

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Endodontic sealers are critical materials for the obturation phase of non-surgical root canal treatment (NSRCT) [1]. Improved NSRCT outcomes are associated with void-free sealer interfaces [2]. Voids at sealer interfaces are affected by the insertion rate of gutta-percha (GP) points coated with a sealer, the application method of sealer in the canal, the rheological properties of sealers, and atmospheric pressure [34]. A sealer that adapts well to the dentin helps to ensure void-free obturation to prevents apical or coronal microleakage [56]. Superior clinical sealing to minimize microleakage is created when the sealer, GP, and dentin are in intimate contact. Dyes, tracers, and bacteria have been used to examine the hermetic sealing but are no longer considered suitable for scholarly publication [3]. Microleakage usually occurs along with the interface between the dentin and the sealer [7]. Understanding the presence and location of voids in the obturated canal may improve NSRCT outcomes.
The single-cone technique is a viable obturation option in NSRCT when using a tricalcium silicate sealer such as EndoSequence BC sealer [89]. However, the single-cone technique has not been explored for other sealer types, including the widely studied epoxy resin sealer AH Plus [3]. ActivGP glass ionomer sealer is available from Brasseler (Savannah, GA, USA); however, Shofu Inc. (Kyoto, Japan) is developing an endodontic sealer using their proprietary surface pre-reacted glass ionomer (S-PRG) fillers designated as “Giomer” technology [10]. The S-PRG fillers release antibacterial ions [1011]. Such S-PRG fillers have been used in commercial restorative resins and cements. The prototype S-PRG sealer exhibits antibacterial and anti-inflammatory effects, induces osteogenesis in the apical bone [1213].
Several studies have reported the percentage of voids for single-cone obturation with AH Plus epoxy resin sealer (Dentsply Sirona, Konstanz, Germany), EndoSequence BC tricalcium silicate sealer (Brasseler), and ActivGP glass ionomer sealer (Brasseler) [1415]. However, these studies did not identify the locations of the voids. Scanning electron microscopy (SEM) has been used to observe interfaces, but this technique requires sample destruction [161718192021].
This study used non-destructive 3-dimensional (3-D) image analyses from X-ray micro-computed tomography (µCT). Multiple sagittal 2-dimensional (2-D) images were examined by rotating the cross-section view around the central axis of a tooth using image display software. Then 2-D images of the dentin-sealer and GP-sealer interfaces were evaluated precisely without sample destruction.
The hypothesis in this study was that the single-cone technique with the prototype S-PRG sealer obturates as well as AH Plus and EndoSequence BC sealers. The aims of this study were to compare voids in single-cone obturation among AH Plus, EndoSequence BC, and prototype S-PRG sealers, and to determine the percentage of sealer contact at the dentin and GP interfaces using µCT in vitro.
MATERIALS AND METHODS
Collection of extracted human teeth and root canal preparation
Fully erupted, human permanent maxillary anterior teeth, without caries or defects, were collected from local oral surgeons and stored in 10% formalin solution until use (Institutional Review Board#: 010617-005, University of New England, not human subject research). The teeth, extracted for treatment unrelated to this study, were placed under running water for 1 hour, then cleaned for this study with a scaler. Radiographs were taken to exclude teeth with multiple canals, cracks, fractures, resorption, caries, immature apices, or root curvature more than 10°.
Fifteen teeth were selected for NSRCT, and the working length was determined to be 1 mm short of the apex using a size 10 K-file. Canals were cleaned and shaped using ProTaper NEXT (Dentsply Sirona, Johnson City, TN, USA) NiTi rotary files with a ProMark torque-limited electric motor (Dentsply Sirona, Tulsa, OK, USA) to size X5 (#50/variable taper, a 6% taper in a 3 mm tip) using copious 2.5% NaOCl irrigation. The canals were dried by ProTaper NEXT absorbent points (Dentsply Sirona, Johnson City, TN, USA).
Root canal filling with gutta-percha point and 3 endodontic sealers
The fifteen cleaned and shaped teeth were randomly divided into 3 groups (n = 5) for single-cone obturation with GP and a sealer: AH Plus, EndoSequence BC, or prototype S-PRG. The teeth were fitted with a variable-taper GP point (ProTaper NEXT GP point X5, Dentsply Sirona, Johnson City, TN, USA) to match the ProTaper NEXT NiTi rotary files size X5. Sealers were mixed (where necessary) and promptly applied to the GP point within their standard working times summarized in Table 1 [81122]. The GP point was inserted in the canal to working length with the sealer, cut with a heated Calamus Pack (Dentsply Sirona, Johnson City, TN, USA) obturation system at the cemento-enamel junction, and condensed vertically with an endodontic plugger. All teeth were cleaned and obturated by one operator, and no temporary filling material was applied to the access opening.
Table 1
Endodontic sealers evaluated
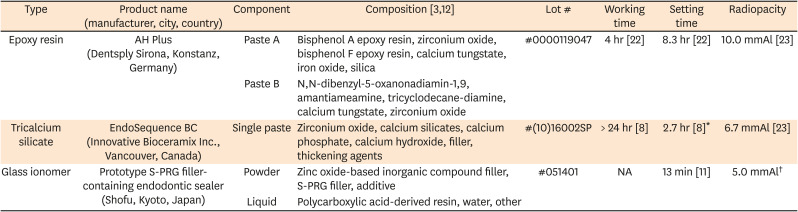
| Type | Product name (manufacturer, city, country) | Component | Composition [312] | Lot # | Working time | Setting time | Radiopacity |
|---|---|---|---|---|---|---|---|
| Epoxy resin |
AH Plus (Dentsply Sirona, Konstanz, Germany) |
Paste A | Bisphenol A epoxy resin, zirconium oxide, bisphenol F epoxy resin, calcium tungstate, iron oxide, silica | #0000119047 | 4 hr [22] | 8.3 hr [22] | 10.0 mmAl [23] |
| Paste B | N,N-dibenzyl-5-oxanonadiamin-1,9, amantiameamine, tricyclodecane-diamine, calcium tungstate, zirconium oxide | ||||||
| Tricalcium silicate |
EndoSequence BC (Innovative Bioceramix Inc., Vancouver, Canada) |
Single paste | Zirconium oxide, calcium silicates, calcium phosphate, calcium hydroxide, filler, thickening agents | #(10)16002SP | > 24 hr [8] | 2.7 hr [8]* | 6.7 mmAl [23] |
| Glass ionomer |
Prototype S-PRG filler-containing endodontic sealer (Shofu, Kyoto, Japan) |
Powder | Zinc oxide-based inorganic compound filler, S-PRG filler, additive | #051401 | NA | 13 min [11] | 5.0 mmAl† |
| Liquid | Polycarboxylic acid-derived resin, water, other |
Micro-computed tomography scanning and image analysis of teeth
Each tooth was scanned by x-ray µCT (SkyScan1272, Bruker, Billerica, MA, USA) at 6 μm voxel size, 90 kVp, 110 μA, with 0.5 mm aluminum and 0.038 mm copper filters. All datasets were exported in the DICOM file format.
The apical 3 mm of GP was used to analyze the interfaces and apical 8 mm were measured from the tip of the GP in 2 mm increments.
Void analysis: 3-dimensional reconstruction
The volume of GP, sealer, and voids was determined with image analyzer software (CTAn v.1.18.40+, Bruker). A threshold value was defined for each image and the gray level image to a binary image. The region of interest was manually selected in each tooth from each 2 mm slice for 0–2, 2–4, 4–6, and 6–8 mm from the apex. Volumes were calculated for the regions' canal, GP, sealer, and void fractions. The mean and standard deviations were calculated in each sealer group for the 4 volumes with respect to their regions: 0–2, 2–4, 4–6, and 6–8 mm from the tip of the GP.
Interface analysis: innovative digital tooth axis rotation and transformation into sagittal 2-dimensional images
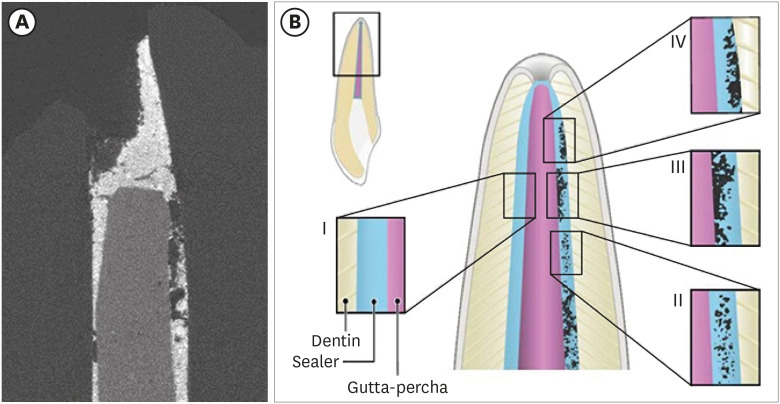
Datasets were imported for segmentation using 3-D image analysis software (Dragonfly, Object Research Systems, Montreal, Canada). Figure 1A shows a sample µCT image. Figure 1B schematically shows 4 interface types of contact. Type I is perfect contact at both the dentin-sealer and the GP-sealer interfaces. Type II shows voids within the sealer, but not at the interfaces. Type III contact is when the dentin-sealer interface is perfect, but pores exist at the GP-sealer interface. Type IV contact mode is defined as pores existing at the dentin-sealer interface, but perfect contact is present at the GP-sealer interface. Mixed modes of contact may exist.
Figure 1
A sample micro-computed tomography image and schematic of 4 contact modes in endodontic obturation.
(A) High resolution computed tomography sagittal image of tooth obturated by a gutta-percha (GP) point (center), AH Plus sealer (light grey), areas unfilled by AH Plus sealer (darkest grey), and dentin (dark grey). (B) Schematic of 4 contact modes in endodontic obturation.
Type I: perfect contact mode (both the dentin-sealer and GP-sealer interface), type II: sealer porosity mode, type III: dentin-sealer interface contact mode (a perfect contact is present at the dentin-sealer interface, but pores exist at the GP-sealer interface), type IV: GP-sealer interface contact mode (pores exist at the dentin-sealer interface, but there is a perfect contact at the GP-sealer interface).
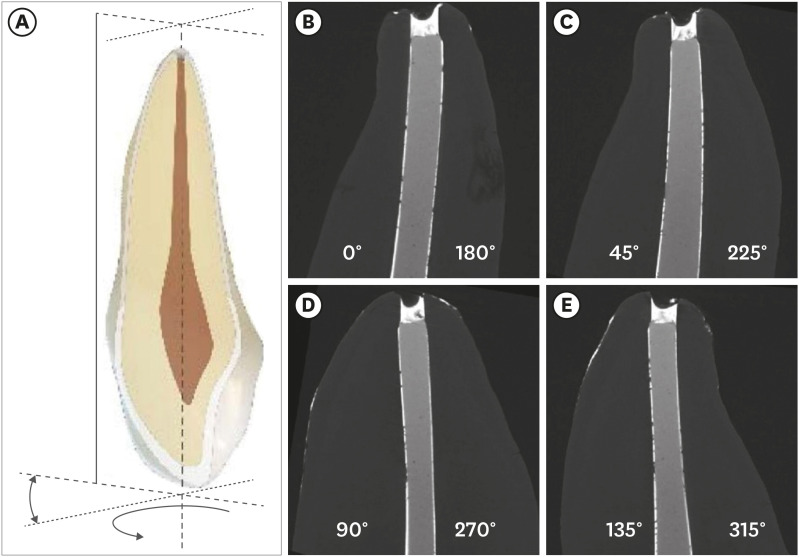
After segmentation, 3-D images were constructed around the tooth's central axis. This innovative approach used software to capture images as if the tooth were rotated around its central axis (Figure 2A). The 2-D images were recorded every 45 degrees around the central axis to obtain 4 sagittal images at 3 mm from the apex of teeth based on the importance of the apical seal [24]. High-resolution images were saved from the scans to examine the interfaces and porosity. The contact point of dentin to sealer and the GP to sealer interfaces was evaluated every 100 µm for 30 layers; these interface contacts were denoted as dentin-sealer or GP-sealer interface contacts or contacts. From the 4 sagittal images of each tooth (0°, 45°, 90°, 135°), each image provided 2 interfaces of GP and sealer and 2 interfaces of dentin and sealer. Eight interfaces of GP and sealer and 8 interfaces of dentin and sealer were evaluated to determine voids (Figure 2B-E). One operator evaluated the sealer interface to determine voids at each contact point, either no contact (0) or contact (1). Voids indicate imperfect sealing and a possible pathway for microleakage.
Figure 2
An innovative approach to rotate an image around the central axis of the tooth for interface observation. (A) Sample 2-D sagittal view from 3-D rotation of tooth around central axis. (B) Digital rotation of tooth around central axis every 45°. (B) 0°, (C) rotation 45°, (D) rotation 90°, (E) rotation 135°. Each image provides 2 views of sealer contact with dentin and 2 with gutta-percha (GP). For example, 1 image provides 2 slides, such as 0° (left) and 180° (right) in (B). The dentin-sealer and the GP-sealer interface contacts were evaluated every 100 μm (30 layers) from the apical tip of the GP, to evaluate voids (0: open) or contact (1: contact) on both sides.
Statistical analysis
To analyze voids, descriptive statistics were computed for the volumes of the canal, GP, sealer, and voids in the 3 sealer groups. The average percentages of GP, sealer, and voids from the tip of the GP to an 8 mm away were calculated and statistically analyzed using 1-way analysis of variance (ANOVA). If an ANOVA test showed significant results, post hoc test was conducted to identify which pair of sealer groups yielded significant results, and Bonferroni corrections were used. A Pearson correlation coefficient was computed to estimate the association between sealer volume and the distance from the apex.
Descriptive statistics were computed for dentin-sealer and GP-sealer interfaces, and the mean and standard deviations were calculated. Paired t-tests were conducted to examine differences in the average interfacial contact percentage between the dentin and sealer versus between the GP and sealer. Bonferroni corrections were used to adjust for multiple comparisons. The standard deviations in the average interface contact percentages were calculated with 95% confidence intervals. Pearson correlation coefficients were computed to examine the correlation between the percentage of interface contact and the distance from the apex.
All analyses were performed using the SAS/STAT 15.1 statistical package (SAS Institute, Cary, NC, USA). A p value less than 0.05 was considered statistically significant.
RESULTS
Void analysis
Table 2 summarizes the average total canal volume (mm3) and the percentages of GP, sealer, and voids in the apical 8 mm at 4 regions from the apex. No statistical differences were found in the total canal volume among the 3 sealer groups (p > 0.05), indicating the shaped canals were not statistically different among the 3 sealer groups. Furthermore, no significant differences were found in the GP volumes among the 3 sealer groups (p > 0.05).
Table 2
Average volume (mm3) and percentage (%) of gutta-percha (GP), sealer, and voids
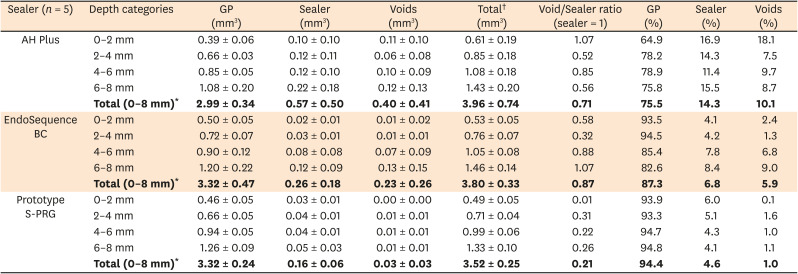
Sealer volume varied significantly among the 3 sealer groups (p = 0.001). The highest sealer volume was measured in the AH Plus group (0.57 mm3) and the lowest sealer volume in the prototype S-PRG sealer group (0.16 mm3). Sealer volume in the AH Plus group was significantly larger than the other 2 sealer groups; however, no significant difference was found in sealer volume between the EndoSequence BC and prototype S-PRG sealer groups (p = 0.38). No significant differences were detected in sealer volume among the 4 regions within each sealer group (p > 0.05).
The void volumes were not significantly different among the 3 sealers (p > 0.05). No significant differences in void volume were found among the 4 regions within each sealer group (p > 0.05). Volumes of GP, sealer, and voids at each region for each sealer were added and normalized to a percentage using GP + sealer + voids = 100%. Within the AH Plus sealer group, the percentage of voids in each region were 18.1, 7.5, 9.7, and 8.7% for 0–2, 2–4, 4–6, and 6–8 mm. Within the EndoSequence BC sealer group, the percentages of voids were 2.4, 1.3, 6.8, and 9.0%. Within the prototype S-PRG sealer group, the percentages of voids were 0.1, 1.6, 1.0, and 1.1%. The void to sealer ratio in all sealer groups varied with distance from the tip of the GP. In the 0–8 mm region of the GP, the prototype S-PRG sealer had the lowest void to sealer ratio (0.21), followed by the AH Plus sealer (0.71) and EndoSequence BC sealer (0.87).
Interface contact of sealer at dentin and gutta-percha
Figure 1B illustrates 4 interface types of contact. Based on our analysis, mixed modes of contact were detected for the 3 sealer groups.
Figure 3 illustrates the average percentage of interface contact at the dentin-sealer and GP-sealer interfaces for the apical 3 mm of GP of each sealer group. The average contact percentages of dentin-sealer interface were 82.4% ± 6.8% for AH Plus, 71.6% ± 25.3% for EndoSequence BC, and 70.2% ± 9.4% for prototype S-PRG. The average contact percentage of the GP-sealer interface was 65.6% ± 29.1% for AH Plus, 80.7% ± 25.8% for EndoSequence BC, and 87.0% ± 8.6% for prototype S-PRG. Paired t-tests were conducted to determine if significant differences occurred in the sealers' interface contact with dentin versus contact with GP. The contact at the dentin-sealer interface was significantly higher than the contact at the GP interface within the AH Plus (95% confidence interval [CI], 6.2–27.4%; p = 0.003) sealer group, but the opposite was true for the EndoSequence BC (95% CI, 2.8–15.5%; p = 0.006) and prototype S-PRG (95% CI, 12.3–21.4%; p < 0.001) sealer groups. The AH Plus sealer group had a significantly higher dentin-sealer interface (contact) ratio than the prototype S-PRG sealer group (p = 0.019) although significantly lower GP-sealer interface (contact) ratio than the EndoSequence BC (p = 0.013) and prototype S-PRG sealer (p = 0.001) groups, adjusting for the effect of multiple comparisons with Bonferroni corrections.
Figure 3
Average contact percentage at sealer interfaces for apical 3 mm (from gutta-percha [GP] tip) among 3 sealers.
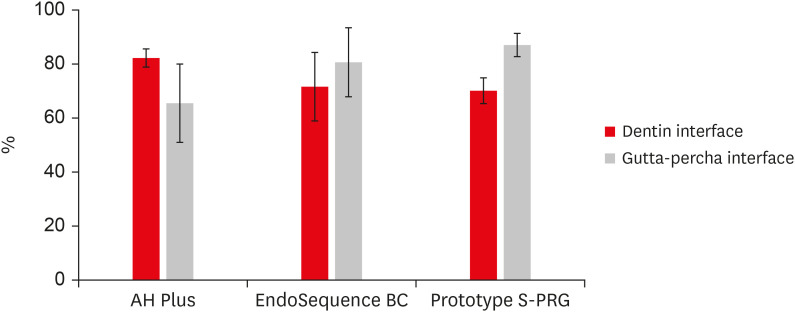
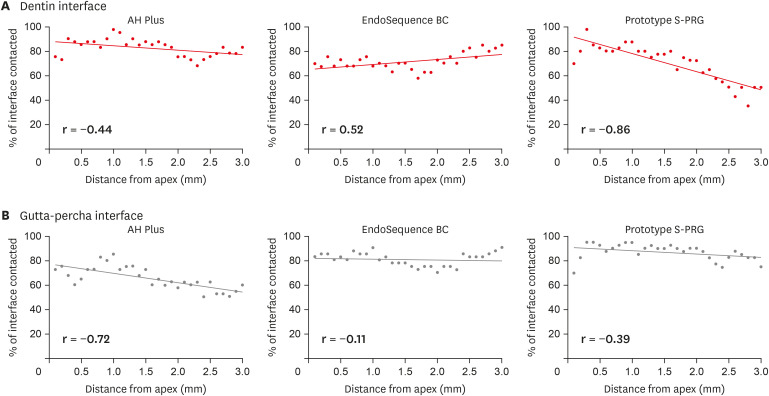
Figure 4 shows the percentage of interface contact versus distance from the apex of the GP. Linear regression was performed for each sealer and interface. The sealer contact decreased at each interface farther from the apex, indicated by a negative Pearson correlation (r). The only exception was the dentin-sealer interface with the EndoSequence BC sealer (Pearson correlation; r = 0.52). The correlation coefficients were lowest for the GP interface with the AH Plus sealer.
DISCUSSION
Previous studies have used x-ray µCT to evaluate voids and the filling quality of endodontic sealers [142526]. The present study used µCT to evaluate void and sealer volume of single-cone obturation with 3 types of sealer: epoxy resin, tricalcium silicate, and glass ionomer. Our results showed no significant statistical difference in GP volume, which allowed for void and sealer volume analysis amongst the sealers.
In the present study, the AH Plus sealer group had an average of 10.1% voids, which is in agreement with Naseri et al.'s [25] findings (between 2%–5%) for overall apical void volume when using another epoxy resin sealer (AH 26 powder-liquid sealer). However, previous single-cone obturation studies reported less than 3%, for overall void volume using the AH Plus sealer [527]. Moeller et al. [28] assessed AH Plus sealer and the lateral compaction technique using µCT and found 66% of their cross-sectional samples had voids, and porosity increased from the apical towards the cervical third; however, they did not report the percentage of voids.
The sealer volume (mm3) consistently increased with distance from the apex in the 3 sealer groups. The void volume increased with distance from the apex for the EndoSequence BC and S-PRG sealer groups. The AH Plus sealer group presented a larger void volume in the 0–2 mm (0.11 ± 0.10 mm3) than void volume in 2–4 mm (0.06 ± 0.08 mm3), although the difference was not significant. The prototype S-PRG sealer group had the lowest percentage of sealer (4.6%) and voids (1.0%) among all sealer groups. However, a previous single-cone obturation study by Celikten et al. [15] reported that EndoSequence BC sealer had the lowest percentage of voids in the apical third of root canals among AH Plus, EndoSequence BC, and ActivGP sealers.
Higher volume percentages of sealer and voids for AH Plus (14.3% and 10.1%), compared to EndoSequence BC sealer (6.8% and 5.9%) and prototype S-PRG sealer (4.6% and 1.0%), were observed in the present study. This result might be attributed to the plunging/condensing rate of GP while coated with a sealer, the method of application of sealer (in this case, a “buttered” cone), the viscosity of the sealer, or image analysis methodology. The preparation of a sealer can affect sealer porosity. Vigorous spatulation can easily develop a frothy sealer; however, static mixing tips, such as AH Plus jet or a single component sealer such as EndoSequence BC, are known to introduce less air. Only the tricalcium silicate sealers are currently commercially available in 1 paste format [3]. In GP condensation, viscosity is a quantitative parameter for evaluating the rheological properties of endodontic sealers and may help achieve an ideal flow [4]. A study by Zhou et al. [8] showed AH Plus sealer had a slightly lower flow than that of EndoSequence BC sealer, indicating higher viscosity of AH Plus sealer. However, Zhou et al. [8] reported a contradictory finding that AH Plus sealer has lower film thickness than EndoSequence BC sealer. Low film thickness is presumed to indicate lower viscosity and better ability to fill root canals but viscosity is a complex property that also depends on the shear rate.
In the present study, the void to sealer ratio ranged from 0.01 to 1.07, where a low ratio is favorable. This finding is similar to Naseri et al. [25] and Keleş et al. [14], who reported the void to sealer ratio of AH Plus sealer ranged from 0.1 to 1.3, and in this study the void to sealer ratio of AH Plus sealer was 0.52 to 1.07. The S-PRG sealer had the lowest values of void/sealer.
In addition to voids, our study examined the type and location of contact at interfaces. The AH Plus sealer had the highest percentage contact at the dentin-sealer interface, in agreement with the SEM interface study of Adhikari and Jain [17]. Also, the present µCT results agree with the SEM study of epoxy resin and EndoSequence BC sealers by Mohammadian et al. [18] in that both sealers had equal dentin contact in the apical 1/3. Polineni et al. [20] also did not find a significant difference between epoxy resin and tricalcium silicate sealers. Al-Haddad et al. [29] reported in a confocal laser study that dentin-sealer interface contact by AH Plus sealer was about 92%, and EndoSequence BC sealer was about 83%, while the present µCT study was 82% for AH Plus sealer and 72% for EndoSequence BC sealer.
The prototype S-PRG sealer (glass ionomer sealer) had only 70.2% of the dentin-sealer interface contact. Another glass ionomer sealer (Ketac-Endo) has been shown to adhere to dentin, demonstrating no separation at the sealer dentin junction in a selected SEM image [21]. On the other hand, De Gee et al. [30] showed that Ketac-Endo sealer had lower sealing capacity than AH 26 sealer (a powder-liquid epoxy resin sealer). Ketac-Endo and prototype S-PRG sealer are liquid and powder systems, whereas EndoSequence BC sealer is 1 paste and AH Plus sealer is 2 pastes. Mixing may have caused voids in glass ionomer sealers via air entrapment [21].
Extrapolating the regression curve predicts EndoSequence BC sealer has 98% of the dentin-sealer interface contact at 8 mm from the apex. Such a high percentage of contact supports an ideal coronal seal with the single-cone technique [89]. This extrapolation is in agreement with Mohammadian et al. [18] who reported the dentin-sealer interface of EndoSequence BC sealer was better sealed than that of AH Plus sealer in the middle and coronal areas of the root. A recent meta-analysis study reported the degree of leakage relative to the AH Plus sealer (1.0 as a standard) [3]. EndoSequence BC sealer had a relative leakage score of 0.78, lower than Ketac-Endo Glass ionomer and zinc oxide-eugenol sealers whose scores were the same, 1.15. This meta-analysis indicates that EndoSequence BC sealer has the lowest mean relative leakage, which is in agreement with this study. In the present study, the rank order of the dentin-sealer interface contact by Pearson correlation was EndoSequence BC sealer (r = 0.52), AH Plus sealer (r = −0.44), and prototype S-PRG sealer (r = −0.86). Figure 4 indicates the interfacial adaptation between the dentin and sealer was distance-dependent. This study found the EndoSequence BC and prototype S-PRG sealers have a higher percentage of GP interface contact than AH Plus sealer. The importance of GP-sealer interface contact for microleakage prevention needs future investigation.
The hypothesis was accepted that the single-cone technique with the prototype S-PRG sealer obturates as well as the EndoSequence BC sealer in single-cone technique with a matching size variable-taper GP point. Sealer choice is affected by factors such as the tooth being vital or non-vital or the time required before core build-up treatment [38112223]. The core build-up is a minimum 5 mm of GP distant from the apex, and this study examined up to 8 mm. The fast setting of the prototype glass ionomer sealer would be preferable for a post/core/build-up scheduled on the same day as endodontic obturation. If post/core/build-up can occur later, AH Plus sealer can be a choice for vital pulp cases because of its high dentin-sealer interface contact observed in this study. EndoSequence BC sealer may be chosen for necrotic pulp cases because its high pH creates an antimicrobial environment [3].
Our study provided interesting findings in dentin-sealer interface contact and GP-sealer interface contact, although the number of samples was limited. Future studies may compare the voids of root canal fillings utilizing larger sample groups with new materials or compare endodontic instrumentation techniques for cleaning and shaping. EDTA was not used to remove the smear layer, so no accessory filling ability was investigated because the tubules and lateral or accessory canals were obscured by the smear layer. This pilot study can guide future studies to increase sample size and decrease the labor and potential human errors in measuring interface in regions of interest by using artificial intelligence. Future studies may also investigate voids and interface contact of new root canal filling materials or endodontic instrumentation techniques that affect sealer interface contact.
CONCLUSIONS
All 3 sealers contained voids at both the dentin and GP interfaces. AH Plus sealer had the highest total void percentage, followed by the EndoSequence BC sealer and prototype S-PRG sealer. The void volume did not increase with distance from the apex for any sealer. The prototype S-PRG sealer group had the lowest void to sealer ratio, followed by the EndoSequence BC sealer and the AH Plus sealer groups. The prototype S-PRG sealer group has the same quantity of sealer contact as the other sealers for the single-cone technique to create low-void obturation.
The prototype S-PRG sealer had the best contact at the GP interface, followed by EndoSequence BC and AH Plus sealers. However, at the dentin-sealer interface, the AH Plus sealer had the highest contact, followed by EndoSequence BC and prototype S-PRG sealers.
Only the EndoSequence BC sealer had an increasing dentin-sealer interface ratio as the distance from apex increase. Contact at the GP-sealer interface of all sealers trended downward as the distance from apex increased in the first 3 mm.
 XML Download
XML Download