

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Accurate knowledge of the root canal anatomy, comprehensive assessment of radiograph images, proper access to the canal orifices, thorough chemo-mechanical instrumentation, and 3-dimensional (3D) obturation is essential for a successful root canal therapy [1]. The genetic and ethnic variations in the root canal anatomy are fairly common, and they have been extensively discussed [2]. Thus, the internal root canal anatomy must be determined as it is used as a basis for the course of endodontic therapy [3].
Conventional radiography is an indispensable tool for rapid chair-side visualization of the root canal anatomy, but 3D visualization is not achieved. Thus, methods that can enhance visualization are required. Barker et al. [4] first attempted to use an endogram to enhance the radiographic visualization of the root canals using contrast media but, the toxic lead-based elastomeric contrast media was difficult to remove from the root canals. Water-soluble contrast agents have been used with varying degrees of success [56]. Contrast media can be categorized into the ionic type (monomers: diatrizoic acid, iodic acid, and ioglicic acid and dimers: ioxaglic acid and iocarmic acid) and the non-ionic type (monomers: iohexol, iopamidol, iobitridol, ioversol, iopromide, and iopentol and dimers: iotrol, iotrolan, and iodixanol). The non-ionic type has lower osmolality and reduced chemotoxic effects and is better tolerated and less viscous than the ionic type [7].
The Ruddle's solution is an iodinated ionic contrast media containing 5% sodium hypochlorite (NaOCl), 17% ethylenediaminetetraacetic acid (EDTA), and Hypaque (GE Healthcare, Chicago, IL, USA). NaOCl dissolves organic tissues and, enhances the ingress of the radiopaque dye molecules into the root canal system. However, it should not be introduced forcefully [8].
Chitosan is a natural polysaccharide prepared via the deacetylation of chitin and obtained from the shells of the crustaceans. It is an effective chelating agent similar to EDTA and has an antimicrobial property that prevents the growth of microorganisms in the root canal system [91011]. Injectable radiopaque chitosan-based hydrogels have been used in endovascular therapies as sclerosing embolizing agents for the treatment of endoleaks and endovascular aneurysm repair [1213]. Our research team formulated a chitosan-based endo-radiopaque solution (CERS), which was granted Indian patent [14]. Thus, the current study aimed to perform an in vitro comparison of 4 different contrast media introduced into the maxillary premolars and molars and in vivo comparison between Xenetix 350 + 5.25% NaOCl and CERS was conducted to visualize the root canal anatomy of the maxillary and mandibular premolars and molars.
Go to : 
MATERIALS AND METHODS
Chemicals
The following chemicals were used in the experiment: Omnipaque 350 (non-ionic; GE Healthcare, Bengaluru, India), Iopamidol (non-ionic; Bracco Diagnostic Inc., Milan, Italy), Xenetix 350 (non-ionic; Guerbet, Hong Kong), Urografin 76 (ionic; Bayer, Madrid, Spain), chitosan (I-chess, Mumbai, India), and CERS, which is a mixture of 3% chitosan, iobitridol, and 100% acetone alcohol [14].
Sample size calculation
The study was approved by the ethics committee of Siksha ‘O’ Anusandhan (Deemed to be University), Odisha, India (reference No. DMR/IMS-SH/SOA/16029). In vitro study was conducted over a period of 4 months (July 2016–October 2016) and the in vivo study was carried out during the period Jan 2017–March 2019 according to the STROBE statement (http://www.strobe-statement.org). The sample size was determined based on the results from previous studies using G* power software, version 3.1.9 (available at http://www.gpower.hhu.de/en.html) [715]. With the level of significance and the power of test set at 5% and 80% respectively, the individual group sample size for in vitro was n = 60 (total 120 teeth) and for in vivo was n = 40 (total 80 teeth).
In vitro experiment
1. Sample collection and preparation
Extracted human maxillary premolars (group 1, n = 60) and molars (group 2, n = 60) with intact roots and mature apices were collected from the department of oral surgery according to the university guidelines. After extraction, the teeth were immersed in 5.25% NaOCl solution (Prime Dental Products Pvt Ltd., Thane, India) for 30 minutes to remove soft tissue remnants and stored in 0.2%thymol solution until use.
The teeth in each group were divided (software: www.randomizer.org) into 4 subgroups (n = 15 each) according to the contrast media used (a) Omnipaque 350, (b) Xenetix 350, (c) Iopamidol, and (d) Urografin 76.
Subsequently, the teeth were mounted on polyvinyl siloxane putty (President, Coltene/Whaledent AG, Altstätten, Switzerland), and radiography in bucco-lingual and mesio-distal plane was performed using the digital radiovisiography (RVG) (CDR, FONA, Assago, Italy) and x-ray unit (X-Mind DC, Acteon, Italy) operating at 7 mA and 70 kv for 0.1 second.
2. Application and evaluation of contrast media
A single trained endodontist performed the procedure to avoid procedural bias. All procedures were performed under a dental operating microscope (DOM) (Alpha Slim 6, Seiler Instrument, St. Louis, MO, USA) at 6–10× magnification. In total, 1 mL of each contrast solution was mixed with 0.5 mL of 5.25% NaOCl via electro-stirring. After access cavity preparation, the contrast media was passively introduced into the pulp chamber using a double side-vented 30-G endodontic irrigation needle (Mirajet Endotec duo Luer, Hager & Werken, Duisburg, Germany). After 1 minute, RVGs in bucco-lingual and mesio-distal planes were performed to analyze the depth of contrast media ingress. The canal patency was determined using a no.6 K-file (MANI, Utsunomiya, Japan), and coronal third enlargement was performed with the Sx file (Protaper Universal, Dentsply Maillefer, Ballaigues, Switzerland) with X-smart Plus endomotor (Dentsply Sirona, York, PA, USA) at a torque of 4.0 N.cm and 350 rpm. Under DOM (6× magnification) actual length (AL) was determined by inserting a size 10K file into the canal until visible at the apical foramen. Working length (WL) was established by subtracting 0.5 mm from the AL. Canal enlargement was done with the sequential use of K-file (MANI) sizes #8, #10, #15, and #20 up to WL. Two mL of 3% NaOCl was used between each successive file size. The canals were dried using absorbent paper points (DiaDent, Cheongju, Korea), and 0.5 mL of contrast media was introduced into each canal using a positive pressure with a double side-vented 30-gauge endodontic irrigation needle and successive RVG was performed.
To evaluate the depth of contrast media ingress and to identify the aberrant root canal anatomy, 2 experienced endodontists who were blinded to the study assessed the results (Figure 1), using the scoring criteria described in a study [15].
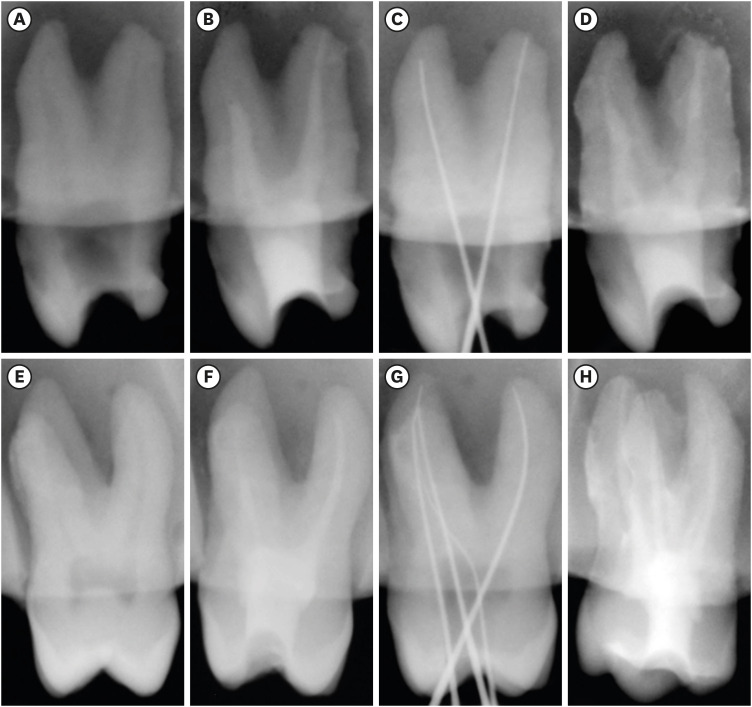 | Figure 1In vitro radiographs illustrating Ingress of Xenetix 350 + 5.25% sodium hypochlorite into root canals. (A, E) Pre-operative radiographs (mesio-distal) of maxillary premolar and molar teeth. (B, F) Compromised ingress of contrast solution into the root canals after access opening. (C, G) Working length radiographs of premolar and molar teeth. (D, H) Complete ingress of contrast solution into the root canals after cleaning and shaping.
|
The scoring criteria for contrast media ingress in the root canals were as follows:
0: No radiopacity
1: Radiopacity up to the middle third.
2: Radiopacity up to the apical third.
3: Radiopacity of the apical part of the root canal along with the accessory canals.
The scale was further dichotomized, with scores of 0 and 1 (inadequate ingress) and scores of 2 and 3 (adequate ingress) of the contrast media.
In vivo experiment
1. Patient selection and randomization
In total, 80 patients (open-labeled, multi-arm parallel group) who visited the department were included in the study. The inclusion criteria were healthy adults aged 20–40 years with a chief complaint of symptomatic irreversible pulpitis (only vital teeth) with no history of any systemic diseases and allergies. Following radiographic evaluation, teeth with open apices, receded pulp chambers, and resorbed apex were excluded from the study. The age group selection was based on complete pulp space development by 20 years, and higher chances of completely receded pulp chambers beyond the age of 40 years.
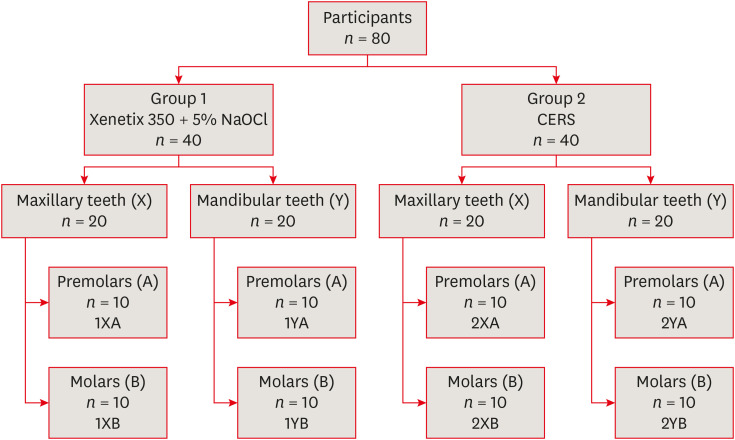
Informed consent was obtained from the participants. A patch test was performed by injecting 0.2 mL of the contrast media subcutaneously, and the area was monitored for about 5 minutes for the presence of any inflammatory reaction/sensitivity. The patients were randomly assigned to 2 groups (group 1: Xenetix 350 + 5.25% NaOCl, group 2: CERS, n = 40 each) using the software available at www.randomizer.org. The allocation of participants to subgroups is presented in Figure 2. Preoperative RVG was performed using the x-ray unit operating at 7 mA and 70 kv for 0.1 second. All RVGs were taken in between 0°–30° angulations and images were stored using FONA's imaging software. After obtaining adequate pulpal anesthesia (LOX 2%, Neon Laboratories, Mumbai, India), the teeth were isolated under a rubber dam (Hygenic, Coltene/Whaledent AG). Standardized access cavities were prepared using a high-speed handpiece under a water coolant with an endo-access bur (sizes #2 and #3, Dentsply Maillefer).
Mandibular teeth (YA, YB)
One mL solution was introduced into the canal orifices with a double side-vented 30-gauge endodontic irrigation needle. A dampened cotton pellet was placed in the cavity and RVG was taken to evaluate the extension of the solution in the canals. Subsequently, in all groups, WL was determined by using an apex locator (CanalPro, Coltene Whaledent), and initial cleaning and shaping was done with the sequential use of K-file (MANI) sizes #8, #10, #15, and #20 up to WL. Sx file was used to enlarge the coronal third of the canal and S1 file (ProTaper Universal) was used till WL. Insertion of the contrast media is performed as discussed in section 2.
Maxillary teeth (XA, XB)
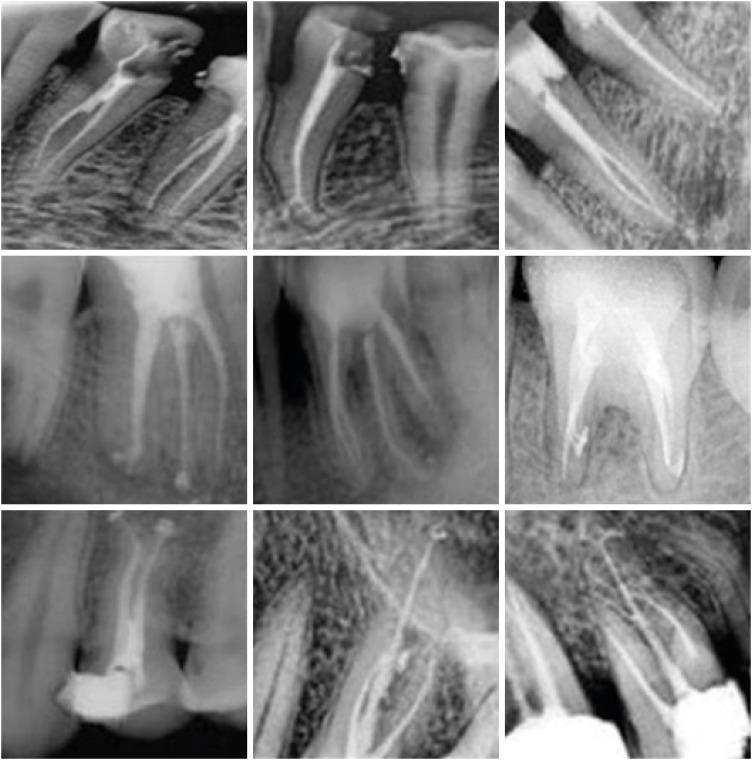
A similar procedure (as in the mandibular group) was followed for the maxillary teeth group. Achieving the contact time of the solution in the root canals was challenging due to gravitational force. This was managed by using contrast media-dampened absorbent points. To prevent the solution from flushing out of the pulp chamber/canal, a double side-vented 30-G needle with the solution was introduced and exposure to RVG was done with the needle in the canal (Figure 3J).
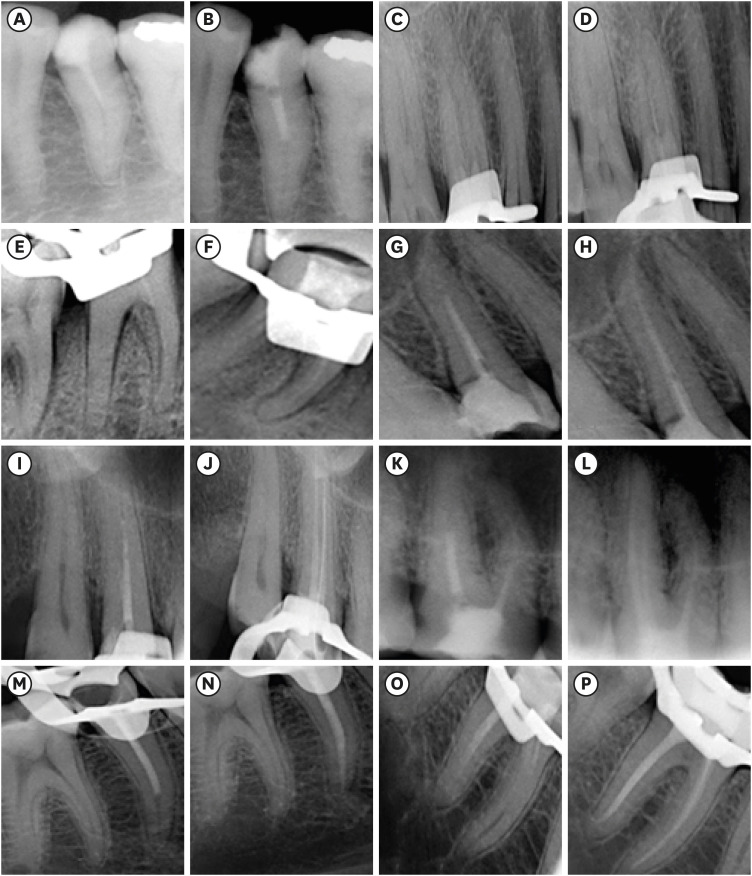
Two experienced endodontists, blinded to the study, assessed and scored both the groups based on the depth of ingress and efficacy in identifying lateral or accessory canals in both groups (Figure 3). The solutions were flushed out from the root canals by irrigating with a copious amount of saline and confirmed with the radiographs. All root canals were obturated using the warm vertical condensation technique with a sealer (Sealapex, Kerr, Brea, CA, USA). Patients' postoperative pain was evaluated (24 hours and 72 hours interval) and anti-inflammatory medications were prescribed if required.
Statistical analysis
Statistical analysis was conducted using IBM SPSS statistics 24.0, SPSS South Asia Pvt. Ltd. (http://www.spss.co.in). The degree of interobserver reliability was assessed using a Kappa analysis of agreement of 0.7–0.8, and Cronbach's alpha reliability between observers was 0.62. Hence, the readings of the first observer were considered. The Kruskal–Wallis test was applied for the in vitro study in maxillary premolars and molars to compare the depth of ingress of the 4 contrast media.
Wilcoxon-signed rank test was used for comparison of depth of ingress of Xenetix 350 + 5.25% NaOCl and CERS among the roots of maxillary and mandibular premolars and molars (before and after initial cleaning and shaping). Mann-Whitney U test was used to compare the level of significance between the groups. The level of significance was set at p = 0.05.
Go to :
RESULTS
Based on the interobserver analysis of agreement in the in vitro study, Xenetix 350 + 5.25% NaOCl (groups 1 and 2, p < 0.05) had the most significant depth of ingress, followed by Urografin 76, Iopamidol, and Omnipaque 350 (Tables 1 and 2). In Figure 1, the ingress of Xenetix 350 + 5.25% NaOCl after access opening is significantly more in premolars (B) as compared to the molar (F). For both premolars and molars after initial cleaning and shaping, the ingress of contrast media to the WL increased (Figure 1D and 1H) and, significant canal anatomy was visualized on the radiograph.

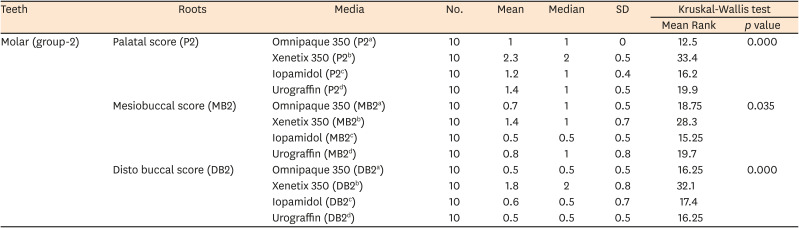
Table 1
Comparative scores of contrast medias in premolar teeth (in vitro)
![]()
Table 2
Comparative scores of contrast media in molar teeth (in vitro)
![]()
In vivo study, CERS group had a significantly higher depth of ingress as compared to Xenetix 350 + 5.25% NaOCl. Ingress of CERS in maxillary premolars (XA) and mandibular molars (YB) (p < 0.01) were statistically significant in comparison to maxillary molar (XB) and mandibular premolar (YA) (p < 0.05; Table 3). In both groups, the scores/depth of ingress after cleaning and shaping was significantly higher. After cleaning and shaping the efficacy of identifying the aberrant root canal anatomy was increased. Accessory canals/apical delta was observed in 2 palatal roots of maxillary premolars, 3 mandibular premolars (2YA), 2 palatal roots of maxillary molars (2XPB), 3 (2-distal, 1-mesial) of mandibular molars (2YB). All those who entered the study were accounted for.
Table 3
Comparison of scores by media solutions type among premolar and molar teeth (in vivo)
NaOCl, sodium hypochlorite; CERS, chitosan-based endo-radiopaque solution; XA, maxillary premolar; YB, mandibular molar; XB, maxillary molar; YA, mandibular premolar.
*Significant level at 5%; †Significant level at 1%.
![]()
Go to :
DISCUSSION
The use of contrast media and endo-radiopaque solution during intraoperative digital radiography has been considered effective in determining the root canal anatomy [16]. In vitro, the absence of pulpal tissues in the pulp chamber and the root canal resulted in a greater ingress of contrast media solution. Compared with ionic media, non-ionic contrast media can be easily delivered due to low osmolality and less viscosity. In terms of disadvantages, ionic contrast media causes discomfort and, individuals can feel the heat sensation during injection due to high osmolality, cytotoxicity of the agent and, increased pressure requirement during injection [7].
The current in vitro study indicated that Xenetix 350 + 5.25% NaOCl (p < 0.05) had the greatest efficacy, followed by Urografin 76, Omnipaque 350, Iopamidol. The root canals of the maxillary premolars (mean rank: P1 canal-34.6, B1canal-21.67) had a significantly higher ingress of contrast media penetration than those of the maxillary molars (mean rank: P2canal-33.4, MB2canal-28.3, and DB2canal-32.1). Based on various clinical trials Xenetix 350 is a safe and effective iodine-based contrast media with low osmolarity and, 5.25% NaOCl helps in eliminating the organic and inorganic debris from the root canal [17181920]. Thus, the in vitro study helped in formulating the CERS composition, and Xenetix 350 + 5.25% NaOCl was selected for further in vivo comparison.
In clinical settings, calcifications in the pulp chamber and root canals, constriction of root canals and, increased volume of pulpal tissues in the chamber must be considered, which might prevent ingress of the solution. In the present study, patients within the age group of 20–40 years were considered as they have patent canals and fewer difficulties in glide path, whereas beyond 40 years of age the canals have a smaller diameter, few auxiliary canals, higher incidence of dentinal tubules obliteration and, deposition of inorganic content [212223]. In the current study, for better ingress of the solution Gates-Glidden drills (MANI) and Start X ultrasonic endodontic tips (Dentsply Maillefer) were used to remove pulpal tissues and calcifications respectively [24]. Enhanced visualization of the solution was observed in the mandibular teeth as compared to the maxillary teeth. The compromised visualization of the root canals in the maxillary molar teeth was attributed to the orientation of the roots, overlapping roots, superimposition of the maxillary sinus/zygoma, and holding time of the solution in the pulpal chamber against gravitational forces.
The root canal anatomy can be accurately assessed using a radiographic angulation of 0°–30° [16]. Based on this criterion all RVG's in the present study were taken within this range for assessing root canal anatomy. The sensitivity of the intra-rater reliability improved with the use of the zoom, inverse, and revealer options in the RVG software. Hence, the Kappa analysis of agreement indicated a high standard of agreement (> 0.61).
The in vivo study revealed that CERS (group 2) had a greater depth of ingress in the maxillary premolars (−3.888), mandibular premolars (−2.339), maxillary molars (−2.363), and mandibular molars (−3.465) as compared to Xenetix 350 + 5.25% NaOCl (group 1). The clinical performance of Group 1 was compromised (Figure 3A-3F) as the solution cannot be injected forcefully due to the risk of NaOCl accident.
The enhanced visualization of the root canal anatomy with the use of CERS (Figure 3G-3P) is attributed to the combinatorial effect of 3% liquid chitosan, iobitridol, and 100% acetone. Chitosan is a natural polysaccharide with a molecular weight of 100–3,000 kg/mol, and has a good antimicrobial and chelating effect on the root canal walls [25]. Acetone reduces the viscosity of the contrast media without any physical changes in the solution. Ingress of the solution was compromised in both groups when it was immediately placed after access cavity preparation. However, the visualization of CERS was better after initial cleaning and shaping and adequate irrigation of the root canals [20]. Optimal visualization of the accessory/lateral canals was seen in the apical one-third of the roots (Figure 4). CERS was completely removed from the canal as the complete irrigation protocol was followed and was confirmed by subsequent radiographs. According to previous studies, complete removal of Hypaque solution was checked radiographically after each successive step of the shaping procedures and, the contrast media was flushed with 0.5mL of 3% NaOCl by manual agitation and ultrasonic activation [2627]. Radiopaque solutions have been used as root canal irrigant before obturation for assessing the root anatomy, and are beneficial for investigating the penetration of the root canal irrigation solution [28]. Hence, to achieve a successful endodontic therapy, CERS can be used routinely to identify the complex root canal anatomy during and after cleaning and shaping.
In the current study, no adverse reaction was observed immediately after the completion of the root canal therapy. A 24-hour evaluation showed that 92% (n = 74) of the patients were comfortable and no postoperative pain and other reactions were observed. Two patients in group 1 and 4 patients in group 2 required anti-inflammatory medications due to pain within the first 24 hours, and a significant reduction in pain was noted thereafter. For both groups, no apical extrusions of solutions occurred and were flushed out suggesting that root canal instrumentation and obturation techniques may influence post-operative pain [29]. Previous literature states that the most adverse reaction of the contrast media was warmth sensation which occurs initially, and is transient [17]. Limitations of the study include restricted initial ingress of contrast solutions before cleaning and shaping in all groups and maxillary molar teeth (particularly MB and DB canals) due to canal curvature and gravitational forces. The factors impeding the detection of accessory canals include a narrow lumen, resolution of RVG, and masking of accessory canals (buccal and lingual direction) due to 2D RVG images.
Go to :
CONCLUSIONS
In the current study, the use of CERS to visualize and understand the intricate canal anatomy for endodontic treatment via RVG was found to be effective. Future research using CERS can be conducted regarding the cleaning efficacy of the organic and inorganic debris from the root canal and to determine the clinical incidence of accessory and/or lateral canals routinely.
Go to :
 XML Download
XML Download