

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The main aim of root canal treatment is eradication of the endodontic microbial biofilm, which may cause an inflammatory reaction in the periapical tissues, through disinfection and sealing of the root canal space [1]. Successful endodontic therapy therefore relies on adequate mechanical shaping, a copious and effective irrigation protocol, and 3-dimensional (3D) obturation of the root canal system [2]. Finally, a proper coronal seal preventing micro-leakage is essential to obtain long-term clinical success [3].
The ideal root canal obturation should provide filling material that reaches the cemento-dentinal junction [4]. This point is subject to strong individual variability: its distance from the radiographic apex ranges from 0 to 3 mm and can be altered by inflammatory processes [5]. Therefore, no general consensus existed in the prior literature regarding the apical limit of the obturation: on the basis of Kuttler's anatomical studies of the cement-dentinal junction [6], some authors argued that instrumentation and obturation of the canals should end 0.5–2 mm before the radiographic apex, while others recommended debridement and obturation until the radiographic apex is reached [7]. The electronic apex locator (EAL) is currently recognized as a valid instrument for identifying the apical constriction and determining the working length as an alternative to the radiographic method, and the same authors suggested that working length determination using an EAL may perform better than radiography [8].
Root canal obturation is one of the most important factors contributing to the success of endodontic therapy. It is generally accepted that the filling material should be entirely confined to the root canal space. The extrusion of filling materials beyond the radiographic apex is described as overfilling, which can occur owing to the lack of apical constriction, as a result of inflammatory apical root resorption or an incompletely formed root apex, and due to over-instrumentation because of errors in working length assessment [9]. In the literature, there are still very discordant opinions concerning the likelihood that overfilling will compromise endodontic therapy. The aim of this case series was to present a long-term follow-up (up to 35 years) of 6 clinical cases involving accidental overfilling at the moment of root canal treatment.
CASE REPORT
Four cases with 10-year follow-up
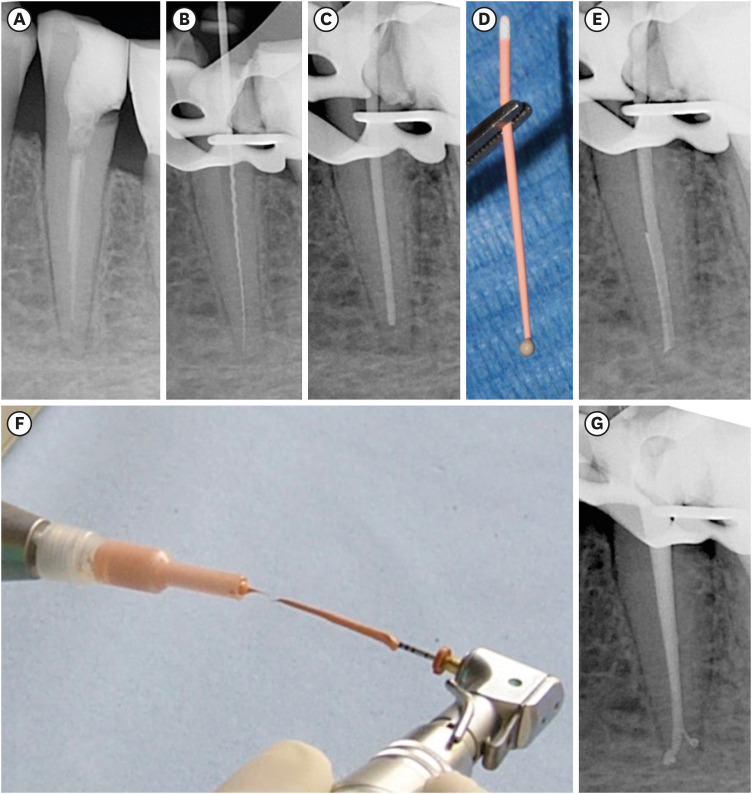
Four patients were referred for the evaluation and treatment of a lower right second premolar (Figure 1A-1D), a lower left second premolar (Figure 2A-2D), a lower right canine and first premolar (Figure 3A-3E), and a lower left first molar (Figure 4A-4F), respectively. The preoperative radiographs of all cases (Figures 1A, 2A, and 4A) showed the presence of a periapical radiolucency, except for 1 (Figure 3A). It was re-treated in only 1 case (Figure 1A). In all clinical cases, after rubber dam isolation, the old restorations and root canal filling materials, if present, were removed (Figure 1B). The pulp chamber was opened using high-speed rotating diamond-coated burs and the root canal orifices were located using low-speed carbide burs and/or endodontic ultrasonic tips under magnification using a dental operating microscope (Figure 4B). After the scouting phase and establishing the working length (Figures 2B, 4C, and 4D), all root canals were shaped using Mtwo instruments (VDW, Munich, Germany) using the simultaneous technique, irrigated with 5% sodium hypochlorite (NaOCl) alternating with 17% ethylenediaminetetraacetic acid (EDTA) and finally obturated with warm preheated thermoplasticized gutta-percha (MicroFlow, Microseal system, Sybron Endo, Orange, CA, USA), and sealer corresponding to Rickert's formula (Pulp Canal Sealer, Sybron Endo) according to the hybrid Microseal/PacMac obturation technique refined by 1 of the authors of the presented cases [10]. The Microseal obturation technique involves the use of preheated gutta-percha inserted inside the root canal, applied on a conical ISO 25 0.04 PacMac (Sybron Endo) introduced up to 2–3 mm from the apex, and activated at 6,000–7,000 rpm (Figure 5A-5G). The first to describe this technique in 1993 was John T. McSpadden [11], who referred to it as the multiphase gutta-percha obturation technique. Since then, some modifications have been made to this technique, which was later named Microseal [1213], such as the use of a 0.2 tapered gutta-percha master cone brought to 1 mm from the working length to limit overfilling [10]. The quantity of sealer used in the Microseal technique is very minimal; the master cone of gutta-percha only gets dirty at the tip (Figure 5D), and the canal is filled by the preheated preplasticized gutta-percha applied to the PacMac instrument (Figure 5F-5G).
Figure 1
Case 1, lower right second premolar. (A) Preoperative radiograph of the lower right second premolar. (B) Intraoperative radiograph after removal of the old filling material. (C) Postoperative radiograph showing slight overfilling. (D) Radiograph after 10 years of follow-up.
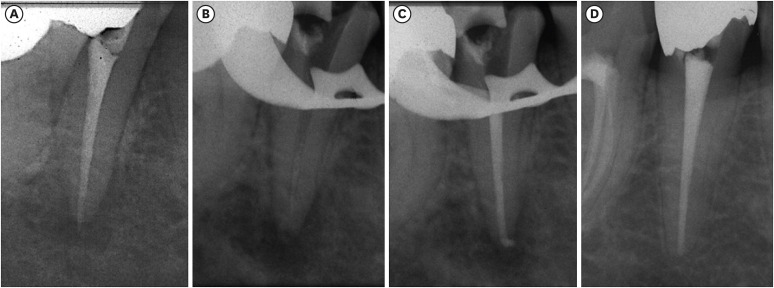
Figure 2
Case 2, lower left second premolar. (A) Preoperative radiograph of the lower left second premolar. (B) Intraoperative radiograph working length determination. (C) Postoperative radiograph showing a slight overfilling. (D) Radiograph after 10 years of follow-up.
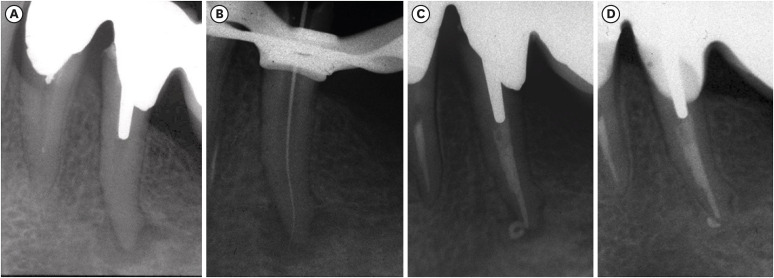
Figure 3
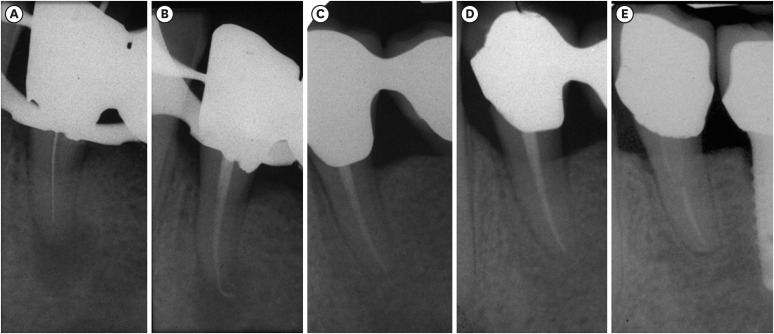
Case 3, lower right canine and premolar. (A) Preoperative radiograph of the lower right canine. (B) Postoperative radiograph showing slight overfilling of the canine. (C) Postoperative radiograph (5 years), showing the lower right premolar, which was part of a porcelain fused to metal (PFM) bridge with the first molar on the preoperative radiograph. (D) Postoperative radiograph of the lower right premolar showing a slightly short root canal filling. (E) Radiographic follow-up 10 years after the canine was restored with radiolucent composite resin and 5 years after the first premolar was covered by the crown of the PFM bridge.
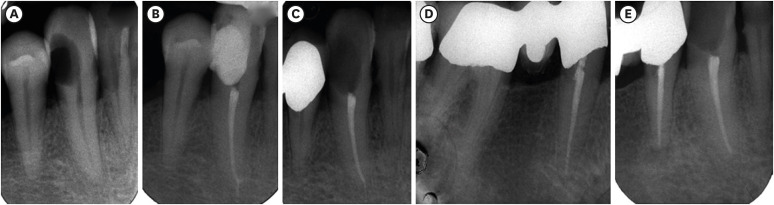
Figure 4
Case 4, calcified right lower first molar. (A) Preoperative radiograph showing a calcified pulp chamber with narrow root canals and a large area of radiolucency. (B) Intraoperative clinical image taken during access of the pulp chamber and root canal location. (C and D) Intraoperative radiograph of working length determination in the mesial and distal canals, respectively. (E) Postoperative radiograph with overfilling. (F) Follow-up after 10 years.
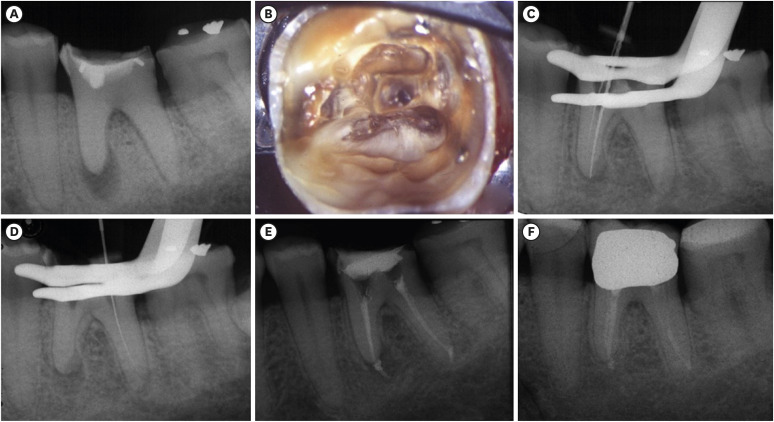
Figure 5
Microseal technique. (A) Preoperative radiograph. (B) Radiograph after removing the old root canal filling and measuring the working length. (C) Radiograph of trying the master cone of gutta-percha at a 1 mm working length without sealer. (D) Amount of sealer used with the gutta-percha master cone. (E) Radiograph after inserting the master cone of gutta-percha with sealer into the canal and lateral compaction with a spreader. (F) Microflow of preheated preplasticized gutta-percha and the PacMac instrument. (G) Postoperative radiograph after placement of preplasticized gutta-percha.
Overfilling occurred during obturation in all cases (Figures 1C, 2C, 3B, and 4E), but the radiographic follow-up at 10 years showed complete or almost complete resorption of the filling material beyond the apex and healing of the periapical lesions or maintenance of healthy periapical status (Figures 1D, 2D, 3E canine, and 4F). Radiographic follow-up (Figure 3E) showed healing of the lower canine restored with radiolucent composite resin, but also a periapical lesion on the first lower right premolar contiguous to the canine, part of the porcelain-fused-to-metal (PFM) bridge, where 5 years earlier slightly short canal filling was performed (Figure 3C and 3D).
A case with 20-year follow up
A 50-year-old male patient was referred for evaluation and treatment of the lower left right first premolar tooth (Figure 6A-6E). The patient had no pain and the clinical examination revealed a moderate tenderness to percussion without a sinus tract. The diagnosis of chronic apical periodontitis was made for the tooth, which needed to be treated. For economic reasons, the old PFM bridge was preserved and the endodontic treatment was performed through the PFM crown covering the tooth. After rubber dam isolation, the root canal was negotiated (Figure 6A), shaped according to the manual technique using stainless-steel K and H files, irrigated with 5% NaOCl alternating with 17% EDTA, and finally obturated with preheated thermoplasticized gutta-percha (Sybron Endo) and sealer corresponding to Rickert's formula (Pulp Canal Sealer, Sybron Endo) according to the Microseal technique. During obturation, overfilling occurred (Figure 6B), but the radiographic follow-ups at 1, 10, and 20 years showed complete resorption of the filling material beyond the apex and the healing of the periapical lesion (Figure 6C-6E). Curiously, in the last follow-up radiograph, after insertion of a fiber post to retain a new single PFM crown, the obturation material seemed short of the radiographic apex, showing that the resorption of filling material may also continue inside the apical root canal space, as evidenced by a thin radiopaque border at the apex of the tooth, suggesting the formation of new hard tissue (Figure 6E).
Figure 6
Case 5, lower first premolar. (A) Lower left first premolar, part of a porcelain fused to metal bridge: intraoperative radiograph during working length determination. (B) Postoperative radiograph showing accidental overfilling. (C) Follow-up radiograph after 1 year. (D) Follow-up radiograph at 10 years. (E) Follow-up radiograph after 20 years.
A case with 35-year follow-up
A 26-year-old female patient was referred for evaluation and treatment of the upper right central and lateral incisor (Figure 7A-7G). The patient had pain and clinical signs of abscess, and both elements were unresponsive to thermal pulp sensibility tests. A preoperative radiograph showed the presence of a radiolucency between the middle and apical third of the root of the lateral incisor, with a direct communication between the endodontium and the periodontium (Figure 7A). The diagnosis of internal root resorption with apical chronic periodontitis was made for the lateral incisor, which needed to be treated with endodontic orthograde therapy combined with surgical therapy. Instead, the diagnosis of asymptomatic irreversible pulpitis was made for the central incisor. Both incisors had incongruous obturation, and under the filling of the lateral incisor there was a layer of cement-like material for capping the pulp. Under rubber dam isolation, both elements were instrumented with stainless-steel K and H files, irrigated with 5% NaOCl, and obturated with a large calibrated gutta-percha master cone (Sybron Endo) and sealer corresponding to Rickert's formula (Pulp Canal Sealer) following the cold lateral condensation technique. Overfilling occurred in both teeth (Figure 7B). In the same operative session, surgical therapy was performed to remove the apical fragment of the lateral incisor without performing retrograde preparation and obturation. Subsequently, both incisors were reconstructed with direct composite resin.
Figure 7
Case 6, upper right central and lateral incisor. (A) Preoperative radiograph of the upper right central and lateral incisor. (B) Postoperative radiograph showing overfilling on both teeth. (C) Follow-up radiograph after 20 months. (D) Follow-up radiograph after 10 years. (E) Follow-up radiograph after 25 years. (F) Follow-up radiograph after 30 years. (G) Follow-up radiograph after 35 years; healing of the central incisor appeared to be stable, while a new periapical lesion seemed to have appeared in the latter incisor.
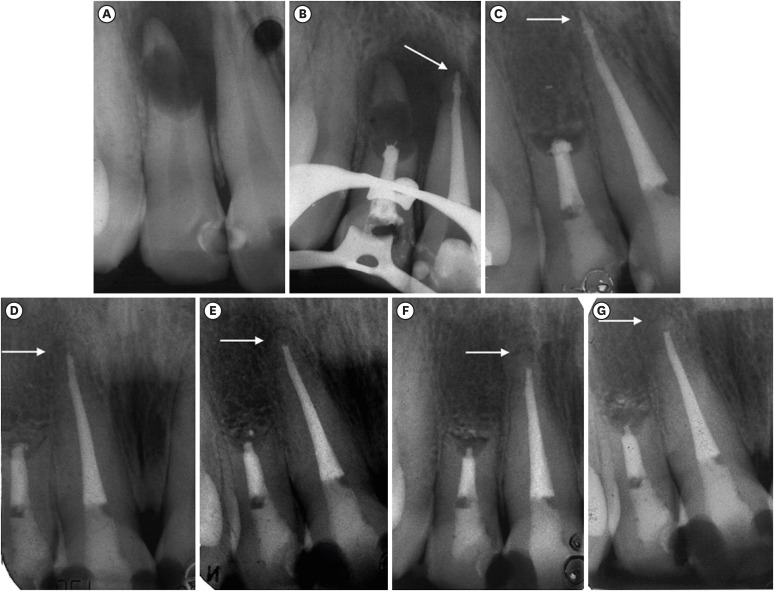
Radiographic follow-ups at 20 months, 10 and 25 years showed healing with complete disappearance of the periapical lesion (Figure 7C-7E); the 30-year radiographic follow-up revealed a still minimal presence of the overfilling material in the lateral incisor with a clearly distinguishable reduction in the diameter of the calibrated gutta-percha master cone at the apex. In the central incisor, complete resorption of the last millimeters of the gutta-percha filling material was observed (Figure 7, white arrow), with the formation of a radiopaque bridge closing the apex (Figure 7F). After another 5 years, at the 35-year follow-up, the patient did not report symptoms and there was no mobility, and on a radiographic evaluation, the apex of the central incisor appeared to be stable. On the contrary, in the area of the lateral incisor, it was possible that reabsorption of the gutta-percha and root was continuing (Figure 7G) and a new periapical lesion seemed to have appeared, probably due to loss of the apical seal.
DISCUSSION
Several in vitro research studies have reported relevant cytotoxic effects of both gutta-percha and root canal sealers [14]. When extruded beyond the apex, these obturation materials could act as foreign bodies, inducing histological reactions ranging from simple periradicular inflammation to more severe necrosis of the periodontal ligament [15]. On this basis, some authors argued that root canal obturation short of the radiographic apex may improve the prognosis of endodontic treatment, while overinstrumentation and overfilling may reduce its success rate [416]. Nevertheless, the present case series indicates that, in the presence of a 3D seal at the apex, overfilling may not affect the clinical outcome negatively.
In order to understand these results, it is important to understand the difference between overextension and overfilling of a root filling. Overfilling is defined as a case in which the obturation material fills and seals the whole canal space and extrudes beyond the apex, while overextension describes a case in which the material extrudes beyond the apex without filling and sealing the whole canal space [9], thus leaving voids which may leak and act as bacterial reservoirs and worsen the clinical outcomes [1217]. Distinguishing between these situations on radiography is possible, although difficult: overextension is characterized by a radiopacity that is discontinuous in the apical third, where the gutta-percha does not completely fill the root canal volume (Figure 1A), while overfilling appears as a continuous radiopacity for the entire canal length (Figure 1C).
Thus, it appears evident that the success rate reduction related to overfilling described in the literature does not directly depend on the material extruded in the periapical tissues, but is instead mainly due to residual infection in the root canal space and the absence of an adequate 3D seal at the apex, which allows nutrition to be supplied to the residual bacteria [18]. The absence of an adequate 3D seal at the apex can also occur when making a root canal filling that may appear to be slightly short on an X-ray examination; this probably happened in the case of a first lower right premolar that was part of a PFM bridge (Figure 3C) with slightly short obturation (Figure 3D) and which showed the development of a periapical lesion after 5 years (Figure 3E). It is important to underline that in both root canal treatments, the same protocol of adequate disinfection by irrigation was performed.
While some root canal filling materials used in the past were considered cytotoxic and responsible for persistent inflammation when extruded beyond the apical foramen [15], currently used obturation materials are either biocompatible or slightly cytotoxic only before setting [19]. Specifically, gutta-percha is a relatively inert material with low cytotoxicity that is well tolerated by the periradicular tissues [20]. In an in vivo rabbit dentin implant study, Gutierrez et al. [21] reported that in the absence of bacteria, extruded gutta-percha was removed by cells loaded with a granular substance, macrophages, until it was completely absorbed; the authors reported that clinically, gutta-percha produced the same type of reaction in the periapical zones of human teeth as those found in the dentin implants, since it disintegrated in the same manner and was later removed by macrophages until it was completely absorbed. This aligns with the observations of gradual disappearance in the present case series. Furthermore, several authors (even many years ago) documented cases of overfilling with subsequent resorption of the gutta-percha over 13 years of follow-up [22]; other authors documented, in a case report using scanning electron microscopy, successful healing of a periapical lesion with overfilling and subsequent deposition of calcified tissue at the root apex [23]. In a retrospective study of the long-term radiographic outcomes of 220 root canal treatments and root canal retreatments with unintentional root canal overfilling, the teeth overfilled with gutta-percha were not associated with a negative healing process, and in some cases extruded gutta-percha was completely reabsorbed from the periapex [24].
Similar clinical radiographic findings were observed in the cases presented herein, in which the material beyond the apex had been resorbed to such an extent that, at a long-term follow-up, the initial overfilling appeared to be a root canal filling even short of the radiographic apex of the canine (Figure 3E), first premolar (Figure 6E), and central incisor (Figure 7D-7G), and a thin radiopaque border was appreciable at the apex itself. However, if this does not occur and there is simultaneous resorption of the calibrated gutta-percha master cone and the root apex, it is important to note that loss of the seal could occur over time and a periapical lesion could develop again, as in the case of the lateral incisor after 35 years of follow-up (Figure 7G).
These findings lead to the hypothesis that, in a relatively bacteria-free environment, gutta-percha resorption is not limited to the periapical tissues, but may also happen in the inner portion of the canal at the apex, in order to create a biological barrier of dental/periodontal tissue at the anatomical apex itself. If this occurs, as is possible to visualize on radiography, it would seem to be a radiographic sign of stable periapical health over long-term follow-up. However, further studies are needed to analyze the histologic nature of these tissues to support this hypothesis and the use of 3D imaging in radiography. Although overfilling should ideally be avoided, if proper decontamination is performed and a 3D seal is obtained at the apex, overfilling may only be responsible for a possible delay in the healing process [17] and slight potential discomfort for the patient during the obturation procedures and the immediate postoperative phase [16].
CONCLUSIONS
Within the limitations of a case series, it is possible to report that, provided proper disinfection and a 3D seal of the apical third, an accidental overfilling of root canal sealer and gutta-percha in the periapical tissues may not adversely affect the long-term outcomes of root canal treatment.
 XML Download
XML Download