

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Calcifications in dental pulp tissue may be seen as diffuse calcifications or pulp stones [1]. Pulp stones are discrete calcified bodies with an organic matrix found in both the coronal and radicular parts of the dental pulp cavity. They are also found in pulp tissue or attached or embedded in dentin [2]. The radioopacity and density of the pulp stones resemble dentine. The stones include 2 essential chemical elements: calcium and phosphorus [3]. Additional elements that may be found in pulp stones are fluorine, magnesium, potassium, sodium, zinc, iron and copper [34]. In terms of their etiology, formation of pulp stones are unclear. However, some proposed factors associated with the formation of pulp stones include pulp degeneration, periodontal disease, aging, genetics, elevated oxidative stress and alkaline phosphatase in addition to deep caries and restorations, which can cause irritation and inflammation, trauma and atherosclerosis [567]. Cardiovascular diseases and kidney diseases, as well as gallstones and salivary gland stones, are potential risk factors for the formation of pulp stones [8]. However, pulp stones can be found in all age groups, irrespective of health status [910].
Pulp stones may be associated with impacted teeth. They are most commonly associated with first molars, followed by maxillary and mandibular second molars [29]. Pulp stones are least commonly associated with incisors and canines [2]. Pulp stones may make it difficult to identify root canals due to the obstruction of the root canal orifices and increase the risk of instrument fractures during endodontic therapy [11].
There is no agreement in the literature on the prevalence of pulp stones, with studies reporting a prevalence ranging from 8% to 90% [1112]. Histology-based research has noted a greater prevalence of pulp stones than radiographic research because calcified masses smaller than 200 µm cannot be detected on radiographs [21314]. The popularity of cone-beam computed tomography (CBCT) imaging in dental practice has increased, as it can generate accurate 3-dimensional images of the anatomic structures appropriate for diagnosis and treatment planning before root canal therapy [15]. According to previous research, CBCT offers a sensitive diagnostic system to detect pulp stones as compared to 2-dimensional radiographic techniques [16].
Previous studies noted a wide discrepancy in the frequency of pulp stones in various populations. According to these studies, the variations in frequency among different populations might be owing to ethnic and geographical variations [1718]. Some previous studies used CBCT to detect pulp stones in a Turkish population [817]. However, no studies have compared the prevalence of pulp stones in Turkish subpopulations according to age, sex and types/depths of coronal restorations in teeth. Hence, the aim of this study was to evaluate the presence of pulp stones using CBCT images and to correlate their prevalence with age, sex, dental arch and side, tooth type, and restoration type and depth. The null hypothesis of the present study was that there would be no significant difference in pulp stone formation between different types and depths of restorations.
MATERIALS AND METHODS
This study was performed in accordance with the guidelines of the World Medical Association Declaration of Helsinki and was reviewed and approved by the Institutional Review Board of Biruni University (2020/43-11).
Patient selection
CBCT images were obtained from 673 adult patients (363 [53.9%] females; 310 [46.1%] males) who visited Biruni University Faculty of Dentistry for routine dental care between July 2019 and December 2019 and subsequently underwent diagnostic CBCT imaging were examined retrospectively. The mean age of the participants was 38.06 ± 12.82 years (range, 18–75 years). In total, 11,494 teeth, which had already been documented in the archives of our faculty, were examined, including all types of teeth.
The case inclusion criteria were CBCT images from patients with a minimum age of 18 years in whom the roots of all permanent teeth were fully developed and there was at least one fully erupted permanent tooth in each CBCT image. As another inclusion criteria, radiopaque masses only in the coronal pulp chamber were examined. The exclusion criteria were teeth with root canal therapy, root resorption, indirect restorations, unerupted teeth and artifacts on CBCT images.
Data acquisition and validation
All the CBCT images were obtained with the patient in a standing position, using a Sirona Galileos Comfort Plus device (Dentsply Sirona, York, PA, USA), which was operated at 98 kVp and 6 mA, with a 36-s rotation time, voxel size of 250 µm and 150 × 150 mm field of view in accordance with the manufacturer's recommendations. The CBCT images were assessed using Sidexis software (Dentsply Sirona) in all 3 planes (axial, coronal, and sagittal) on a 28-inch Samsung LU28H750UQMXUF monitor (Samsung Electronics, Seoul, Korea) with a pixel resolution of 3,840 × 2,160. For optimum visualization, the brightness and contrast of the CBCT images were adjusted using the image-processing tool of the software.
Two endodontists, who had at least 5 years of experience, evaluated the CBCT images. Before the evaluation, each endodontist assessed a series of randomly chosen 50 images that were not associated with the present study for calibration between the examiners. Cohen's kappa coefficient was used to measure the agreement between the 2 examiners. The values for intra-examiner and inter-examiner consensus were excellent (0.93 and 0.91, respectively). After calibration, the observers assessed the CBCT images, and any disagreement in the evaluation was resolved through a discussion until reaching an agreement.
Image examination of pulp stones and direct restorations
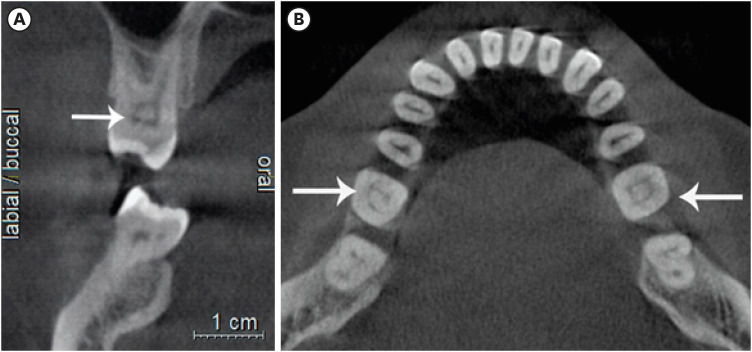
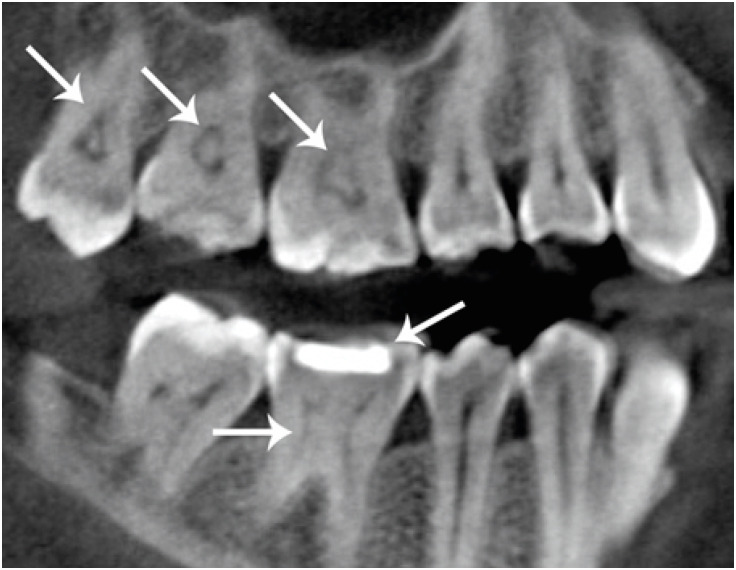
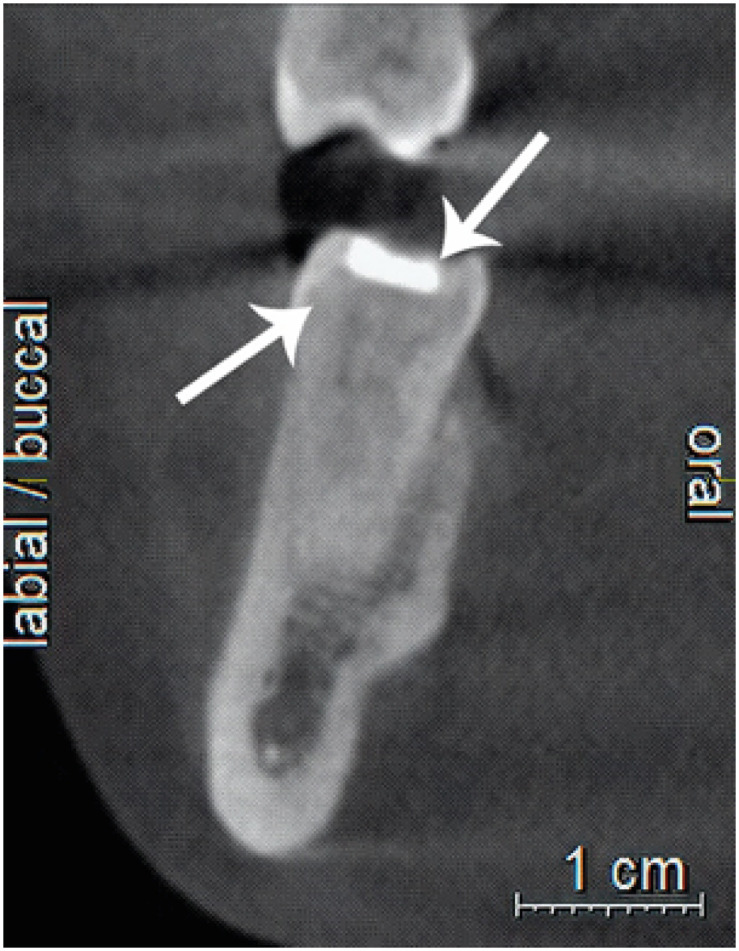
The presence of pulp stones was investigated according to age, sex, dental type and location and the presence and type (composite or amalgam) of restorations. A pulp stone was considered a clear radiopaque mass (round or oval shape) in the coronal pulp chamber (Figures 1 and 2). The depths of the restorations (shallow: up to one-third of the dentin affected; medium: one-third to two-thirds of the dentin affected; deep: two-thirds to all of the dentin affected without exposure of pulp) were also recorded according to the method described by da Silva et al. [9] (Figures 2 and 3). All the restorations were assessed in the sagittal plane, and the deepest point of the restorations was recorded.
Figure 1
Teeth with pulp stones on different sections of cone-beam computed tomography (CBCT). (A) Coronal CBCT section of maxillary first molar. (B) Axial CBCT section of mandibular first molar.
Statistical analysis
Statistical analysis was performed using IBM SPSS Statistics 22 (IBM SPSS, Istanbul, Turkey). A χ2 test was used to evaluate the number and prevalence of pulp stones according to age and sex. One sample χ2 test was used to evaluate the relationship between study parameters. Cohen's kappa coefficient was used to measure the inter-examiner agreement. The statistical significance level was set at p < 0.05.
RESULTS
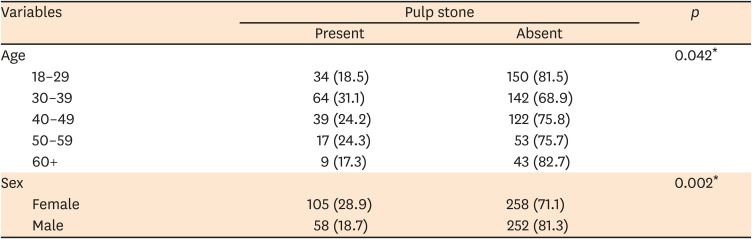
The parameters assessed in association with the presence or absence of pulp stones are reported in Table 1. One hundred and 63 patients (24.2%) had at least 1 pulp stone. Of the 11,494 teeth assessed, there were 379 (3.3%) teeth with pulp stones. In total, pulp stones were statistically higher in females than in males (28.9% vs. 18.7%, p = 0.002). In addition, the percentage of pulp stones in those aged 30–39 years (31.1%) was significantly higher than that in the 18–29 years (18.5%) and ≥ 60 years (17.3%) age groups (p1 = 0.004; p2 = 0.049) (Table 1).
Table 1
Number and prevalence of pulp stones according to age and sex (n = 673)
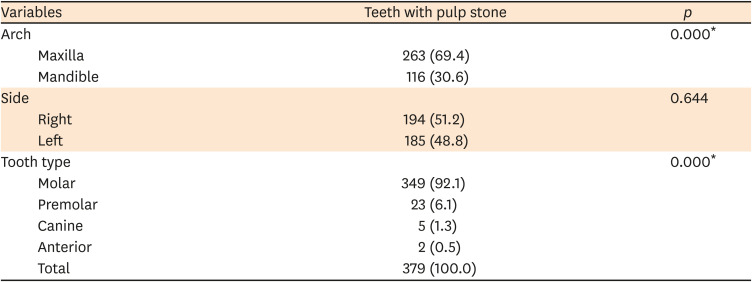
The difference in the percentage of pulp stones in the mandibular and maxillary arches was statistically significant (30.4% vs 69.4%, p < 0.05). There was no statistical significance regarding the dental arch sides (p > 0.05). In terms of tooth type, pulp stones were significantly more common in molars (92.1%) than premolars (6.1%), canines (1.3%) and anterior teeth (0.5%) (p < 0.05). In addition, pulp stones were more common in premolars than canines and anterior teeth (p < 0.05) (Table 2).
Table 2
Prevalence of pulp stones regarding arch, side and tooth type (n = 379)
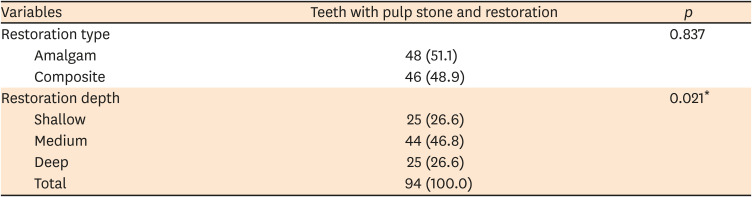
Nearly one-quarter of teeth (24.8%) with pulp stones had restorations. The percentages of pulp stones in composite and amalgam restored teeth were nearly equal (p > 0.05). The prevalence of pulp stones in teeth with medium-depth restorations was significantly higher (46.8%) than that in teeth with shallow (26.6%) and deep restorations (26.6%) (p1-2= 0.022) (Table 3).
Table 3
Distribution of teeth with pulp stones and restorations regarding restoration type and depth (n = 94)
DISCUSSION
Pulp stones may lead to adverse outcomes in endodontic therapy, as they can block the root canal paths. In addition to blocking the passage of files through root canals, they can cause deformation of file tips [19]. Furthermore, pulp stones may hamper disinfection/irrigation procedures [20]. Consequently, pulp stones can give rise to clinical difficulties in endodontic therapy [2].
Many previous studies have used panoramic radiography and histological analysis for the detection of pulp stones [12122]. As noted earlier, calcified masses with diameters smaller than 200 µm may not be detected on panoramic radiographs. Thus, the percentage of pulp stones detected using histological analysis is higher than that using panoramic radiography, which is helpful only as an ex-vivo technique [22]. In addition, pulp stones may not be detected on periapical radiographs because of the superimposition of alveolar bone. CBCT overcomes the problem of overlapping structures and permits high-resolution images in axial, coronal and sagittal planes. As such, it is the most useful and accurate imaging technique available to detect the presence of pulp stones [15]. Thus, the present study used CBCT images to detect the presence of pulp stones and analyze the possible association between pulp stones and the following parameters: age, sex, dental arch and side, tooth type, and restoration type and depth. None of the patients in this study were exposed to additional radiation, as the data were obtained from archival CBCT image records.
We detected pulp stones in 3.3% (379/11,494) of all teeth assessed and 24.2% (163/673) of all patients assessed. In other CBCT studies, Tassoker et al. [23] and Patil et al. [24] detected pulp stones in 52% and 50.93% of patients, respectively, and da Silva et al. [9] reported pulp stones in 31.9% of patients. The present study examined pulp stones only in the coronal pulp chamber, as pulp stones tend to be more common in this region. Radiopaque masses in the radicular part were considered diffuse calcifications [25]. This may explain the difference in the percentage of pulp stones detected in the present study as compared with the findings of previous research.
Sener et al. [10] reported pulp stone prevalence as 38% in 536 patients and 4.8% in teeth by evaluating periapical and bite-wing radiographs on a Turkish subpopulation. On the other hand, Gulsahi et al. [26] reported a pulp stone prevalence in periapical radiographs of 12% in 519 patients and 5% in teeth. In this study, we detected a pulp stone prevalence of 24.2% in 673 patients and a prevalence of 3.3% in teeth. The discord in the findings can be explained by geographical differences and imaging techniques.
Tamse et al. [27] noted that the percentage of pulp stones increased with age. However, Hsieh et al. [11] reported that there was no association between pulp stones and age. In the present study, the percentage of pulp stones in the 30–39 years (31.1%) age group was significantly higher than that in the 18–19 years (18.5%) and ≥ 60 years (17.3%) age groups The conflicting results of these studies may be explained by the fact that restorative treatments, which cause chronic inflammation in pulp tissue, are performed more frequently among the middle-aged population in Turkey. In addition, older age is commonly associated with obstructions in root canals rather than pulp stones [28].
Consistent with the findings of many studies, the prevalence of pulp stones in this study was higher in females than males (28.9% vs. 18.7%), which might be related to the increased frequency of bruxism in females [1014]. In contrast, Hsieh et al. [11] and al-Hadi Hamasha et al. [29] found that the prevalence of pulp stones was higher in males than females. The discord in the findings may be explained by the hypothesis that calcifications, which are associated with pulpal inflammation resulting from chronic irritants, are detected mostly in men from the countries where those studies were performed [30]. Some previous studies found no statistically significant association between pulp stones and sex [913].
In this study, the percentage of pulp stones in the maxilla was significantly higher than that in the mandible. Similarly, Hsieh et al. [11] reported higher numbers of pulp stones in maxilla than mandible. Some studies found that the percentage of pulp stones in maxillae and mandibles was nearly equal, [2324] whereas another research detected a higher percentage of pulp stones in mandible than maxilla [31]. Thus, further examinations with larger sample sizes are needed. Similar to our results, many studies detected a higher prevalence of pulp stones in molars [111829]. The volume of molar teeth may explain this finding. Due to the large amount of pulp tissue and high blood supply that molars have, their pulp tissues calcify easier than that of other tooth groups. The early eruption time of molars as compared to premolars may be another explanation for the increased prevalence of pulp stones, with molars exposed to irritation for a longer period [27].
In the present study, 24.8% of teeth with pulp stones had restorations. In other studies, da Silva et al. [9] and Tassoker et al. [23] reported that 13% and 73.5% of teeth with pulp stones had restorations, respectively. Differences in the study populations and oral care habits may explain the discord in the findings. In the present study, the percentages of pulp stones associated with composite and amalgam restorations were nearly the same. Besides, the severity and duration of chronic irritation caused by these restorations might be critical and affect the findings of the studies. Longitudinal researches are needed to resolve this problem [10] da Silva et al. [9] and Tassoker et al. [23] reported that as the depth of a restoration increased, the possibility of pulp stones increased. One possible explanation for this finding may be the theory that chronic irritation of pulp tissue leads itself to produce pulp stones as a defense mechanism. However, it was reported that pulp stones were more commonly found in teeth with medium-depth restorations in this study. The retrospective nature of this study may explain this finding. Based on this study’s findings, the null hypothesis was rejected.
The absence of data on the age of the restorations and comparatively limited sample size can be considered as limitations of the present study. Due to the uncertainty about the restoration duration and intensity of chronic irritation in teeth with restorations, we did not assess in terms of restoration presence or absence. This may also be considered a limitation of the study. In this study, the medical conditions of the patients were ignored. Considering that some systemic diseases may cause pulp stone formation, this may be noted as another limitation of this study.
CONCLUSIONS
Within the limitations of this study, a pulp stone prevalence was detected of 24.2% in 673 patients and a prevalence of 3.3% in teeth. The presence of medium-depth restorations increased the risk of pulp stone formation. It can also be concluded that female sex and maxillary molar teeth were associated with a higher percentage of pulp stones. The percentage of pulp stones in the 30–39 years age group was the highest among the other age groups. Dentists should be aware that pulp stones can be encountered frequently in the clinical scenario and various predisposing factors can trigger pulp stone formation.
 XML Download
XML Download