

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Pneumonia is a common infectious disease with a high disease burden among children. Moreover, it is a leading infectious cause of death worldwide, particularly among children under the age of 5.1 In the United States, the annual incidence of pneumonia requiring hospitalization was estimated to be 15.7/10,000 children in 2010–2012, and pneumonia was the most common reason for hospitalization among children in 2011.23 In South Korea, approximately 40,000 children visited the emergency department annually between 2007 and 2014, but the number of patients widely varied by season.456
To adequately manage this important infectious disease in children, identifying pathogens is a critical but challenging task. Clinical symptoms and radiographic findings may sometimes not be helpful for differentiating upper and lower respiratory tract infections (URTIs/LRTIs), and clinical specimens such as blood, sputum, nasopharyngeal swab/aspirate (NPS/NPA) may not represent the actual infection site in pneumonia. In addition, some pathogens may colonize the upper respiratory tract (URT) without inducing any symptoms, particularly in infants and toddlers.7 Therefore, it is important to study the contemporary and regional epidemiological and etiological characteristics of pediatric community-acquired pneumonia (CAP), applying accurate diagnostic criteria to guide the adequate management of CAP in children.
In South Korea, some retrospective studies on the proportion of respiratory pathogens detected in pediatric pneumonia have been performed.45 In addition, a nationwide prospective etiologic study of CAP in children was recently performed.6 However, all clinical studies of CAP among children thus far have had substantial limitations, particularly regarding the completeness of the etiologic work-up and the appropriateness of its interpretation. In addition, the etiology of CAP in children is likely to change after the coronavirus disease 2019 (COVID-19) pandemic.8 In this study, we aimed to identify the etiologic distribution and clinical characteristics of CAP requiring hospitalization in Korean children during the 5 years before the COVID-19 pandemic.
METHODS
Study design
Children aged 18 years or younger who were hospitalized with a diagnosis of CAP at four referral hospitals in South Korea (Seoul Metropolitan Government-Seoul National University Boramae Medical Center, Chung-Ang University Hospital, Seoul National University Bundang Hospital, and Seoul National University Children’s Hospital [SNUCH]) from March 2015 to February 2020 were included in this study. We collected the demographic data of the enrolled study subjects and clinical information of the CAP cases, including laboratory results, treatments, and outcomes. After review by each site’s Institutional Review Board, this study was exempted from the informed consent requirement due to its retrospective nature.
The enrollment procedure of the study subjects was as follows (Supplementary Fig. 1): first, all children with an administrative diagnostic code including the word ‘pneumonia’ and with a description of ‘infiltration,’ ‘nodule,’ or ‘consolidation’ in chest radiography (CXR) were searched. After excluding duplicates and cases of hospital-acquired infections, we selected cases with obvious pneumonic infiltration on CXR through an interpretation of the entire radiologic report and CXR itself if needed. Then, cases in which the actual diagnosis was suspected to be bronchiolitis or ventilator-associated pneumonia were excluded through a retrospective chart review. Finally, we reconfirmed the cases that satisfied the clinical definition of pneumonia, which was 1) acute systemic and/or respiratory symptoms, such as fever, cough, sputum, chest pain, tachypnea, and dyspnea, 2) rales/crackles or evidently decreased lung sounds, and 3) CXR findings of pneumonic infiltration and/or pleural effusion (PE).9
This study included children with an underlying medical condition (UMC), a pre-existing chronic illness requiring ongoing medication and/or regular medical attention. Preterm birth at ≥ 34 weeks of gestation and completely solved medical/surgical problems were excluded from this definition. Preterm birth was considered a UMC only for infants and children younger than 2 years of age. This study defined clinically notable postinfectious bronchiolitis obliterans (PIBO), which was diagnosed by clinical symptoms/signs and then computerized tomography (CT) scan, and death as poor outcomes.
Laboratory testing for pathogen detection
Laboratory tests for the etiologic diagnosis of pneumonia were conducted using standard techniques in each hospital based on their institutional practice protocol and/or the corresponding clinician’s decision. The results of laboratory tests were included for analysis only when the clinical specimen was obtained within 3 days before or after admission, except PE and bronchoalveolar lavage (BAL), which were included if performed within 2 weeks of presentation. In this way, pyogenic bacteria were regarded as detected if they grew in cultures of blood, PE, or BAL fluid. In addition, a positive result in the Streptococcus pneumoniae urinary antigen test performed on PE was also regarded as etiologic detection.
As atypical bacterial pathogens, Mycoplasma pneumoniae, Chlamydophila pneumoniae, Chlamydophila trachomatis, and Legionella pneumophilia were detected from respiratory specimens such as NPS, NPA, sputum, and BAL fluid by using polymerase chain reaction (PCR), although PCR was not uniformly performed at each site. For M. pneumoniae, the results of serologic tests were also used. Serologic diagnosis for M. pneumoniae infection was primarily made by a 4-fold increase in antibody titers between the acute and convalescent stages. When only one serologic test result was available, we regarded M. pneumoniae as detected if the titer was ≥ 1:640 in an indirect agglutination test (IAT)10 or its equivalent in another serologic test platform.
Respiratory viruses were detected from respiratory samples by using multiplex reverse-transcriptase quantitative polymerase chain reaction (mRT-qPCR) using different commercial or in-house kits between study sites. Targeted viruses were adenovirus (AdV), influenza virus (Flu), human metapneumovirus (HMpV), parainfluenza virus (PIV), respiratory syncytial virus (RSV), human rhinovirus/enterovirus (HRV), human bocavirus (HBoV), and seasonal human coronavirus (HCoV). In this study, HRV, HBoV, and HCoV were excluded from the analysis because these viruses can often be detected even in asymptomatic children, and thus, the significance of their detection from respiratory specimens is still not evident, particularly in children.111213 For some patients, the results of antigen detection tests for RSV and Flu from respiratory specimens were used.
Statistical analysis
All statistical analyses were performed using SPSS version 25.0 (IBM Corp., Armonk, NY, USA). Pearson’s χ2 test and Fisher’s exact test were used to compare categorical variables. The Mann–Whitney or Kruskal–Wallis test was used for nonparametric analysis, and the results are expressed as medians and interquartile ranges (IQRs). Differences across study sites and etiologic groups were tested by using a Wilcoxon rank test. All tests were two-sided, and a P value of < 0.05 was considered statistically significant.
RESULTS
Demographic and clinical characteristics of children with CAP
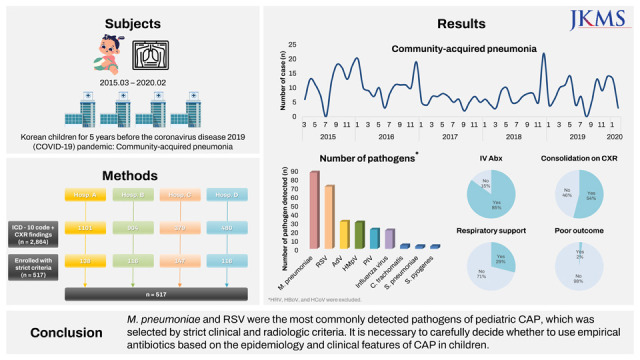
A total of 2,864 pneumonia cases were collected by diagnosis code and keywords indicating pneumonia on CXR findings in four hospitals during the five consecutive epidemic seasons. Then, 517 cases (18.1%) among 489 patients were selected, excluding nosocomial infections or cases without evident pneumonic infiltration (Supplementary Fig. 1). Among the 489 patients, 25 (5.1%) patients were admitted 2 times, 3 patients 3 times, and 1 patient 4 times during the study period. Male patients accounted for 48.1%, and the median age at admission was 3 years (8 days to 18 years). Among the patients, 79 (15.3%) were under 1 year of age, 222 (42.9%) were between 1 and 4 years of age, 174 (33.7%) were between 5 and 11 years of age, and 42 (8.1%) were between 12 and 18 years of age (Table 1). Twenty-nine percent (n = 149) had a UMC, among which preterm birth (< 34 weeks of gestational age) was the most common at 20.8%, followed by neuromuscular (18.1%) and genetic diseases (14.1%).
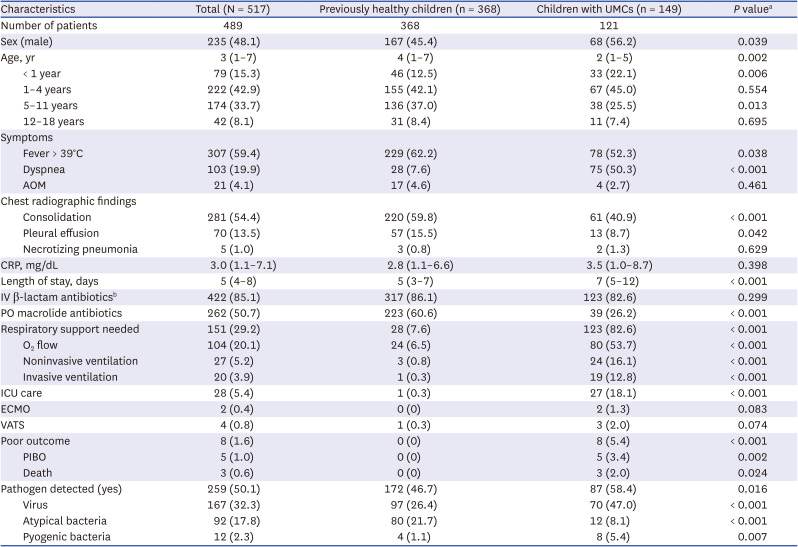
Table 1
Demographic and clinical characteristics of children hospitalized with community-acquired pneumonia in four referral hospitals, 2015–2020
All categorical variables are presented as numbers (percentages) except the total number of patients enrolled, and continuous variables are presented as medians (interquartile ranges).
UMC = underlying medical condition, AOM = acute otitis media, CRP = C-reactive protein, IV = intravascular, PO = per oral, ICU = intensive care unit, ECMO = extracorporeal membrane oxygenation, VATS = video-assisted thoracic surgery, PIBO = postinfectious bronchiolitis obliterans.
aPearson’s χ2 test or Fisher’s exact test for categorical variables, and Mann–Whitney or Kruskal–Wallis test for nonparametric analysis. bOnly among patients without acute otitis media.
![]()
A high fever (defined as ≥ 39°C) and dyspnea were present at admission in 59.4% and 19.9% of patients, respectively. Acute otitis media (AOM) was present in 4.1% of children, and the median C-reactive protein (CRP) concentration at admission was 3.0 mg/dL. On the initial CXR, consolidation and PE were present in 54.4% and 13.5% of patients, respectively. Five (1.0%) patients were diagnosed with necrotizing pneumonia on the initial and/or follow-up CT scan. The median duration of hospitalization was 5 days. Among children with CAP but not AOM, 85.1% were administered parenteral β-lactam antibiotics, and oral macrolide antibiotics were used for 50.7% of the total subjects. Respiratory support was applied for 29.2%, including invasive mechanical ventilation for 3.9%, and 28 patients (5.4%) were managed in the intensive care unit (ICU). Almost all patients recovered without sequelae, but five patients had clinically notable PIBO as a complication, and three patients ultimately died (Table 1).
Previously healthy children were admitted with a high fever (62.2%) and radiographic findings of consolidation (59.8%) and/or PE (15.5%) and received macrolides (60.6%) more often than children with a UMC (P < 0.001 for all except PE [P = 0.042]). Children with a UMC presented with dyspnea (50.3%), needed respiratory support (82.6%) and ICU care (18.1%), and had poor outcomes (6.0%) more often than healthy children (P < 0.001 for all). All patients who died were immunocompromised (primary immune deficiency or oncologic disease). Nevertheless, the initial concentration of CRP was comparable, and parenteral β-lactam antibiotics were used with similar frequencies in both groups (Table 1).
Distribution of detected pathogens
Pathogens were detected in 50.1% (n = 259) of CAP patients hospitalized in four hospitals during 2015-2020. Respiratory viruses were detected in 32.3% (n = 167), atypical bacteria in 17.8% (n = 92), and pyogenic bacteria in 2.3% (n = 12). Coinfection of respiratory pathogens was encountered in 19 (3.3%) cases, including one case of pyogenic and atypical bacteria, 10 cases of atypical bacteria and one virus, one case of atypical bacteria and two viruses, and 7 cases of two viruses. The frequency of admission with CAP was highest during every winter season (except 2018/2019), which was induced by both viral and atypical bacterial respiratory pathogens (Fig. 1).

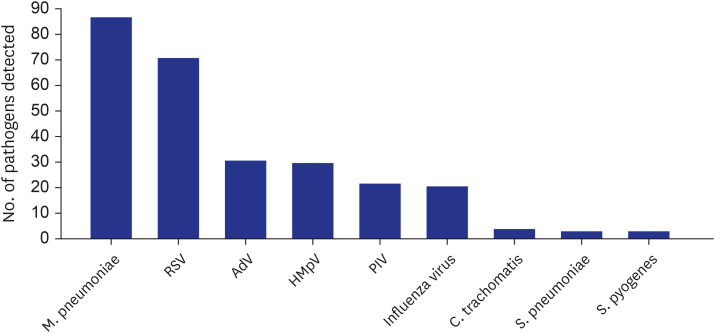
As an individual pathogen, M. pneumoniae was the most frequently identified (n=87, 16.8%). Other atypical bacteria detected were C. trachomatis (4 cases) and C. pneumoniae (1 case). The second most common single pathogen detected was RSV (n = 71, 13.7%), followed by AdV (n = 31, 6.0%), HMpV (n = 30, 5.8%), PIV (n = 22, 4.3%), and Flu (n = 21, 4.2%) (Fig. 2). Among pyogenic bacteria, S. pneumoniae and Streptococcus pyogenes were most commonly detected, each in 3 cases.
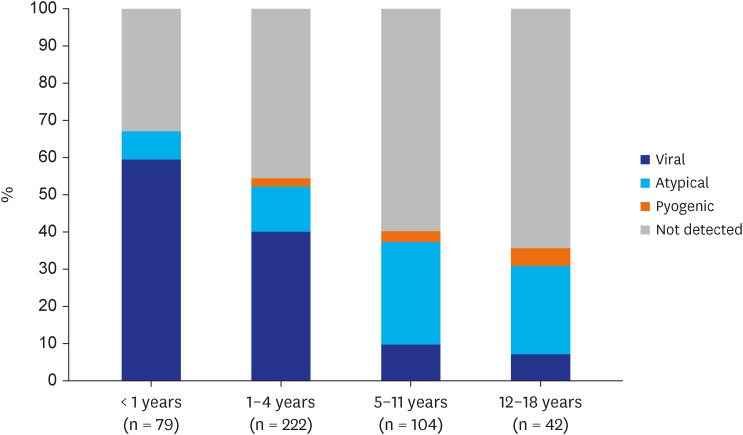
According to age group, the proportion of viral CAP was high among infants (59.5%) and children aged 4 years or younger (40.1%) but rare among adolescents (7.1%). The proportions of both atypical bacterial CAP and CAP with no pathogen detected were high in the 5–11 (27.6% and 59.8%, respectively) and 12–18 years (23.8% and 64.3%, respectively; Fig. 3) age groups. Previously healthy children were more frequently diagnosed with atypical bacterial CAP (21.7%; P < 0.001), but children with a UMC were diagnosed with viral (47.0%; P < 0.001) and pyogenic bacterial (5.4%; P = 0.007) CAP more often (Table 1).
DISCUSSION
In this study, the etiologic distribution and clinical characteristics of CAP in Korean children with or without UMC for 5 years before the COVID-19 pandemic were investigated through an intensive selection procedure for evident pneumonia and strict criteria for the positive results of the etiologic tests. As a result, the detection rate of M. pneumoniae was the highest, followed by RSV, and the incidence of pyogenic bacterial CAP was very low at 2.3%. Nevertheless, most and half of hospitalized children with CAP received parenteral β-lactam and oral macrolide antibiotics, respectively. In addition, even though life-supporting management such as mechanical ventilation and ICU care and poor outcomes such as PIBO and mortality were mostly encountered among children with underlying medical conditions, parenteral antibiotics were used for previously healthy children with CAP with a similar frequency.
Pneumonia is known to be one of the most common causes of hospitalization among children. The main reasons for hospitalization might be the need for close monitoring of respiratory distress and secondary complications, respiratory support, and parenteral antibiotic treatment. The diagnosis of pneumonia is also a common reason for the use of oral antibiotics in the outpatient clinic. However, in many studies, even those from developed countries, a substantial proportion of CAP is caused by respiratory viruses, whereas the proportion of pyogenic bacterial pneumonia is relatively small.214 Nevertheless, empirical β-lactam antibiotics are widely used due to the limitations in diagnosing the causative bacteria of pneumonia in clinical practice.15
Accurate clinical diagnosis of pneumonia is not always easy. Of course, if there are clear CXR findings indicative of pneumonia, such as lobar consolidation and a moderate amount of PE, with acute onset of respiratory symptoms and abnormal auscultation, pneumonia should be evident, and even the possibility of a pyogenic bacterial etiology might be high. However, in many clinical situations, CXR shows nonspecific findings, such as peribronchial or parahilar infiltrations on the nonfully inspired lungs of infants and toddlers. In addition, rales/crackles, which are known to be an indicative auscultation finding of pneumonia, could also be accompanied by viral bronchiolitis. These limitations cause pneumonia to be overdiagnosed and thus antibiotics to be overused. Furthermore, in many clinical studies conducted without this distinction being clear, the proportion of viruses as the etiology of pneumonia may appear larger than in reality. In the current study, as a result of applying very strict pneumonia diagnosis criteria, only 18% of cases with a pneumonia diagnosis and/or CXR findings of pneumonic infiltrations were selected among all clinically diagnosed pneumonia cases. It is assumed that a large number of acute respiratory tract infections have been misdiagnosed as pneumonia and thus resulted in hospitalization.
Additionally, in the etiologic diagnosis of pneumonia, many special considerations are required for the appropriate interpretation of radiographic and laboratory tests. Since it is almost impossible to collect samples from the lung parenchyma itself, the specific pathogen is assumed to be present primarily based on clinical features and CXR findings in usual clinical situations or by some NPA/NPS or sputum tests. However, infants and children are not able to spit out sputum properly. As a result, the etiologic diagnosis of pneumonia is mainly performed with mRT-qPCR tests from NPA/NPS for respiratory viruses, PCR tests from NPA/NPS or serological tests for atypical bacteria, and conventional culture from blood, PE, BAL fluid or some endotracheal aspirates (ETAs) for pyogenic bacteria. Additional PCR tests, including rRNA sequencing for atypical and pyogenic bacteria and antigen testing for S. pneumoniae both from PE or BAL fluid, could also be utilized.15
However, URT specimens may not properly represent the etiology of LRTIs. For example, S. pneumoniae, the most common cause of pyogenic bacterial pneumonia, commonly colonizes in infants and young children and can be detected at any time even in healthy children without symptoms. This frequent colonization of S. pneumoniae could also induce positivity in the blood PCR and urinary antigen tests, which can be used for adults. On the other hand, when the amount of blood for culture is insufficient or antibiotics are administered before culture, the yield of the blood culture could decrease.16 Moreover, some respiratory viruses, such as HRV, HCoV, and HBoV, could also be detected in asymptomatic children due to their prolonged shedding and recurrent asymptomatic/mild symptomatic infections as well as the false positivity of PCR tests. Additionally, M. pneumoniae can be PCR positive from NPS/NPA specimens of asymptomatic children depending on the epidemic period and country,17 and serological tests have even more limitations. Two blood samplings in both acute and convalescent periods are not practical, and the immunoglobulin M (IgM) test is known to be positive for a very long time and thus cannot reliably differentiate acute and previous infection.1718
The proportions of CAP etiologies among children have been widely reported depending on country, period, and age group.2141920 This also largely depends on which tests are used for the identification of each causative organism and at what level the results are accepted as positive. To determine the more accurate distribution of CAP etiologies among Korean children, only respiratory viruses known to be meaningful from NPS/NPA specimens were included, and PCR detection and serological test results of at least a 4-fold increase or a higher single antibody titer corresponding to 1:640 of IAT were considered for M. pneumoniae in the current study. For pyogenic bacteria, the possibility of detection of colonizers was aggressively excluded. As a result, more than one pathogen was detected in only half of CAP cases, comprising respiratory viruses in 32.3%, atypical bacteria in 17.8%, and pyogenic bacteria in 2.3%. These proportions were much lower than those of recent etiologic studies in the US, except for M. pneumoniae.214 In these multicenter prospective studies, any pathogen was detected in 65–81% of patients, including viruses in 56–73%, atypical bacteria in 8–9%, and pyogenic bacteria in 4–7%. This might be partly because they used more rigorous etiologic workups, including serologic tests for viruses and/or blood PCR for pyogenic bacteria. On the other hand, recent retrospective and prospective multicenter etiologic studies in South Korea reported a much higher proportion of M. pneumoniae at 29.6% and 41.3%, respectively.56 This is probably due to the low specificity of serologic tests for M. pneumoniae.
The number of children hospitalized with CAP and the detection frequency of both respiratory viruses and atypical bacteria were highest in the winter season during the current study period. This shows that RSV and M. pneumoniae have a large effect on hospitalization for CAP among Korean children with or without UMCs during the epidemic period almost every year.2122 Moreover, there was also an annual increase in the number of CAP hospitalizations in March–May and September–October, which are early school opening periods, and the lowest annual prevalence of CAP admissions during the summer vacation season. This suggests that the circulation of respiratory pathogens in schools also largely affects the occurrence of CAP among children. In this regard, large changes in the epidemiology of CAP in children might have occurred during the COVID-19 pandemic and even thereafter. We should note these changes to properly respond to new CAP epidemics among children.
In addition to RSV, other respiratory viruses, such as AdV, HMpV, PIV, and Flu, were commonly detected and induced the year-round prevalence of CAP among children. Regarding atypical bacteria, it is noteworthy that the proportion of C. trachomatis was relatively high. Because diagnostic PCR testing for C. trachomatis was performed only in the selected cases and hospitals, there might be more cases where a diagnosis was not made and improved by the use of empirical macrolide antibiotics. It is also noteworthy that the detection frequency of S. pyogenes was as high as that of S. pneumoniae among pyogenic bacteria. The influence of H. influenzae, which has been classically thought to be a major bacterial etiology, or S. aureus, which has recently been detected frequently in CAP, did not appear in the current study.
Toddlers aged 1–4 years and children aged 5–11 years comprised more than three quarters (76.6%) of all children hospitalized with CAP during the study period. The frequencies of dyspnea (19.9%) as an initial symptom and CXR findings of consolidation (54.4%) and PE (13.5%) were relatively low considering that all CAP cases were hospitalized in a referral hospital. Moreover, these proportions were even lower among previously healthy children. However, most (85.1%) patients received parenteral β-lactam antibiotics on admission for CAP, and this proportion was comparable between children with and without UMCs. Considering the detection rates of pyogenic bacteria (2.3% in overall and 1.1% in healthy children) in the current study, the rate of antibiotic use was too high even considering the low sensitivity of the test for bacteria. Moreover, this management strategy has probably resulted in unnecessary hospitalizations for relatively mild CAP that probably has a viral or mycoplasma etiology.
In the current study, 6 of 10 children aged 5–18 years with CAP had no pathogen detected. This was probably because very strict criteria for the serologic test were used, and the PCR test was not uniformly performed for atypical bacterial pathogens, particularly M. pneumoniae. Some pyogenic bacterial pathogens may have been missed due to the low sensitivity of their etiologic detection. However, an unknown pathogen not routinely tested for could be an etiology for CAP in school-aged children and adolescents. Vigorous etiologic investigation with novel technologies is warranted for CAP in this age group.
The current study aimed to properly investigate the epidemiology and clinical characteristics of CAP in children with or without UMCs by using strict guidelines with up-to-date evidence for etiologic diagnosis. Nevertheless, this study had several limitations. First, since this was a retrospective study, the adequacy of CAP diagnosis could not be perfect even if strict criteria were applied. In addition, etiologic workups were not uniformly performed at each study site. Thus, it is possible that a number of pathogens were missed, and the effect of superinfections may have been underestimated. Furthermore, pyogenic bacterial infection may be underdetected due to the previously mentioned endogenous limitations of pneumonia etiology studies among children. It is also possible that the rates of viral and atypical bacterial CAP were also underestimated due to the exclusion of the possibly causative respiratory viruses HRV, HBoV, and HCoV, and the much higher cutoff level for the positive single serologic test titer for M. pneumoniae. In addition, this study did not include healthy controls for the detection rate of respiratory pathogens, so we could not confirm the causality of each pathogen detected in children with CAP. PIBO was not uniformly evaluated and captured for all patients; thus, the prognosis of CAP, particularly in previously healthy children, could have been underestimated. However, because we considered only PIBO with clinically notable respiratory symptoms and signs, those with these clinical features were probably evaluated with a CT scan. Finally, although this was a multicenter study, the results of this study may have been biased due to the large heterogeneity of each institution and the geographical location. Therefore, there is still a limitation in generalizing the results of this study to all institutions. Nevertheless, the proportion of a viral etiology was high even among children hospitalized in referral hospitals, and the actual rate of CAP seems to be exaggerated. The greatest importance of the results from this study is that many children with CAP can be treated without parenteral antibiotics in an outpatient setting.
In conclusion, more stringent criteria should be applied to detect actual pediatric pneumonia cases and then properly manage them. If possible, sufficient etiologic workup is recommended, and the results should be appropriately interpreted with caution. Previously healthy Korean children with CAP might initially be treated without hospitalization for parenteral antibiotic treatment unless there is a considerable clue for a pyogenic bacterial etiology, such as a very high concentration of inflammatory markers and lobar/lobular consolidation on CXR.
 XML Download
XML Download