

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Acute myeloid leukemia (AML) is a hematologic malignancy characterized by the rapid proliferation of abnormally differentiated myeloid blast cells.1 AML, the most common type of leukemia in adults worldwide,2 predominantly affects elderly individuals, with about 60% of patients diagnosed at ≥ 65 years of age.3 From 1990 to 2017, the global incidence of AML rose by 87%, with 119,570 cases recorded in 2017.4 In Korea, AML is the most frequently diagnosed myeloid malignancy and is most prevalent in patients aged 60 to 79 years.5 Despite the greater prevalence of AML in older vs. younger adults, survival outcomes for this population remain extremely poor.6
The current standard of care for AML is intensive chemotherapy (ICT), but approximately 50% of patients are ineligible for this treatment7 owing to factors such as advanced age, poor performance status, and prevalence of comorbidities.89 AML-related genetic abnormalities can also increase the likelihood of resistance to ICT.9 Treatment options for these patients remain limited and include low-intensity treatment with hypomethylating agents (HMAs), low-dose cytarabine (LDAC), and best supportive care (BSC).21011 The availability of targeted therapies, such as inhibitors of B-cell lymphoma-2, isocitrate dehydrogenase isoforms 1/2, FMS-like tyrosine kinase-3 (FLT3), and Hedgehog, is also increasing for patients who are ineligible for ICT.12
Prognostic models have been developed to determine the suitability of older patients for ICT, yet there is no consensus regarding their optimal treatment.131415 Treatment decision-making for elderly patients with AML is an escalating global clinical challenge in light of emerging new agents and is compounded by an increasing incidence of AML due to the aging population.416 Thus, there is a growing need to understand current treatment strategies and their associated clinical outcomes in patients who are ineligible for ICT.
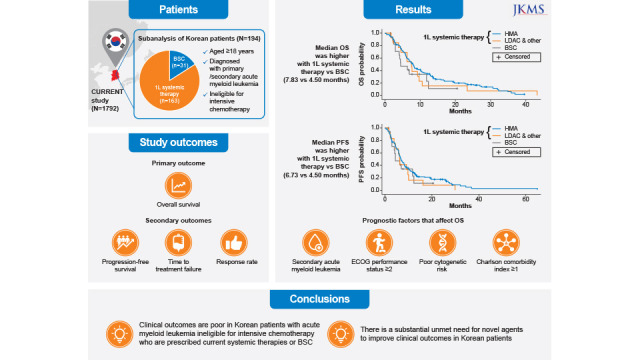
The CURRENT study was an international, real-world, non-interventional, retrospective chart review that aimed to evaluate clinical outcomes, clinicopathologic characteristics, and treatment patterns of patients with AML deemed ineligible for ICT.17 Here, we report that clinical outcomes were poor among the subgroup of Korean patients included in the CURRENT study.
METHODS
Study design
The CURRENT study17 enrolled 1,792 patients across 112 community or hospital medical centers from 22 countries between January 1, 2015, and December 31, 2018; four of the medical centers were in Korea.
Study population
Eligible patients were aged ≥ 18 years, diagnosed with primary or secondary AML, and ineligible for ICT based on physician assessment of age, Eastern Cooperative Oncology Group (ECOG) performance status, comorbidities, regional guidelines, and institutional practice. Patients were also required to have commenced first-line systemic therapy with low-intensity chemotherapy (e.g., HMAs, including azacytidine and decitabine, or LDAC), targeted therapy, or BSC and to have attended at least two practice visits to the physician during the treatment period in addition to the initial treatment visit. Exclusion criteria included undiagnosed AML, acute promyelocytic leukemia, and having received first-line therapy for AML in a clinical trial. Patients were followed up until the last recorded contact or death (whichever came first), and all visits were completed before data extraction.
Endpoints
The primary endpoint was overall survival (OS; measured from diagnosis of AML). Secondary endpoints included progression-free survival (PFS), time to treatment failure (TTF), response rate (including complete remission [CR] and CR with incomplete hematologic recovery [CRi]), and duration of response (DoR).
Data collection
Anonymized patient data including age, sex, disease characteristics, prior treatment, ECOG performance status, cytogenetic risk, and Charlson comorbidity index (CCI) were extracted from patient charts and/or site documentation, and recorded via electronic case report forms (CRFs) completed by each center.
Sample size
Target sample size for the overall CURRENT study was 1,600 patients, and the target sample size in Korea was 170 patients. Because of the descriptive nature of the study, formal statistical power considerations are not provided. However, the sample size was considered sufficient to provide reasonably precise estimates.
Statistical analyses
Data analyses were primarily descriptive. Continuous variables were described using mean, standard deviation, median, and ranges. Categorical variables were reported as counts and proportions. Time-to-event data were estimated using the Kaplan-Meier method, with median time and 95% confidence intervals (CIs) reported. Log-rank test or Wilcoxon test were used to compare Kaplan-Meier estimates of survival between patient subgroups. Cox regression analyses were performed to evaluate the association between patient variables and estimates of median OS and PFS. Missing data were captured via an “unknown” option in the electronic CRFs wherever appropriate. No imputation was performed, and all analyses were conducted on available data only.
Ethics statement
Notification was made to the responsible ethics committees, health institutions, and/or competent authorities as required by local laws and regulations. Ethics committee approval was obtained for this study, with the following Institutional Review Board approval numbers (Seoul National University Bundang Hospital: B-1908/559-102; Korea University College of Medicine: K2019-1535-001; Chungnan National University School of Medicine: 2019-09-027; Asan Medical Center: S2019-1692-0001). Informed consent was waived because of the retrospective nature of the study. Data collection was carried out anonymously, and final data cut-off was March 31, 2020.
RESULTS
Patient demographics and clinical characteristics
At final data cut-off, 194 Korean patients were enrolled. Patient baseline characteristics by treatment group are provided in Table 1. In the first-line systemic therapy and BSC groups, respectively, median age was 74.0 and 78.0 years, 64.4% and 48.4% of patients were male, and secondary AML was diagnosed in 25.2% and 29.0% of patients. The majority (73.0%) of patients in the first-line systemic therapy group had an ECOG performance status of 0 or 1; in the BSC group, approximately half (51.6%) had an ECOG performance status ≥ 2. Cardiovascular, pulmonary, liver, renal, and other comorbidities were reported in 130 (89.7%), 18 (100.0%), and 28 (90.3%) patients who received HMA, LDAC and other systemic therapies, and BSC, respectively (Supplementary Table 1).
Table 1
Baseline demographics and patient characteristics
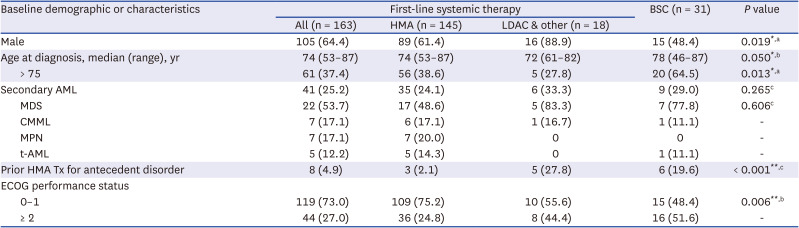
Data are number (%) unless otherwise stated.
AML = acute myeloid leukemia, BSC = best supportive care, CMML = chronic myelomonocytic leukemia, ECOG = Eastern Cooperative Oncology Group, HMA = hypomethylating agent, LDAC = low-dose cytarabine, MDS = myelodysplastic syndrome, MPN = myeloproliferative neoplasm, t-AML = therapy-related AML, Tx = treatment.
P value indicates statistical difference in a three-way comparison between BSC, HMA, and LDAC and other systemic therapies: *P < 0.05, **P < 0.01.
aChi-squared test; bKruskal-Wallis test; cFisher’s exact test.
Patient molecular profiling and cytogenetic risk data by treatment groups are provided in Supplementary Table 2. Of the patients who received first-line systemic therapy with available cytogenic risk data (n = 145), 66 (45.5%), 30 (20.7%), and 49 (33.8%) had favorable, intermediate, and poor risk, respectively, according to the cytogenetic risk classification in the CRF (Supplementary Table 3). Of 16 patients who received BSC with available cytogenic risk data, the respective risk proportions were seven (43.8%), four (25.0%), and five (31.2%) patients. Of the patients who received first-line systemic therapy with available molecular data (obtained using next-generation sequencing or targeted mutation testing; n = 144), 49 (34.0%) had a mutation. None of the patients who received BSC with available molecular data (n = 22) had mutations.
Patients who received first-line systemic therapy were more likely to be < 75 years of age compared with the BSC group (62.6% vs. 35.5%), more likely to be male (64.4% vs. 48.4%), and more likely to have an ECOG performance status < 2 (73.0% vs. 48.4%) and poor cytogenic risk (30.1% vs. 16.1%). Among patients who received first-line systemic therapy who had AML-related mutation(s), NPM1 (n = 11; 22.4%), MLLPTD
(n = 11; 22.4%), CEBPA (n = 8; 16.3%), TET2 (n = 8; 16.3%), and FLT3ITD (n = 7; 14.3%) were most frequently identified.
Among the 194 patients in this Korean subanalysis, 163 (84.0%) received first-line systemic therapy and 31 (16.0%) received BSC; data for the number of patients who received allogenic stem cell transplantation were not collected. In the first-line systemic therapy group, 10 had ongoing treatment, 152 discontinued treatment, and the status of one patient was unknown (Supplementary Fig. 1). There were 145 (89.0%) patients who received HMA monotherapy (azacytidine, n = 5 [3.1%]; decitabine, n = 140 [85.9%]), five (3.1%) who received LDAC monotherapy, and 13 (8.0%) who received HMA and/or LDAC in combination with other systemic therapies (Supplementary Fig. 2).
Primary endpoint
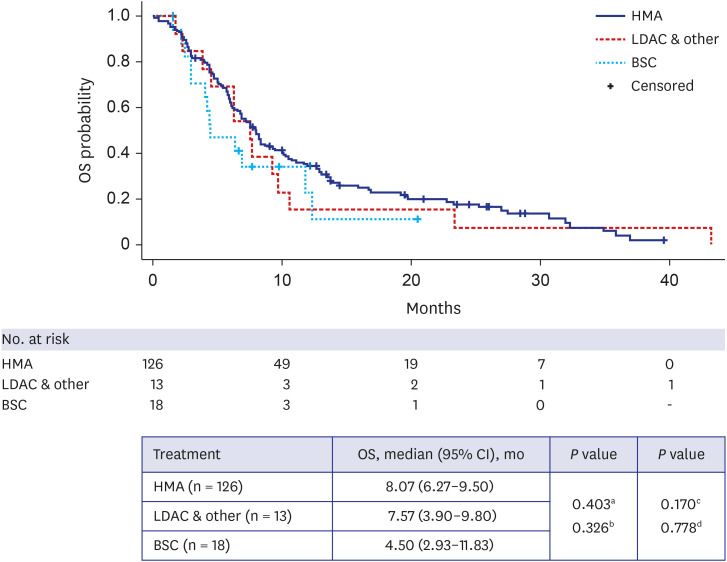
Median (95% CI) OS was 7.83 (6.30–9.27) months in patients who received systemic therapy (HMAs, 8.07 [6.27–9.50] months; LDAC and other systemic therapies, 7.57 [3.90–9.80] months), and 4.50 (2.93–11.83) months in those who received BSC (Table 2, Fig. 1). Thirty-seven patients had missing OS data.
Table 2
Median OS, PFS, TTF, response rate, and duration of response for patients who received first-line systemic therapy or BSC
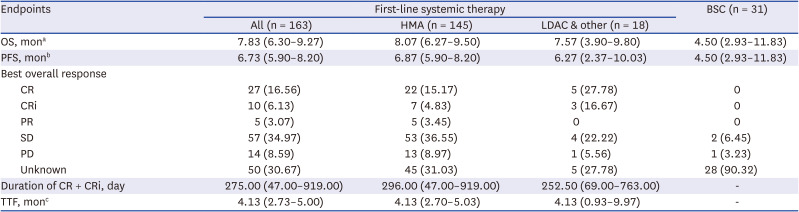
Values are presented as median (95% confidence interval), number (%), or median (range).
BSC = best supportive care, CR = complete remission, CRi = complete remission with incomplete hematologic recovery, HMA = hypomethylating agent, LDAC = low-dose cytarabine, OS = overall survival, PFS = progression-free survival, PR = partial response, PD = progressive disease, SD = stable disease, TTF = time to treatment failure.
aThirty-seven patients with missing data; bForty-two patients with missing data; cFifty-two patients with missing data due to lost to follow-up.
Fig. 1
Kaplan-Meier analysis of OS in patients who received HMA, LDAC and other systemic therapies, or BSC. Patients with missing data across all groups, n = 37.
BSC = best supportive care, CI = confidence interval, HMA = hypomethylating agent, LDAC = low-dose cytarabine, OS = overall survival.
aLog-rank test by comparing between three groups; bWilcoxon test by comparing between three groups; cLog-rank test by comparing between the HMA and BSC groups; dLog-rank test by comparing between the LDAC & other systemic therapies and BSC groups.
Subgroup analyses showed that median OS was significantly different (all P < 0.01) between patients without (8.20 months) vs. with (4.73 months) secondary AML, patients with an ECOG performance status of 0 or 1 (8.30 months) vs. ≥ 2 (4.43 months), patients with favorable (10.67 months) vs. intermediate (6.13 months) and poor (6.32 months) cytogenic risk, and patients with CCI of 0 (8.30 months) vs. ≥ 1 (5.73 months; Supplementary Table 4).
Using Cox regression analyses, we identified several prognostic factors for OS, including presence of secondary AML (hazard ratio [95% CI], 1.67 [1.13–2.45]; P = 0.009), ECOG performance status ≥ 2 (2.41 [1.51–3.83]; P < 0.001), intermediate (1.77 [1.10–2.84]; P = 0.018) or poor (2.10 [1.36–3.24]; P < 0.001) cytogenetic risk, and CCI ≥ 1 (2.26 [1.43–3.58]; P < 0.001; Table 3).
Table 3
Prognostic factors that affect overall survival
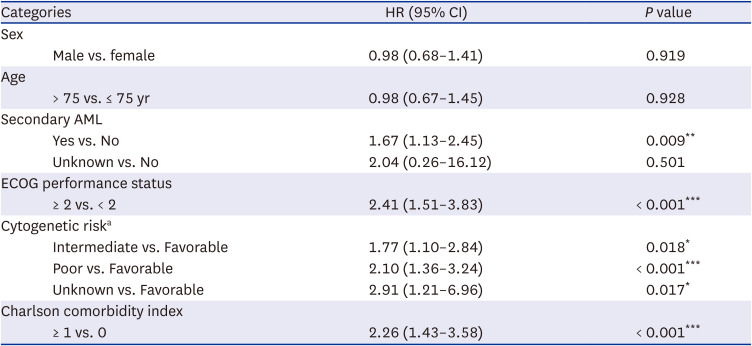
AML = acute myeloid leukemia, CI = confidence interval, ECOG = Eastern Cooperative Oncology Group, HR = hazard ratio.
*P < 0.05, **P < 0.01, ***P < 0.001.
aRisk stratification according to the cytogenetic risk classification described in Supplementary Table 3.
Secondary endpoints
Median (95% CI) PFS was 6.73 (5.90–8.20) months for patients who received systemic therapy (HMAs, 6.87 [5.90–8.20] months; LDAC and other systemic therapies, 6.27 [2.37–10.03] months), and 4.50 (2.93–11.83) months for patients who received BSC (Table 2, Supplementary Fig. 3). Median (95% CI) TTF was 4.13 (2.73–5.00) months for patients who received systemic therapy (HMAs, 4.13 [2.70–5.03] months; LDAC and other systemic therapies, 4.13 [0.93–9.97] months; Table 2). The number of patients with missing data for PFS and TTF was 42 and 52, respectively. Among the 163 patients who received systemic therapy, 37 (22.7%) achieved CR or CRi, with a median (95% CI) DoR of 275.00 (47.00–919.00) days (Table 2). CR or CRi was achieved in 20.0% of patients who received HMAs and 44.4% of patients who received LDAC and other systemic therapies, with a corresponding median (95% CI) DoR of 296.00 (47.00–919.00) and 252.50 (69.00–763.00) days, respectively (Table 2).
Subgroup analysis showed that median PFS was significantly different between patients without vs. with secondary AML (7.37 months vs. 4.68 months; log-rank test P = 0.013; Wilcoxon test P = 0.017), patients with ECOG performance status 0 or 1 vs. ≥ 2 (7.23 months vs. 4.20 months; log-rank test and Wilcoxon test P < 0.001), patients with favorable vs. intermediate and poor cytogenic risk (8.37 months vs. 5.77 months and 6.23 months; log-rank test P < 0.001; Wilcoxon test P = 0.004), and patients with CCI of 0 vs. ≥ 1 (7.27 months vs. 5.73 months; log-rank test P = 0.003; Wilcoxon test P = 0.008; Supplementary Table 5).
Using Cox regression analyses, we identified several factors associated with PFS, including presence of secondary AML (hazard ratio [95% CI], 1.58 [1.08–2.33]; P = 0.019), ECOG performance status ≥ 2 (2.25 [1.40–3.62]; P < 0.001), poor cytogenetic risk (1.96 [1.27–3.04]; P = 0.003), and CCI ≥ 1 (2.01 [1.28–3.16]; P = 0.003; Supplementary Table 6).
DISCUSSION
In the overall CURRENT study population, HMAs were associated with longer median OS, PFS, and TTF, compared with other systemic therapies or BSC.7 This subanalysis revealed similar survival outcomes among the study’s Korean subpopulation. We also found that several patient demographic and genetic factors were associated with OS and PFS.
Survival outcomes among all patients in this Korean subanalysis were poor. Median OS was higher in patients who received systemic therapy (7.83 months) compared with those who received BSC (4.50 months), although this was not statistically significant. Notably, median OS was highest in patients who received HMAs (8.07 months). Survival outcomes in patients receiving HMAs were largely consistent with previous reports in clinical trials181920 and real-world studies21 (median OS, 6.6–10.4 months). In line with previous studies and the overall CURRENT study,17 this subanalysis highlights the preference for HMAs in patients who are ineligible to receive ICT, which was not surprising given the favorable survival outcomes associated with HMAs compared with other available therapies. Median OS for the HMA cohort in this subanalysis closely mirrored that of a systematic review and meta-analysis of the efficacy and safety of decitabine in the treatment of elderly patients with AML (n = 718; median [95% CI] OS, 8.09 [5.77–10.41] months).22 Notably, 85.9% of patients in the present subanalysis received decitabine as first-line systemic therapy. In contrast to our results, a US study reported a median (95% CI) OS of 4.30 (3.20–5.80) months in patients treated with HMAs.23 Furthermore, median OS in the LDAC and BSC cohorts were slightly longer than reported previously.19 These differences may be explained by the present population being more representative of real-world clinical practice and comprising only Korean patients. The BSC cohort in the Korean subpopulation also had a longer median OS compared with the BSC cohort in the global population of the CURRENT study. This may be due to a smaller proportion of the BSC group in the Korean subpopulation (29%) having poor or intermediate cytogenetic risks compared with the global population (56%). In addition, the quality of medical care in South Korea and high medical accessibility24 may play a role in the longer median OS observed in the BSC group in the Korean subpopulation compared with that in the global population. When evaluating OS in patient subgroups, we found that those diagnosed with vs. without secondary AML, with an ECOG performance status ≥ 2 vs. 0 or 1, with poor or intermediate vs. favorable cytogenetic risk, or with CCI ≥ 1 vs. 0 had a shorter median OS. Similar observations have been reported in previous studies.15252627
Median PFS in this subanalysis was higher in patients who received systemic therapy (6.73 months) compared with patients who received BSC (4.50 months), although this was not statistically significant. Notably, median PFS was highest in patients who received HMAs (6.87 months), which is consistent with the global CURRENT study.17 Evaluation of PFS according to patient subgroups revealed that patients diagnosed with vs. without secondary AML, with an ECOG performance status ≥ 2 vs. 0 or 1, with poor or intermediate vs. favorable cytogenetic risk, or with CCI ≥ 1 vs. 0 had shorter median PFS. These results are consistent with previous studies in which poor ECOG performance status and comorbidity index scores were associated with shorter median PFS.25
Median TTF was comparable between all patients receiving first-line systemic therapies, which is in contrast to the overall CURRENT study in which longer median TTF was reported in patients who received HMAs.17 CR and CRi rates were lower in patients who received HMAs compared with LDAC and other systemic therapies, which is consistent with results from the CURRENT study.17 On the other hand, median duration of CR and CRi were higher in patients who received HMAs compared with other systemic therapies, which was not observed in the main study.17
Baseline characteristics of Korean patients in this subanalysis were generally consistent with the global CURRENT study.17 The vast majority of patients reported comorbidities, and patients who received HMAs were more likely to report ECOG performance status < 2 with favorable or intermediate cytogenic risk, compared with patients who received LDAC and other systemic therapies, or BSC. Despite the requirement of ineligibility for ICT, there were patients with favorable risk, as well as younger patients (< 75 years old), who were enrolled in the CURRENT study; based on a review of individual CRFs (data not shown), key reasons for ineligibility for ICT in this Korean subanalysis were old age, poor ECOG performance status, and/or presence of comorbidities. The mutation rate in this subanalysis among patients who received systemic therapies was 34.0%; the most frequently occurring mutations reported here and in the CURRENT study17 were NPM1 and FLT3ITD, confirming findings from previous studies.282930 In addition, we found that there was a significant difference between median age, proportion of male patients, and the proportion of patients aged > 75 years for the HMA, LDAC and other systemic therapies, and BSC groups. Fewer patients in the systemic therapies groups vs. the BSC group were > 75 years of age (which is the cut-off value shown to define unfitness for ICT in AML3132), indicating that patients in this subanalysis who received systemic therapies may have had a better prognosis,33 although age was not found to be a significant prognostic factor for survival in this Korean subanalysis.
Factors associated with poorer OS and PFS included secondary AML, ECOG performance status ≥ 2, intermediate or poor cytogenetic risk, and CCI ≥ 1. This is consistent with a multicenter trial in which better performance status, non-adverse cytogenetics, and lower CCI scores were associated with better survival outcomes in patients with AML who were ineligible for ICT and received decitabine as first-line treatment.34 In addition, retrospective, longitudinal cohort study of Korean patients with AML showed that secondary AML was associated with poorer survival outcomes.35 Better performance status was similarly found to be prognostic for survival in Korean patients with AML.3637 This may have influenced the outcomes of patients in our study, in which 75% of patients in the HMA group had ECOG performance status < 2 compared with just 55.6% and 48.4% in the LDAC and other systemic therapies and BSC groups, respectively. In contrast to our results, a study of 248 elderly patients on low-intensity therapy did not find an association between survival and ECOG performance status or cytogenetic risk, but identified response to the first induction cycle and lactate dehydrogenase levels as prognostic parameters,33 neither of which were examined in our study. With regard to treatment with HMAs, patients with DNA methylation-related mutations have improved OS, and TET2 mutation has been recognized as an independent prognostic factor for PFS.38 In this subanalysis, TET2 mutation was identified in 18.2% of patients in the HMA cohort, whereas none of the patients in the other treatment groups had this mutation. Overall, the prognostic parameters associated with median OS and PFS in our study were consistent with those reported in patients who received ICT.2039404142
Finally, we have shown that more patients who were ineligible for ICT received HMAs compared with LDAC and BSC, which is consistent with the CURRENT study.17 Regardless, survival was poor among all patients. Studies investigating outcomes in patients who received HMA compared with ICT have found that HMA was more frequently used in older patients, despite better outcomes with ICT, even in those with comorbidities.2123 Conversely, two recent analyses of elderly patients (≥ 65 years) with AML in Korea noted that despite lower response rates in patients who received HMAs compared with those who received ICT, survival outcomes were comparable.4344 Other studies involving elderly patients with AML have also reported comparable or better survival outcomes for those who received HMAs compared with those who received ICT or palliative care.45 Notably, there were patients in this subanalysis who received only palliative BSC despite the availability of first-line systemic therapies. Given that baseline characteristics, except for age, were largely consistent between the first-line systemic therapy and BSC groups, it may be that BSC is considered for elderly patients because age is regarded as a critical factor when making treatment decisions. There remains a significant unmet need for higher efficacy treatments for patients who are ineligible for ICT owing to advanced age. Although targeted treatments have been associated with a moderate improvement in outcomes for patients unfit for ICT,464748495051 prognosis remains poor and there is a lack of consensus regarding optimal treatment for these patients.
Several limitations should be considered when interpreting the results of this study. As with all real-world retrospective studies, the CURRENT study was uncontrolled and nonrandomized. As this was a retrospective, real-world, chart review, there were some missing data that may limit interpretation; missing molecular and cytogenetic data may limit assessment of their effect on outcomes, and missing response rate data for > 30% of patients who received systemic therapies may limit the generalizability of these findings. There are many systemic therapies included in the “other systemic therapy” group of this study, which may limit interpretation of the clinical outcomes of patients who received each of these therapies. Intra- and inter-site variability may exist, but to reduce variations and the need for corrections in the data collected, we optimized and ensured the clarity of the electronic CRF, and provided all study sites with adequate training. Due to the retrospective nature of this study, adverse events following previous treatment were not collected in the CRF.
In conclusion, this subanalysis of the real-world CURRENT study provided several insights into the clinical management of Korean patients with AML who are ineligible for ICT. The clinical outcomes for this Korean subgroup are poor, with a median OS < 10 months in patients who received systemic therapy and < 5 months in patients who received BSC. The majority of Korean patients with AML who are unfit for ICT receive HMAs, which are associated with numerically longer median OS and PFS relative to other systemic therapies and BSC. Factors such as secondary AML, ECOG performance status, cytogenetic risk, and CCI may be prognostic for survival. Given the rising incidence of AML due to the aging population, there is a substantial unmet need for novel therapies and combination regimens to improve clinical outcomes in this patient population.
 XML Download
XML Download