

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The success of endodontic treatment is strongly affected by the quality of root canal treatment and coronal restoration [123]. In endodontically treated teeth (ETT), coronal restorations provide a coronal seal and protect the remaining tooth structure from fracture [45]. Fracture of ETT usually occurs when ETT are not immediately restored, resulting in coronal microbial leakage or an unrestorable fracture [678].
The amount of remaining tooth structure affects the fracture resistance of ETT [49101112]. Tooth structure loss, quantified in terms of the number of sides, has been reported to be a significant factor associated with reduced tooth stiffness and an increased risk of fracture in posterior ETT [131415]. Loss of marginal ridge(s) decreases tooth stiffness, increases cuspal flexure and, consequently, leads to a risk of tooth fracture [111216].
Previous retrospective studies have indicated that placement of a full-coverage restoration significantly improved the overall survival rate of posterior ETT after fractures [81314]. Nevertheless, a recent systematic review reported that the long-term success of resin composite restorations in posterior ETT depended on the amount of tooth structure loss [5]. A recent clinical study demonstrated a high survival rate of posterior ETT with composite fillings that had different amounts of tooth surface loss, but the results did not report the survival separately by tooth type [14]. Retrospective studies have presented higher survival rates from fracture for premolar ETT with mild to moderate tooth structure loss that were restored with resin composite restorations than for those restored with full-coverage crowns [131718]. However, the results of these studies are limited to only premolar ETT.
A previous study showed an acceptable survival rate of molar ETT with an adequate amount of remaining tooth structure that were restored with resin composite in a short-term period. However, that study did not compare the survival with ETT restored using crown restorations [19]. To date, limited research has compared the fracture survival rate between direct resin composite and crown restorations in molar ETT. Therefore, the purpose of this study was to compare the fracture survival rates of molar ETT restored with direct resin composites or crowns, using a retrospective cohort design. In addition, the potential risk factors associated with fracture survival were identified.
MATERIALS AND METHODS
The protocol of this retrospective study was approved by the Institutional Ethics Committee of Mahidol University (MU-DT/PY-IRB 2020/019.3003) and Rangsit University (DPE. No. RSUERB2020-020). The dental records of patients who received nonsurgical endodontic and restorative treatments and presented at a recall visit from 2015 to 2019 were collected. Some of the ETT molars were selected from our previous study, with a longer follow-up period, and some new ETT were included [13]. The data of the ETT were reviewed and included in the study if the teeth satisfied the following criteria.
The inclusion criteria for ETT were 1) first and second molars with mature root formation; 2) teeth restored with single-unit full-coverage crowns or direct resin composite restorations; 3) a recall examination period of at least 12 months; and 4) adequate data regarding treatment procedures, clinical records, and radiographic records. The exclusion criteria were 1) teeth extracted for other reasons, not due to unrestorable fracture; 2) chronic periodontitis with bone loss of more than half of the root length; 3) preoperative cracks or radicular fracture; 4) history of surgical root canal treatment, hemisection, or root amputation; and 5) fixed orthodontic appliances.
Endodontic and restorative procedures
Root canal treatments were performed by undergraduates, postgraduates, or endodontists under rubber dam isolation. Root canal cleaning and shaping were performed with the crown-down technique using 0.02 taper hand stainless steel and/or 0.04/0.06 taper rotary Ni-Ti files with 2.5% sodium hypochlorite and 17% EDTA irrigants. After calcium hydroxide intracanal medication, the prepared root canals were then obturated with gutta-percha cones and root canal sealer (zinc oxide, epoxy resin, or calcium silicate-based sealer), using one of the following root canal obturation methods: lateral compaction, vertical compaction, or the cold hydraulic (sealer-based) technique.
Coronal restorations were performed by undergraduates, postgraduates, or prosthodontists. Full-coverage crown restorations (with core build-up or post placement) were commonly planned as a final restoration. Direct resin composite restorations were placed as a long-term, interim restoration in cases with a questionable prognosis in terms of endodontics or periodontics, or those on a waiting list for crown restorations. Resin composite was occasionally used as a permanent restoration for patients who could not afford the cost of a crown, or for ETT with tooth structure loss limited to the occlusal surface only.
In cases that were restored with crown restorations, a post was only indicated when the retention from the remaining tooth structure for core build-up was not adequate. Cast metal posts or prefabricated fiber posts (D.T. LIGHT-POSTS (BISCO Inc., Schaumburg, IL, USA) or FRC Postec Plus (Ivoclar Vivadent AG, Schaan, Liechtenstein) were cemented into the prepared root canals with adhesive resin-based cement (Panavia F 2.0, Kuraray Noritake Dental Inc., Tokyo, Japan) or core build-up material (MultiCore Flow, Ivoclar Vivadent AG).
In ETT restored with resin composite restorations, resin composite was placed without the use of a post. The access cavity was prepared using Cavit (CAVITON, GC Corp., Tokyo, Japan), or glass-ionomer cement liner (Vitrebond, 3M ESPE, St. Paul, MN, USA; or GC Fuji VII, GC Corp.) applied at a thickness of 1-2 mm. Resin composite (Z250 or Z350, 3M ESPE) was placed and bonded with etch-and-rinse adhesive (Adper Single Bond 2, 3M ESPE), or self-etch adhesive (Clearfil SE Bond, Kuraray Noritake Dental Inc.).
Data collection and assessment criteria
An overview of the methodology is presented in Figure 1. From clinical and radiographic records, the following information was collected: age, sex, recall period (months), tooth type, tooth location (upper or lower), coronal restoration (crown or resin composite), opposing dentition (natural tooth, fixed prosthesis, removable prosthesis, or none), and number of adjacent teeth. For ETT restored with resin composite restorations, the amount of tooth surface loss was identified from dental records. For ETT restored with full-coverage crowns, the type of post was recorded as no post, a fiber post, or a metal post.
Figure 1
An overview of the methodology in this retrospective study of fracture survival in molar endoscopically treated teeth (ETT) restored with crowns or resin composite restorations.
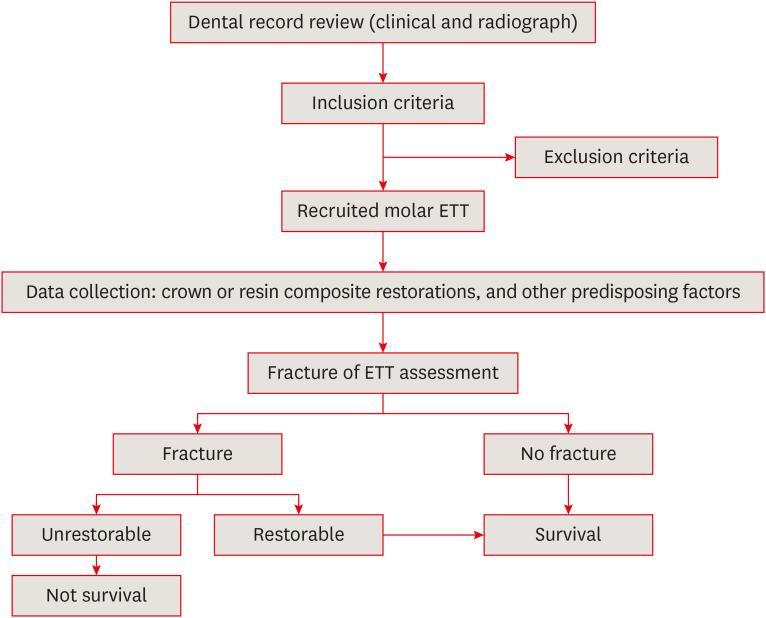
The incidence of fractures and their restorability were identified, and fractures were classified as restorable or unrestorable. Survival was defined using the following criteria: 1) survival: no fracture or a restorable fracture; 2) non-survival: an unrestorable fracture.
Statistical analysis
The survival rates from fracture of ETT restored with full-coverage crown and resin composite were analyzed using the Kaplan-Meier method. The survival rate of the 2 different coronal restorations overall and according to 2 different observation periods—short-term (12−24 months) and long-term (24–60 months)—was statistically compared using the log-rank test. A multivariate Cox proportional hazards model was used to identify any potential risk factors. Factors with a p value ≤ 0.25 and predisposing factors of interest were further analyzed in the multivariate analysis [71314]. A p value < 0.05 was considered to indicate statistical significance. ETT restored with resin composites according to different amounts of tooth structure loss were sub-analyzed using Kaplan-Meier survival analysis.
RESULTS
Data distribution and survival analysis
In total, 169 molar ETT were included in this study. The distribution of predisposing factors of interest and fracture survival rates are presented in Table 1. The ETT were obtained from patients who were 18 to 78 (44.55 ± 15.48) years of age (40 men and 129 women). The ETT comprised 51 maxillary teeth and 118 mandibular teeth, and the coronal restorations were resin composites in 87 cases and crowns in 82 cases. The follow-up period ranged from 12 to 60 months, with a mean of 31.73 (± 17.56) months.
Table 1
Predisposing factors and survival analysis of unrestorable fractures in molar endodontically treated teeth (ETT; n = 169)
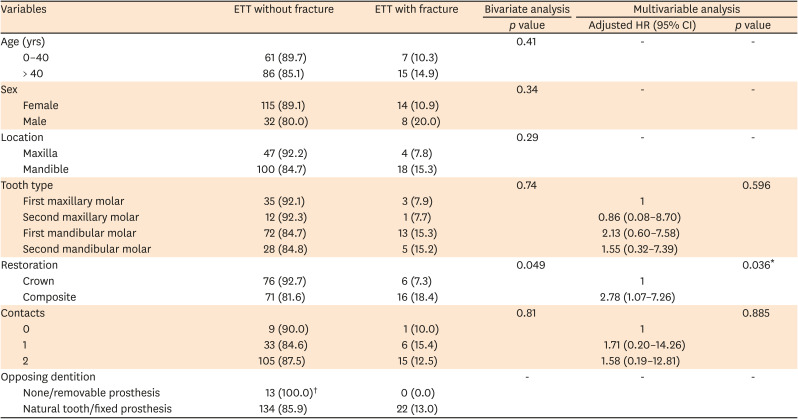
Values are presented as number (%).
HR, hazard ratio; CI, confidence interval.
*The log-rank test (α = 0.05) was used to compare the fracture survival rates within each factor. The factors with a p value ≤ 0.25 and predisposing factors of interest from previous studies were further analyzed using the Cox regression model [71314]; †The p value was not calculated because no cases of ETT fracture were identified.
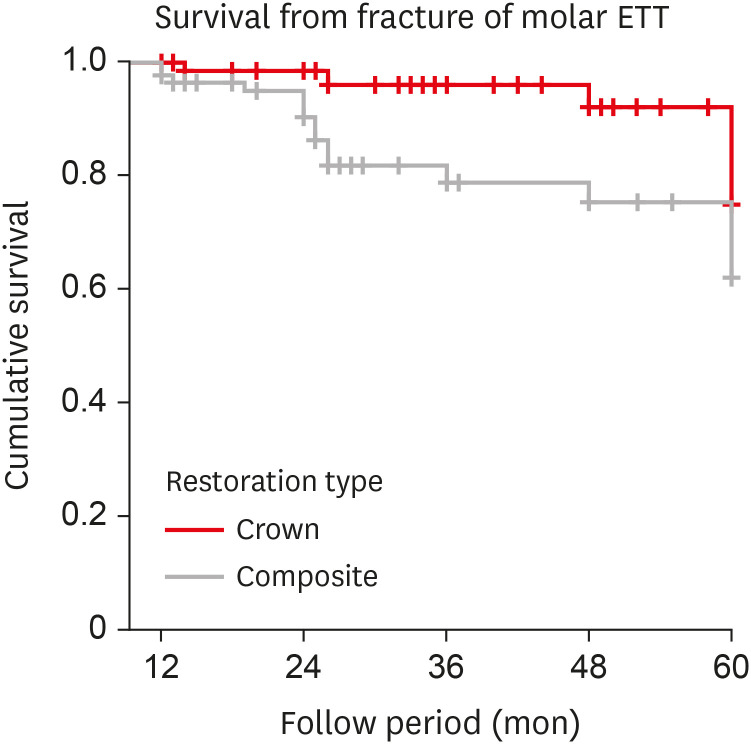
The overall fracture survival rate of molar ETT was 87%. Based on the coronal restorations, the survival rates from fracture of molar ETT restored with resin composites and crowns were 81.6% and 92.7%. The Kaplan-Meier survival analysis according to the type of coronal restoration is presented in Figure 2. From the log-rank test and multivariate Cox proportional hazards model, the type of coronal restoration was found to be a significant predisposing factor that affected the overall fracture survival rate of molar ETT (p < 0.05). No significant difference in the survival rates was observed according to other factors (i.e., age, sex, location of tooth, tooth type, number of contacts, and opposing dentition). In terms of the Cox proportional hazard ratio (HR), the ETT restored with resin composite restorations were 2.78 times more likely to have an unrestorable fracture than ETT restored with crowns (HR, 2.78; 95% confidence interval, 1.07–7.26; p < 0.05).
Figure 2
Kaplan-Meier survival analysis of molar endoscopically treated teeth (ETT) according to the 2 different coronal restoration types. The 5-year overall survival rates of molar ETT restored with full-coverage crowns and resin composites were 92.7% and 81.6%, respectively, and a significant difference was demonstrated (p < 0.05). The survival rates of molar ETT with resin composites and crowns were significantly different (97.6% vs. 83.7%) in the short-term period (12–24 months). The long-term survival rates (24–60 months) were not significantly different between the 2 restoration types (87.8% vs. 79.5%).
Fracture survival rate of endodontically treated teeth restored with full-coverage crowns and resin composites according to short- and long-term observation periods
The fracture survival rates at 12 to 24 months (short-term) and more than 24 months (long-term) for full-coverage crowns were 97.6% and 87.8%, and those for resin composite restorations were 83.7% and 79.5%, respectively (Table 2). A significant difference in the survival rates of the 2 different restorations was observed in the short-term period (p < 0.05). No significant difference in the survival rate was observed between the 2 restoration groups in the long-term period.
Table 2
Fracture survival rate of molar endodontically treated teeth (ETT) restored with crowns and resin composites according to the observation period after restoration

Fracture survival rate of endodontically treated teeth restored with resin composite restorations
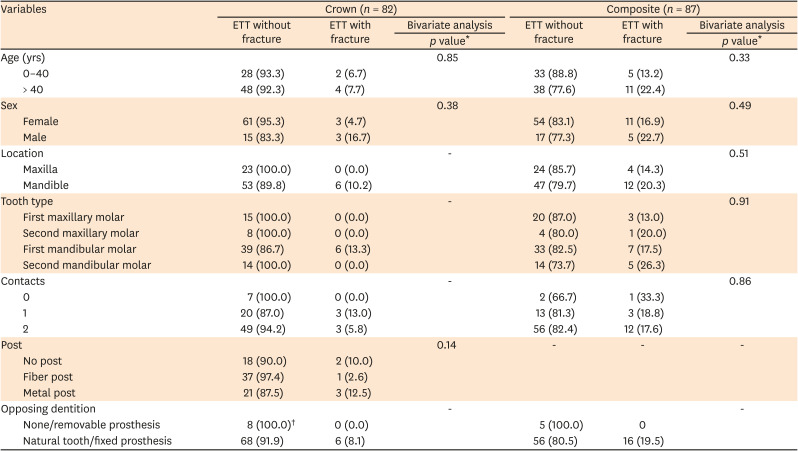
None of the predisposing factors were identified as significant factors that affected the survival rate of molar ETT restored with resin composites (Table 3). The survival rates from fracture of maxillary teeth and mandibular teeth were 85.7% and 79.7%. The first maxillary molars had the highest survival rate (87%) and the second mandibular molars had the lowest survival rate (73.7%). ETT with 2 adjacent teeth had a higher survival rate than those with 1 or 0 adjacent tooth.
Table 3
Distribution of predisposing factors and survival analysis of unrestorable fracture in molar endodontically treated teeth (ETT) restored with 2 different restoration types
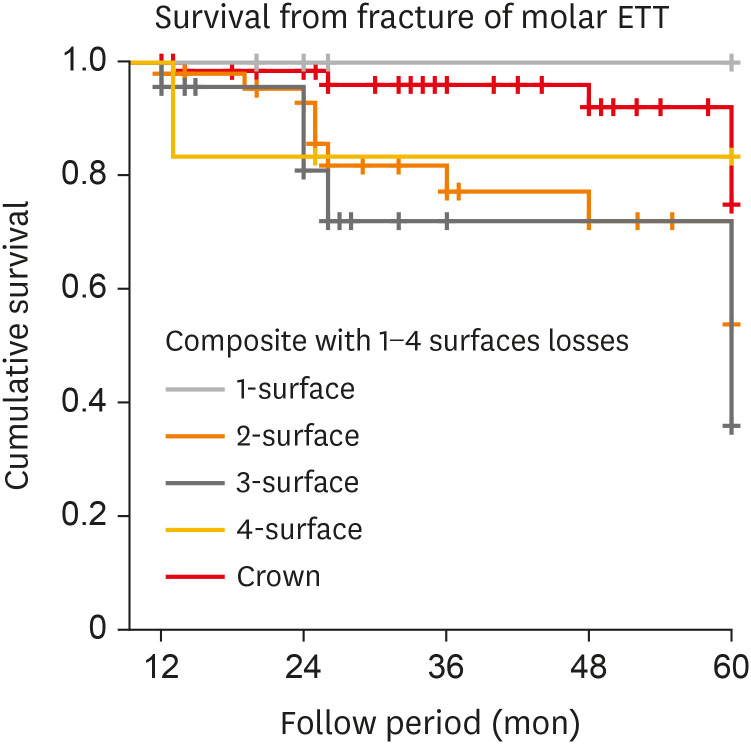
The distribution of ETT restored with resin composite restorations according to the amount of tooth structure loss was as follows: 1-surface loss: 9 teeth, 2-surface loss: 48 teeth, 3-surface loss: 23 teeth, and 4-surface loss: 8 teeth. The fracture survival rates of the ETTs with 1 to 4 surfaces lost were 100% (9 of 19 teeth), 79.2% (38 of 48 teeth), 78.3% (18 of 23 teeth), and 87.5% (6 of 8 teeth), respectively (Table 4). The Kaplan-Meier survival analysis of molar ETT restored with resin composite restorations according to the amount of tooth structure lost, in comparison to ETT with full-coverage crown restorations, is presented in Figure 3. A significant difference was found in the survival rate between ETT restored with resin composites with 2-3 surfaces lost and those restored with crowns (p < 0.05).
Table 4
Fracture survival rate of molar endodontically treated teeth (ETT) restored with resin composites according to tooth structure loss, in comparison to those restored with crowns
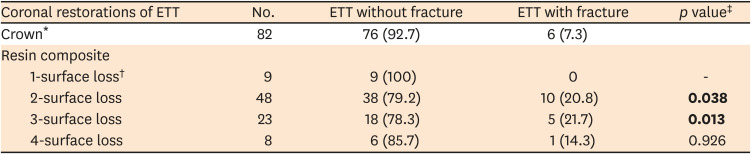
Values are presented as number (%). The bold letters indicate a statistically significant difference.
*The number of surfaces lost could not be identified, so the overall data are presented; †The p value was not calculated because no cases of ETT fracture with 1-surface loss restored with resin composite were identified; ‡The log-rank test (p < 0.05) was used to compare fracture survival rates between the subgroups of resin composite and the crown group.
Figure 3
Kaplan-Meier survival analysis of molar endoscopically treated teeth (ETT) restored with resin composite restorations according to the different amounts of tooth structure losses, in comparison to ETT restored with full-coverage crowns. The survival rates from fracture of molar ETT restored with resin composites with 1–4 surfaces lost and crowns were 100%, 79.2%, 78.3%, 85.7%, and 92.7%, respectively. In comparison to ETT with crowns, a significant difference was shown for ETT restored with resin composites that had 2- or 3-surface loss (p < 0.05).
Fracture survival rate of endodontically treated teeth restored with full-coverage crown restorations
For ETT restored with crowns, the types of posts were as follows: without posts: 20 teeth, prefabricated fiber posts: 38 teeth, and metal posts: 24 teeth. ETT with prefabricated fiber posts showed a higher survival rate (97.4%; 37 of 38 teeth) than ETT without posts (90.0%; 18 of 20 teeth) and cast metal posts (87.5%; 21 of 24 teeth), but a significant difference was not found (p > 0.05).
DISCUSSION
The present study is the first clinical study to compare the fracture survival rate in molar ETT between full-coverage crowns and resin composite restorations. The overall survival rate from fracture for molar ETT with full-coverage crowns was higher than that for molar ETT with resin composite restorations. This is consistent with previous studies that reported a high survival rate of ETT restored with crowns [51320]. These results have encouraged dental practitioners to generally plan and provide full-coverage restorations for molar ETT after endodontic treatment.
However, the amount of remaining tooth structure significantly affected the survival rate and should therefore be carefully considered before restorative planning. The present study showed the highest survival rate in molar ETT with 1 surface lost that were restored with resin composite restorations, and this rate was similar to the survival of ETT with crowns. The results might be attributed to the fact that the existence of mesial and distal marginal ridges preserves structure integration and prevents cuspal fracture in ETT [1112]. Several studies reported a higher survival rate of molar ETT when more tooth structure remained [1719]. Therefore, molar ETT with tooth structure loss limited to the occlusal surface could be successfully restored with direct resin composite restorations.
Cuspal coverage restoration is considered to be an appropriate treatment to improve the longevity of ETT, especially for molars with absent marginal ridge integrity. In our results, the 1- to 2-year survival rate of full-coverage crowns was significantly higher than that of resin composite restorations, while no difference was found in the longer observation period (more than 2 years), which is similar to what has been reported in previous studies [1320]. It can be suggested that molar ETT have a higher risk of fracture if not protected by a full-coverage restoration, especially during the first 2 years postoperatively. However, for molar ETT with suitable conditions that survive for more than 2 years, crown placement might not be required.
The magnitude of occlusal force is the greatest in the molar region [21]. A previous study showed that the survival rate of ETT was significantly lower in molar ETT than in other teeth [7]. In addition, the present study demonstrated a 2-3 times higher incidence of unrestorable fractures, even though the difference was not significantly different, in the mandibular molars than in the maxillary molars; a similar distribution has also been reported in other studies [722]. The anatomical structure of mandibular molars might be a cause for the non-significantly higher risk of coronal and radicular fracture when compared to maxillary molars [23242526].
In the present study, the number of proximal contacts (adjacent teeth) was not a significant factor affecting the fracture survival rate of molar ETT, regardless of the type of restoration. In contrast, other studies demonstrated that 2-side proximal contact improved the survival rate in premolar ETT that received both vertical and lateral occlusal forces [11327]. Theoretically, the presence of adjacent teeth might help in occlusal force distribution and reduce the risk of tooth fracture; however, this effect was not observed in molar ETT, which mainly received vertical forces.
The magnitude of the occlusal force is directly influenced by the presence and type of opposing dentition. Functional and parafunctional forces have been reported to be significant factors contributing to the survival of molar ETT [2128]. An opposing natural tooth or fixed-abutment prosthesis provides higher occlusal force on molar ETT than occurs with a removable prosthesis or in the absence of opposing dentition. However, the opposing dentition had no effect on the survival rate from fracture of molar ETT in this study. This contradictory result may be indirectly related to the very low number of samples in the group with an opposing removable prosthesis or no opposite dentition.
Improper post space preparation often weakens the ETT, which is the primary cause of catastrophic fracture, particularly for metal posts. In the present study, the majority of crown restorations for molar ETT in this study had been restored with prefabricated post or without a post. Post placement was not shown to be a significant factor affecting the survival rate of molar ETT, regardless of the type of post. In correspondence with previous studies, 2 factors (an adequate remaining coronal wall and large dimensions of the pulp chamber) provided adequate retention for core build-up in the present study, and these factors should be considered for post placement in molars [293031]. Nevertheless, a non-significantly higher survival rate was observed in the molar ETT with prefabricated fiber posts (97.4%) than in those with metal posts (87.5%). Further research should investigate the influence of the post (or absence of a post) on the survival rate from fracture in a larger population to reach a conclusion.
Within the limitations of this retrospective cohort study, the fracture survival rates of molar ETT with full-coverage crowns were higher than those with direct resin composites in the first 2 years after restorations. However, molar ETT with 1-surface (occlusal) loss were successfully restored with resin composite restorations, without any incidence of fracture over the recall period. It should be noted that the loss of marginal ridge integrity might be a significant factor to consider for crown restorations in molar ETT. A randomized controlled clinical trial should be further conducted to support these clinical findings.
CONCLUSIONS
The overall fracture survival rate of molar ETT restored with full-coverage crowns was higher than that of ETT restored with resin composite restorations. The survival rates of ETT with resin composites and crowns were only significantly different during the period of 12–24 months. The long-term survival rates (24–60 months) were not significantly different. Molar ETT with tooth structure loss on only the occlusal surface could be successfully restored with resin composite restorations.
 XML Download
XML Download