

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Since the occurrence of coronavirus disease 2019 (COVID-19), the lives of people worldwide have undergone extensive changes.12 Especially, patients with cancer experienced difficulty with the utility of the healthcare system.3 Although physical distancing was an effective policy to prevent viral transmission,4 at some point, this led to the delay in the treatment of patients with cancer.56 This delay adversely affected their psychological health and increased anxiety levels.7 Many studies have shown that patients with cancer experience higher rates of distress and anxiety,89 and the more delay in the treatment, the higher the distress.3 Moreover, these patients experience higher psychological stress due to their fear of acquiring an infection,89 especially during a public health emergency. Patients with cancer faced many obstacles during the COVID-19 pandemic that impacted their psychological health and adherence, compliance, and the chance of receiving medical treatment on time.10
Due to the rapid and easy transmission of the COVID-19 virus, the most effective measure to be taken was physical distancing, which allowed the control of the infection to some extent.1112 However, this has greatly affected society’s mental health.13 Studies have shown unfavorable associations between these strict physical distancing measures and mental health symptoms.14 There was a two to three-fold increase in anxiety and depression due to adherence to distancing, which led to higher social isolation15 than during the pre-pandemic era, exacerbating the psychological distress faced during adherence to these measures.16 Despite all the negative effects resulting from the actions taken, and the non-ending cycle of one measure impacting the society as a whole, adherence to physical distancing was important to save people’s well-being.17
Even though physical distancing may cause loneliness or depression,181920 it can reduce the risk of infection transmission to patients with cancer. They have weakened immune systems due to their disease or treatment, which makes them more vulnerable to COVID-19 and its severe consequences.21 People are encouraged to practice physical distancing to minimize the spread of COVID-19 but to varying degrees of adherence. Previous studies2223 have shown that patients with underlying diseases, including cancer survivors, were discovered to adhere well to physical distancing measures, wearing face masks, and avoiding crowded areas. This could be due to the patients’ increased awareness of vulnerability to infection.9 Living with cancer is already a stressful and uncertain experience, and the COVID-19 pandemic has added an extra layer of burden for these patients, including fear of contracting the infection while in an immunocompromised state. Therefore, patients with cancer are more likely to protect themselves from the virus by adhering to physical distancing measures. However, there is a lack of research into how these patients specifically adhere to physical distancing during the COVID-19 pandemic and the intrapersonal decision-making processes on health-related behaviors that influence physical distancing.
The health belief model (HBM)2425 was constructed to help explain and predict health behaviors by examining people’s beliefs and attitudes about health threats and the perceived benefits of adopting health-related behaviors. The HBM suggests that health-related behavior depends on the desire to avoid illness and the belief that specific health actions will prevent illness. The model specifies that an individual’s behavior is influenced by six socio-behavioral factors26: perceived susceptibility, severity, benefits, barriers, the presence of cues to action, and self-efficacy. A recent analysis27 showed that the HBM has a good predictive ability of COVID-19 preventive behavior, including adherence to physical distancing. In this review, which included 32 studies, the perceived benefit was the most significant predictor in almost all (96.5%) studies, followed by self-efficacy (87.5%), cues to action (72.2%), perceived barrier (64%), susceptibility (59.4%), and severity (40%) in decreasing order.
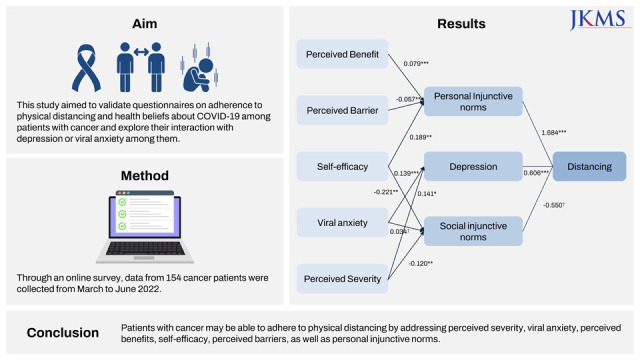
Social norms predict behavior, because people are more likely to act if they feel normative pressure.282930 Descriptive social norms refer to the typical behavior most people exhibit in a given situation. These norms are based on people’s perceptions of the behavior that is displayed. In contrast, injunctive norms refer to the behavior that is expected or required in a given situation. These indicate how people should behave and represent the norms people should follow. In previous COVID-19 prevention efforts, social norms have acted as a positive predictor for engaging in a range of health behaviors.3132 Moreover, people are more reluctant to practice handwashing, mask-wearing, and social distancing when they believe others are not practicing these behaviors. Thus, a questionnaire on adherence to physical distancing and health beliefs about COVID-19 was developed by Gouin et al.33 The Korean version of the questionnaire was validated in the general population34 and healthcare workers in Korea.35 The aim of this study was, first, to examine the reliability and validity of questionnaires on adherence to physical distancing and health beliefs about COVID-19 among patients with cancer and, second, to explore how the various sections interacted with each other and with depression or viral anxiety among these patients.
Go to : 
METHODS
Participants and procedure
We conducted an online survey between March and June 2022 at Asan Medical Center, Seoul, Korea. Participants included patients with cancer who visited the Asan Medical Center Cancer Institute and voluntarily responded to the survey delivered via a link on the poster for enrollment. We developed the survey form including questions on participants’ age, sex, marital status, cancer type, cancer stages, and current treatment modalities. In addition, we included questions on COVID-19, such as “Have you been quarantined due to COVID-19 infection?,” “Have you been infected with COVID-19?,” or “Did you get vaccinated?.” Participants were provided an e-gift coupon valued at $5 for participation. We referred to the Checklist for Reporting Results of Internet e-Surveys guidelines36 for developing the e-survey form.
Measures
Questionnaires on adherence to physical distancing, health beliefs about COVID-19, and perceived social norms
A questionnaire on adherence to physical distancing was developed by Gouin et al.33 It consists of seven items on adherence to physical distancing, 14 items on health beliefs about COVID-19, and three single items on perceived social norms. In this study, we applied the Korean version of the questionnaire.3435
1) Adherence to physical distancing
The questionnaire on adherence to physical distancing includes seven items, which can be rated on a 5-point Likert scale. A higher total score means greater adherence to physical distancing policy. Previous study showed a good fit for a two-factor model for questionnaire on adherence to physical distancing.34 Factor I focuses on individual’s daily routines and maintaining physical distancing at home, while factor II emphasized the use of masks and protective measures in public spaces.
2) Health beliefs about COVID-19 and perceived social norms
The questionnaire on health beliefs about COVID-19 consists of five subcategories: perceived susceptibility to infection (3 items), perceived severity of viral infection (3 items), perceived benefits of physical distancing (3 items), barriers to physical distancing (4 items), and self-efficacy (a single item). The questionnaire on perceived social norms related to physical distancing consists of three single items, a single item of each for descriptive social norms, personal injunctive norms or moral norms, and social injunctive norms.
Stress and Anxiety to Viral Epidemics-6 (SAVE-6) items
The SAVE-6 is an assessment tool for measuring an individual’s viral anxiety.37 It was one of the subscales of the SAVE-9 developed to measure healthcare workers’ work-related and viral anxiety.38 The SAVE-6 consists of six items which can be rated on a 5-point Likert scale ranging from 0 (never) to 4 (always). The higher the total score, the greater the level of anxiety associated with viral infection. We applied the original Korean version of the scale in this study. Cronbach’s alpha for this sample was 0.884.
Patient Health Questionnaire-2 (PHQ-2)
The PHQ-2 is a brief version39 of the PHQ-9, an assessment tool for measuring one’s severity of depression.40 It consists of nine items which can be rated on a 4-point Likert scale ranging from 0 (not at all) to 3 (nearly every day). The higher the total score, the more severe the symptoms of depression are. We applied two items from the Korean version of the PHQ-9,41 which was validated. A split-half coefficient among this sample was 0.890.
Statistical analysis
First, the construct validity and reliability of the Korean version of questionnaires on adherence to physical distancing and health beliefs were examined among patients with cancer. In this study, we performed the confirmatory factor analysis (CFA) among seven items of adherence to physical distancing and four subscales (perceived susceptibility, perceived severity, perceived benefit, and barriers) of the health beliefs questionnaire. Construct validity of the single item of self-efficacy of health beliefs and three single items of the social norms were not examined because the study focus was primarily on overall scales rather than on individual items. The factor structure for both scales was examined through CFA. In CFA, a two-factor model for the adherence to physical distancing scale and a four-factor model for the HBM scale were examined using the diagonally weighted least squares (DWLS) estimation. In this test, model fit was assessed through a comparative fit index (CFI), Tucker–Lewis index (TLI), standardized root-mean-square residual (SRMR), and root-mean-square-error of approximation (RMSEA) values.42 Multigroup CFA was performed to assess the measurement invariance of these two scales across sex. Besides, item analysis was performed for each measure. Cronbach’s alpha and McDonald’s omega were calculated to test the reliability of internal consistency. Pearson’s correlation analysis was done to explore convergent validity.
Second, we examined the interaction between the various assessments and adherence to physical distancing. To begin with, we conducted a correlation analysis using Pearson’s “r.” Based on the results, we constructed a structural equation model (SEM) in which each variable was arranged so that its effects ultimately resulted in adherence to physical distancing among patients with cancer.
We used SPSS version 21.0 (IBM Corp., Armonk, NY, USA), AMOS version 27 for Windows (IBM Corp.), JASP version 0.14.1, jMetrik 4.1.1, and R version 4.1.2 (R Foundation, Vienna, Austria) with the lavaan package to perform statistical analyses.
Ethics statement
This study was approved by the Institutional Review Board (IRB) of Asan Medical Center and the requirement for informed consent was waived (IRB 2022-0054).
Go to :
RESULTS
Demographic characteristics of patients with cancer patients in this study are presented in Table 1.
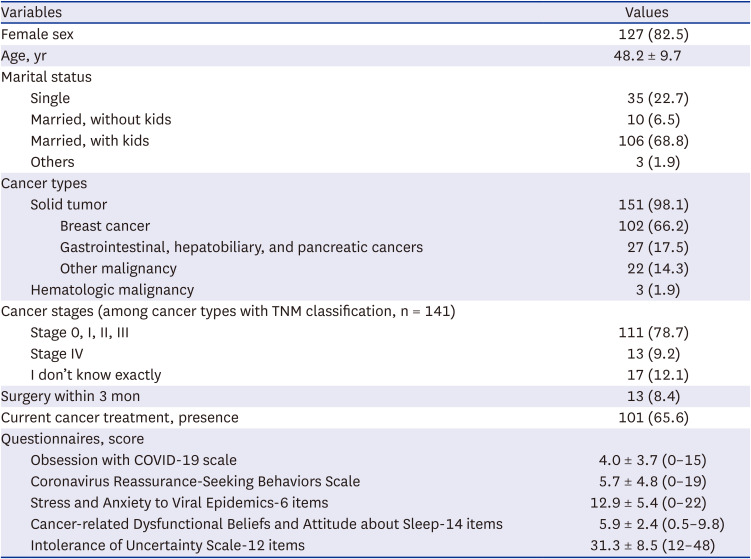
Table 1
Demographic and clinical characteristics of patients with cancer (n = 154)
Values are presented as number (%) or mean ± standard deviation.
TNM = tumor, node, metastasis, COVID-19 = coronavirus disease 2019.
![]()
Reliability and validity of questionnaires
Factor loadings for adherence to physical distancing ranged between 0.587 and 0.917, and those for health belief about the COVID-19 scale ranged between 0.475 and 0.880 (Table 2). The CFA with DWLS estimation showed a good model fit for adherence to physical distancing (CFI = 1.000, TLI = 0.930, RMSEA = 0.000, and SRMR = 0.050) and a satisfactory model fit for health beliefs about COVID-19 (CFI = 0.978, TLI = 0.971, RMSEA = 0.061, and SRMR = 0.089) (Table 3). The multi-group CFA showed that the Korean version of both scales could assess adherence to physical distancing and health beliefs about COVID-19 in the same way across sex. Item analysis results (Table 2) showed that all the items in both scales had good corrected item-total correlation (≥ 0.4).
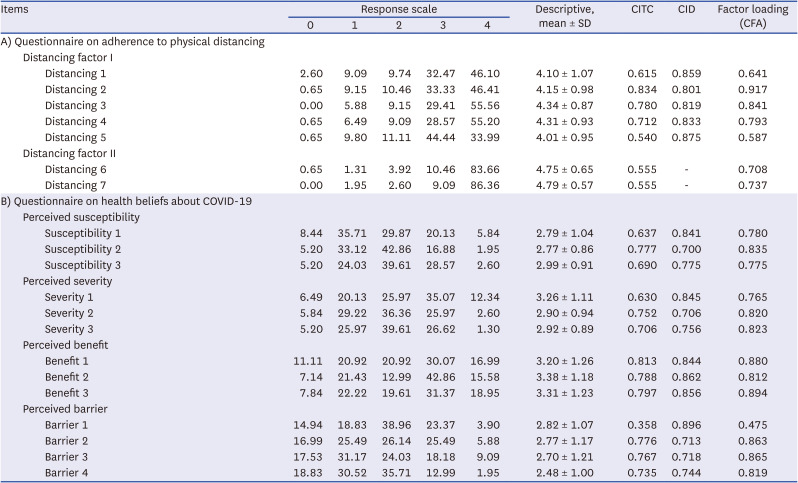

Table 2
Factor structure of the questionnaire (n = 154)
SD = standard deviation, COVID-19 = coronavirus disease 2019, CFA = confirmatory factor analysis, CITC = corrected item-total correlation, CID = Cronbach’s alpha if item deleted.
![]()
Table 3
Scale level psychometric properties of the questionnaire
COVID-19 = coronavirus disease 2019, CFI = comparative fit index, TLI = Tucker–Lewis index, RMSEA = root-mean-square-error of approximation, SRMR = standardized root-mean-square residual.
![]()
The questions on adherence to physical distancing showed good reliability for factor I (Cronbach’s alpha = 0.866) and factor II (Cronbach’s alpha = 0.709). The health beliefs about COVID-19 also showed good reliability for perceived susceptibility (Cronbach’s alpha = 0.834), perceived severity (Cronbach’s alpha = 0.831), perceived benefit (Cronbach’s alpha = 0.898), and barriers to following physical distancing (Cronbach’s alpha = 0.824). The convergent validity of each subscale with each other is presented in Table 4.
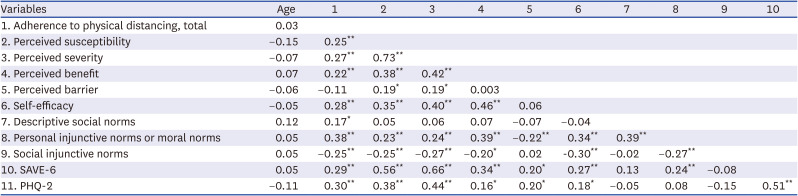
Table 4
Correlation coefficients of each variable in all participants
SAVE-6 = Stress and Anxiety to Viral Epidemics-6, PHQ-2 = Patients Health Questionnaire-2.
*P < 0.05; **P < 0.01.
![]()
SEM for adherence to physical distancing
The correlation results suggested that a three-tier model would be possible. We arranged the first tier to include the health belief variables (perceived benefit, perceived barrier, perceived severity, and self-efficacy) and viral anxiety. The second tier included two of the perceived social norms variables (personal and social injunctive norms) and depression. The last tier consisted of physical distancing only. The model was arranged so that the effects “flowed” from the first towards the last tier. Through this model, we found that personal injunctive norms were the main mediators linking health beliefs with physical distancing in patients with cancer (Fig. 1). Depression also played a role by mediating the effects of viral anxiety and the perceived severity of physical distancing. Fit measures suggested that the model was acceptable (χ2 = 20.073, df = 15, P = 0.169; CFI = 0.984; RMSEA = 0.047).
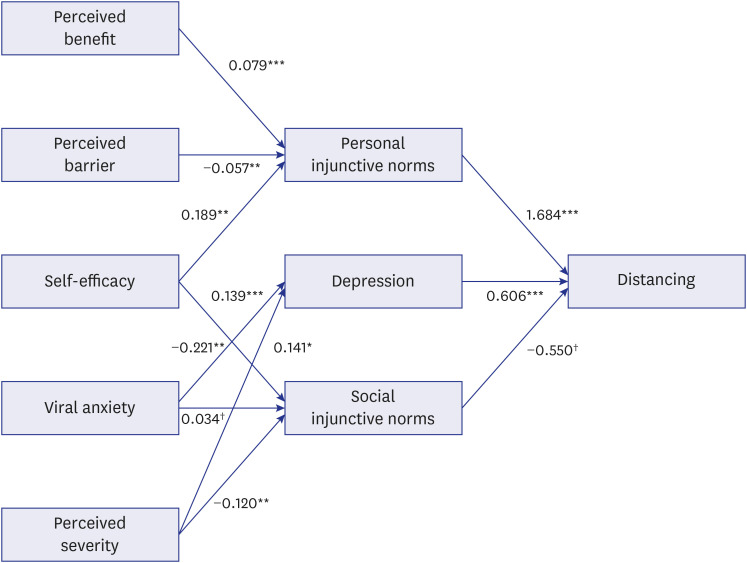 | Fig. 1Structural equation model of the variables. Numbers next to arrows correspond to standardized estimates. Structural equation model of the variables. Numbers next to arrows correspond to standardized estimates. Fit measures indicate a good fit (χ2 = 20.073, df = 15, P = 0.169; comparative fit index = 0.984; root-mean-square-error of approximation = 0.047).
*P < 0.05; **P < 0.01; ***P < 0.001; †P < 0.1.
|
Go to :
DISCUSSION
We observed that the questionnaire on adherence to physical distancing and health beliefs about COVID-19 is a scale that could assess adherence to physical distancing in COVID-19 with good reliability and validity in patients with cancer. In this study, such patients’ personal injunctive norms and depression influenced adherence to physical distancing during the COVID-19 pandemic, while social injunctive norms did not have an impact. Perceived benefit and self-efficacy positively influenced personal injunctive norms, while perceived barriers had a negative influence. Moreover, viral anxiety and perceived severity influenced depression.
Questionnaires on adherence to physical distancing were already validated in Korea among the general population34 and healthcare workers.35 This study showed a good fit for a two-factor model among patients with cancer. Questionnaires on health beliefs about COVID-19, excluding a single item of self-efficacy, showed a good model fit for the four-factor model in CFA. Undoubtedly, physical distancing during the COVID-19 pandemic has affected the psychological aspect of people in general and patients with cancer in particular. In addition, many of those people have suffered a financial crisis that increased the burden on their mental health.43 Physical distancing is a weapon of two ends; on the one hand, it was an effective way to decrease the transmission of the virus, especially among patients with cancer that were more fragile and susceptible to severe infections, conferring them the feeling of security regarding their health. On the other hand, it increased stress and loneliness in these patients who needed a great degree of psychological support. Moreover, due to the complexity of medical services during this era, patients with cancer had more difficulty accessing their treatment than before.
In the SEM, we observed that depression and personal injunctive norms in patients with cancer influenced their adherence to physical distancing. More specifically, higher levels of depression were associated with lower adherence to physical distancing. According to previous studies, the increased depression in patients with cancer due to their disease and the pandemic led to less compliance with physical distancing. In addition, a high level of viral anxiety or perceived severity may be associated with a high level of depression. Patients with have been more worried about their health and the probability of being infected by the newly emerging virus. This has led to increased anxiety about viral illness. Furthermore, anxiety has a complicated relationship with the immune system, leading to the release of cortisol, a hormone that weakens the immune system.44 This perceived severity by patients with cancer has increased their depression, leading to less compliance with physical distancing.
Personal injunctive norms are characterized as internalized moral rules that individuals follow independently of others’ expectations and influences. These norms have been found to influence adherence to physical distancing among patients with cancer. Adherence to physical distancing is further influenced by perceived benefit and self-efficacy in a positive manner, as well as by perceived barriers in a negative manner. These influences occur through the pathway of personal injunctive norms.
Patients with cancer have impaired immune function due to the disease itself and its treatment. Therefore, when these patients are aware of the seriousness of their condition, they will exhibit more adherence to physical distancing by perceiving its benefit of having a less chance of acquiring the virus. Moreover, perceived barriers to perform the recommended action of physical distancing and self-efficacy of a patient have led to more adherence, which has made healthcare settings less prone to crowding, more affordable, and less risky. These effects of health beliefs on adherence to physical distancing are mediated by personal injunctive norms. However, in this study, social injunctive norms, which were considered (in)appropriate45 did not significantly influence adherence to physical distancing among patients with cancer. Because these patients have more comorbidities and are prone to more serious infections than the general population owing to a weakened immune system, it is crucial for them to adhere to physical distancing to reduce the possibility of acquiring the infection. This was possible for them because they were already aware of their condition and were able to comply with distancing.
There are limitations to this study. First, the study was conducted in Korea among patients with cancer who attended a tertiary-level, single general hospital. Patients’ emotional states may be affected by the level of readiness and preparedness of their healthcare facility during a pandemic. Therefore, the results cannot be generalized. Second, the design of the cross-sectional, anonymous online survey was a limitation of this study. The results of this study do not suggest a causal relationship between adherence to physical distancing and any other variable such as severity of depression. In addition, responses to web-based questionnaires that are self-reported may be biased. Third, this survey was conducted between March and June of 2022; therefore, the participants might have adjusted the 2 years during which the pandemic occurred. This factor might have influenced a participant’s response to a questionnaire. Finally, the sample size comprising 154 respondents is not representative of the Korean population as a whole.
In conclusion, the Korean version of the questionnaire regarding adherence to physical distancing and health beliefs about COVID-19 is useful in assessing adherence to physical distancing and related health beliefs among patients with cancer. To achieve adherence, this study emphasizes that it is essential to address perceived severity, viral anxiety, perceived benefits, self-efficacy, perceived barriers, as well as personal injunctive norms of patients with cancer. A healthcare professional must be aware of the cultural and social factors that influence patients’ beliefs and provide appropriate education and support for patients with cancer to remain safe in this pandemic.
Go to :
 XML Download
XML Download