primary care clinics often do not have trained examiners, making objective cognitive screening unavailable. We found that the K-ECog-12 did not differ from the K-MMSE or K-MoCA in its ability to differentiate between normal and MCI or between normal and dementia. Therefore, the K-ECog-12, which is an informant-rated scale and can be easily administered without specialized training, is expected to be particularly useful in primary care clinics and community health centers, where many patients need to be screened quickly. Therefore, K-ECog-12 can be used as an alternative to the K-ECog in clinical and community settings in Korea.
To increase its clinical utility, we provided optimal cut-off scores for interpreting the results of the K-ECog-12. However, additional cross-validation with independent samples is needed to validate the usefulness of these cut-off scores.
In addition, although K-ECog-12 was developed for informant rating, there are many elderly people in Korea who live alone and visit hospitals alone. Therefore, further studies are needed to compare the self-rated and informant-rated versions of the K-ECog-12 in elderly people so that it can be used for elderly people who visit hospitals alone.
 XML Download
XML Download