

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Despite countless advances in the development of adhesive systems, the degradation of bonding interfaces over time remains a challenge for restorative dentistry [1]. Several factors are related to the degradation of the resin-dentin interface, which mainly occurs through the hydrolysis and leaching of the adhesive monomers that form the hybrid layer. These processes are facilitated by the presence of water and its penetration into hydrophilic or loosely cross-linked sites [12]. Besides that, the hydrophilicity of the monomers and the presence of residual solvent and nanoleakage zones originating from naked collagen may contribute to the degradation of the resin-dentin interface [13]. In addition, regions of unprotected collagen may undergo a degradation process caused by matrix metalloproteinase enzymes and cysteine cathepsins, which can reduce the longevity of restorations [4].
Dentin biomodification through collagen cross-linking agents (CCLAs) is a strategy to improve the biomechanical and biochemical properties that can reduce the biodegradation of this tissue and preserve adhesion stability over time [56]. Multiple interactions between these agents and various extracellular components of the dentin matrix are the basis for tissue biostability and enhanced biomechanical properties of the dentin matrix. Their use has shown promising initial results in laboratory studies [7891011].
CCLAs can be applied to dentin as a pretreatment, incorporated into the adhesive system, or added to the phosphoric acid etchant [891011]. Various CCLAs have been tested, such as proanthocyanidins (PACs), epigallocatechin-3-gallate (EGCG), riboflavin and glutaraldehyde. Fawzy et al. [9] evaluated the effect of riboflavin photoactivated by ultraviolet A or visible blue light as a dentin pretreatment, and showed its ability to improve the mechanical properties of dentin collagen. This agent was able to increase and preserve the bond strength and interface integrity after short-term water storage. Daood et al. [10] assessed the effectiveness of adhesives incorporated with riboflavin and showed that they were able to increase and maintain the bond strength and interface integrity after storage in artificial saliva. Moreover, there were no adverse effects on the degree of conversion of the adhesive monomers. Subsequently, the effects of CCLAs were evaluated in clinical trials, but there is still a need for a well-established protocol regarding the application and clinical efficacy of these agents under clinical conditions [121314].
Hitherto, no systematic reviews have been published on the use of CCLAs as a strategy to improve the performance of adhesive interfaces, which could provide substantial evidence on the use of these agents in restorative dentistry.
In this context, the objective of this study was to answer the following research question through a systematic review of the literature and meta-analysis of randomized clinical trials (RCTs): are CCLAs capable of improving dentin adhesion?
MATERIALS AND METHODS
Study protocol and search information strategy
This systematic review was based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) checklist [15]. Therefore, its research question was organized according to the PICOS strategy:
1. Population (P): subjects undergoing restorative treatment with composite resin;
2. Intervention (I): application of CCLAs either separately or incorporated into the adhesive;
3. Comparison (C): no use of CCLAs;
4. Outcome (O): performance of a restorative procedure evaluated by postoperative sensitivity, the retention rate, marginal adaptation, marginal staining, or recurrence of caries;
5. Study design (S): RCTs.
The information searched was individualized for each adopted database with a combination of specific terms. Supplementary Table 1 shows additional information regarding the search strategies in this review paper. EndNote X8 (Thompson Reuters, New York, NY, USA) was chosen to manage all references and exclude duplicate articles.
Inclusion and exclusion criteria
Potential studies were required to have included an experimental group (i.e., any composite resin restorative procedure that used any CCLA associated with the adhesive strategy) and a comparative group (i.e., composite resin restorative procedure without adhesive technique-related biomimetic agents).
The following exclusion criteria were considered during the selection process: (1) non-RCT study designs (case reports, meeting abstracts, letters to the editor, book chapters, authors’ personal opinions, clinical observations, and literature reviews); (2) studies that concomitantly used a technique that may interfere with adhesion, in addition to CCLAs; (3) studies with a control group that used an adhesive system differing from that of the experimental group; and (4) studies not written in languages using a Latin (Roman) alphabet (Table 1).
Table 1
Inclusion and exclusion criteria

Database sources
Individual search strategies were performed in PubMed, Web of Science, Scopus, LILACS, Cochrane, and DOSS. The gray literature was assessed through Google Scholar and OpenGrey. The search included all articles published until October 7, 2020, without time limitation.
Study selection and data extraction
Initially, 2 investigators (JCS and ELCF) independently evaluated the titles and abstracts of all studies obtained with the search strategy. They used a web application for systematic reviews (Rayyan, Qatar Computing Research Institute, Doha, Qatar) [16]. Papers that did not appear to meet the inclusion criteria were excluded. After that, the full texts of selected articles were independently analyzed to check their eligibility. A third examiner (VPAS) critically assessed the reference lists of the selected studies. Any disagreement during the study selection process was resolved when the 2 authors reached an agreement. However, in case of disagreement, the other authors (VPAS and FWGC) participated in the final decision.
One investigator (JCS) collected data from the included studies, and a second investigator (ELCF) cross-checked all the obtained information. Any disagreements between the 2 authors were discussed until their complete resolution. The third investigator (VPAS) made the final decision when the 2 authors failed to reach an agreement. Thereafter the statistical analysis was performed by another author (PGBS).
Data items
The following aspects were evaluated for further data synthesis: (1) publication year; (2) methodological design; (3) participants (sample size, sex, and age); (4) type of cavity; (5) cavity characteristics; (6) restorative material-associated variables (CCLAs, adhesive system, composite resin, restorative technique, and curing light); and (7) outcomes of interest for the present systematic review.
Risk of bias (RoB) in individual studies
The RoB was assessed independently by 2 authors (JCS and ELCF), guided by the Cochrane checklist for RCTs [17]. Any disagreement between them over the RoB items was resolved through discussion with a third reviewer (VPAS). The following questions were used: (1) random sequence generation (selection bias); (2) allocation concealment (selection bias); (3) blinding participants and personnel (performance bias); (4) blinding outcome assessment (detection bias); (5) incomplete outcome data (attrition bias); (6) selective reporting (reporting bias); (7) other sources of bias (other bias).
The RoB was classified as high (when the study had a “yes” score of less than 49%), moderate (50%–69%), or low (70% or more), according to Haas et al. [18]. The RevMan software (Review Manager, version 5.3, Cochrane Collaboration, Copenhagen, Denmark) was used to generate the RoB figures.
Meta-analysis
After extraction, the data were imported into the RevMan software to calculate the combined relative risks of each quality parameter of restorations (Fédération Dentaire Internationale [FDI] scores) in the evaluated study periods. The outcome used was the incidence of restorations with events described by mean values from the analysis of fixed effects by the inverse variance method. The I2 coefficient assessed heterogeneity, and leave-one-out analysis (removal of studies one by one from each period) was used to assess the influence of the weight of each data on the final outcome. All analyses were conducted using a 95% confidence threshold.
Quality of the evidence
The Grading of Recommendations, Assessment, Development and Evaluation (GRADE) profiler was used to summarize the evidence quality using the GRADE pro-GDT software (http://gdt.guidelinedevelopment.org). Depending on the study design, RoB, consistency, directness, heterogeneity, precision, publication bias, and additional relevant aspects, the quality of the evidence could be downgraded by 1 or 2 levels for each aspect [19].
RESULTS
Study selection
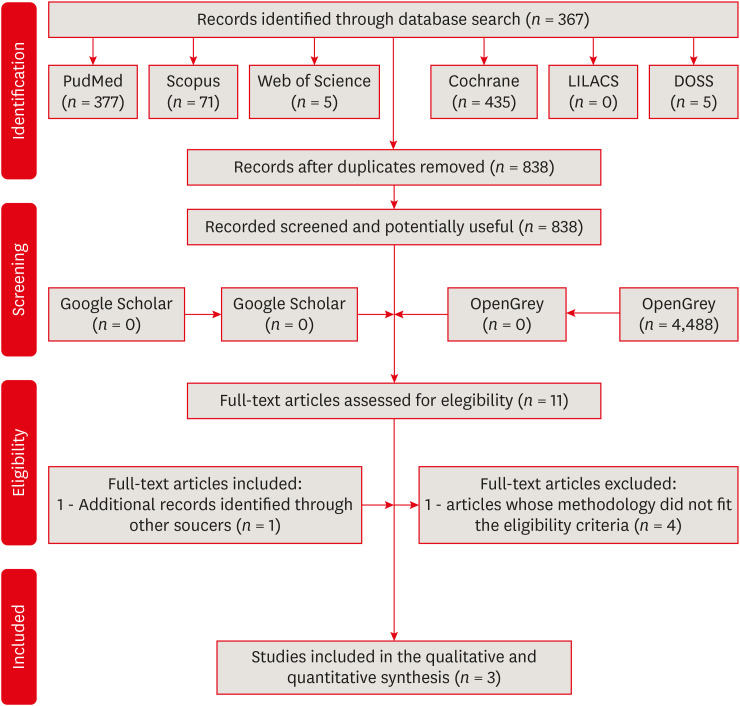
Initially, 893 articles were identified from the electronic databases. Fifty-five duplicated studies were excluded. Then, the titles and abstracts of 838 articles were screened, and 10 potentially relevant studies were selected for full-text reading. No studies were selected from the gray literature (Google Scholar and OpenGrey). Eleven articles were read for eligibility assessment according to the inclusion criteria, from which 8 were excluded due to the main exclusion criteria. Additional records identified through other sources were included (n = 1). Finally, 3 studies satisfied the inclusion criteria and were selected for this systematic review (Figure 1).
Figure 1
Flow diagram of the study identification, screening, and inclusion process. Adapted from Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA). References for the 9 excluded articles are listed in Supplementary References.
Study characteristics
The 3 included studies were from Brazil. They were published in the period from 2019 through 2020 (Table 2) and amounted to 123 participants. All restorative procedures were performed on noncarious cervical lesions (NCCLs), and the CCLAs were obtained from a natural source.
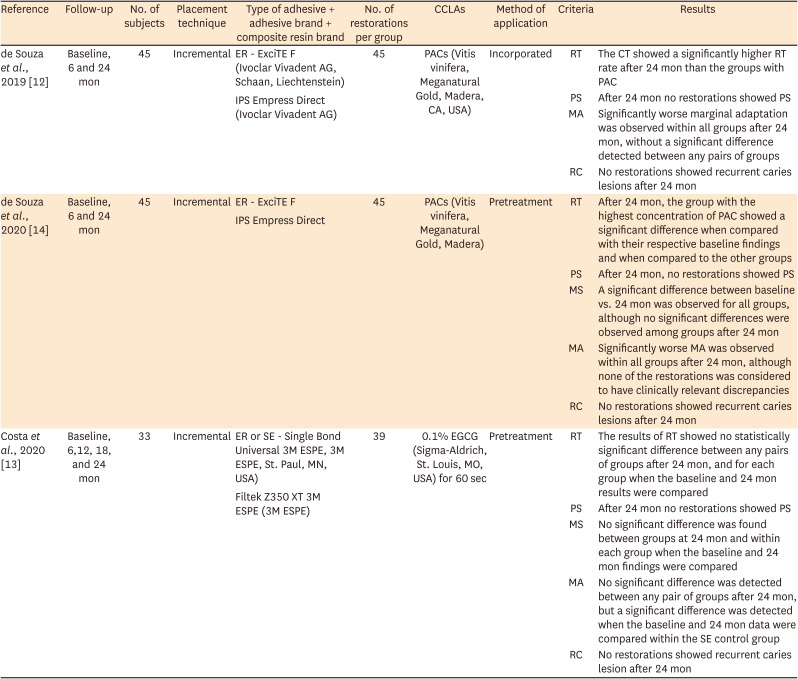
Table 2
Main data of selected articles
| Reference | Follow-up | No. of subjects | Placement technique | Type of adhesive + adhesive brand + composite resin brand | No. of restorations per group | CCLAs | Method of application | Criteria | Results |
|---|---|---|---|---|---|---|---|---|---|
| de Souza et al., 2019 [12] | Baseline, 6 and 24 mon | 45 | Incremental | ER - ExciTE F (Ivoclar Vivadent AG, Schaan, Liechtenstein) | 45 | PACs (Vitis vinifera, Meganatural Gold, Madera, CA, USA) | Incorporated | RT | The CT showed a significantly higher RT rate after 24 mon than the groups with PAC |
| IPS Empress Direct (Ivoclar Vivadent AG) | PS | After 24 mon no restorations showed PS | |||||||
| MA | Significantly worse marginal adaptation was observed within all groups after 24 mon, without a significant difference detected between any pairs of groups | ||||||||
| RC | No restorations showed recurrent caries lesions after 24 mon | ||||||||
| de Souza et al., 2020 [14] | Baseline, 6 and 24 mon | 45 | Incremental | ER - ExciTE F | 45 | PACs (Vitis vinifera, Meganatural Gold, Madera) | Pretreatment | RT | After 24 mon, the group with the highest concentration of PAC showed a significant difference when compared with their respective baseline findings and when compared to the other groups |
| IPS Empress Direct | PS | After 24 mon, no restorations showed PS | |||||||
| MS | A significant difference between baseline vs. 24 mon was observed for all groups, although no significant differences were observed among groups after 24 mon | ||||||||
| MA | Significantly worse MA was observed within all groups after 24 mon, although none of the restorations was considered to have clinically relevant discrepancies | ||||||||
| RC | No restorations showed recurrent caries lesions after 24 mon | ||||||||
| Costa et al., 2020 [13] | Baseline, 6,12, 18, and 24 mon | 33 | Incremental | ER or SE - Single Bond Universal 3M ESPE, 3M ESPE, St. Paul, MN, USA) | 39 | 0.1% EGCG (Sigma-Aldrich, St. Louis, MO, USA) for 60 sec | Pretreatment | RT | The results of RT showed no statistically significant difference between any pairs of groups after 24 mon, and for each group when the baseline and 24 mon results were compared |
| Filtek Z350 XT 3M ESPE (3M ESPE) | PS | After 24 mon no restorations showed PS | |||||||
| MS | No significant difference was found between groups at 24 mon and within each group when the baseline and 24 mon findings were compared | ||||||||
| MA | No significant difference was detected between any pair of groups after 24 mon, but a significant difference was detected when the baseline and 24 mon data were compared within the SE control group | ||||||||
| RC | No restorations showed recurrent caries lesion after 24 mon |
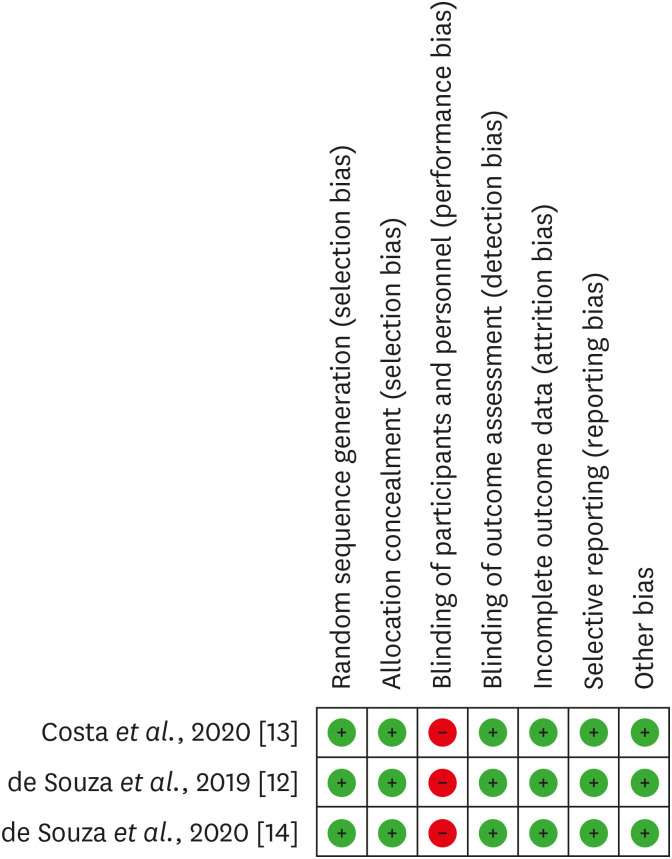
RoB within individual studies
In general, the included articles showed low RoB, with 85% of items classified as low RoB and 15% showing high RoB (Supplementary Figure 1). Regarding the individual questions of the checklist, a high RoB was observed for the blindness of the performer of the procedure, and a low RoB was attributed to the other items (Figure 2).
Results of individual studies
Methodologically, the analyzed studies were randomized and reported a double-blinded design. They performed restorative procedures on NCCLs. The composite resin insertion technique performed in all studies was the incremental type.
In 2 of these studies, CCLA application was performed as a pretreatment [1314]. In the other study, the application was performed through the incorporation of the cross-linking agent within the adhesive system. The CCLAs used were PACs and EGCG [121314].
All studies had control groups with the same adhesive system without the use of a CCLA. Two investigations used ExcitTE F (Ivoclar Vivadent AG, Schaan, Liechtenstein), and the other one used Single Bond Universal 3M ESPE (3M ESPE, St. Paul, MN, USA) [121314]. Two studies used IPS Empress Direct (Ivoclar Vivadent) composite resin, and the other study used Filtek Z350 XT 3M ESPE (3M ESPE) [121314].
The curing light devices were the Emitter A FIT (Schuster Equipamentos Odontológicos, Santa Maria, RS, Brazil) and the DB-685 (1,100 mW/ cm2, Dabi Atlante, Ribeirão Preto, Brazil) [121314].
A total of 426 restorations were performed, distributed into experimental and control groups: 39 restorations per group in Costa et al. [13] and 45 restorations per group in both de Souza et al. [12] and de Souza et al. [14]. In all studies, 2 blinded examiners performed clinical evaluations independently. The evaluators were previously calibrated and used the FDI criteria to evaluate retention, the presence of fractures, marginal discoloration, marginal adaptation, caries, and postoperative sensitivity [121314]. In the study performed by Costa et al. [13] these variables were classified as follows: clinically very good or good (scores 1 + 2), clinically sufficient/satisfactory (score 3), clinically unsatisfactory (score 4), and clinically poor (score 5) at baseline and after 6, 12, 18, and 24 months. In the studies carried out by de Souza et al. [12] and de Souza et al. [14], these variables were classified as follows: clinically very good (score 1), clinically good (score 2), clinically sufficient/satisfactory (score 3), clinically unsatisfactory (score 4), and clinically poor (score 5) at baseline and after 6 and 24 months.
In the studies performed by de Souza et al. [12] and de Souza et al. [14], the restorations were evaluated with the classical United States Public Health Service criteria (adapted by Dalton Bittencourt et al. [20] and Perdigão et al. [21]), in the same periods. Table 2 shows the main results of the selected articles.
Meta-analysis results
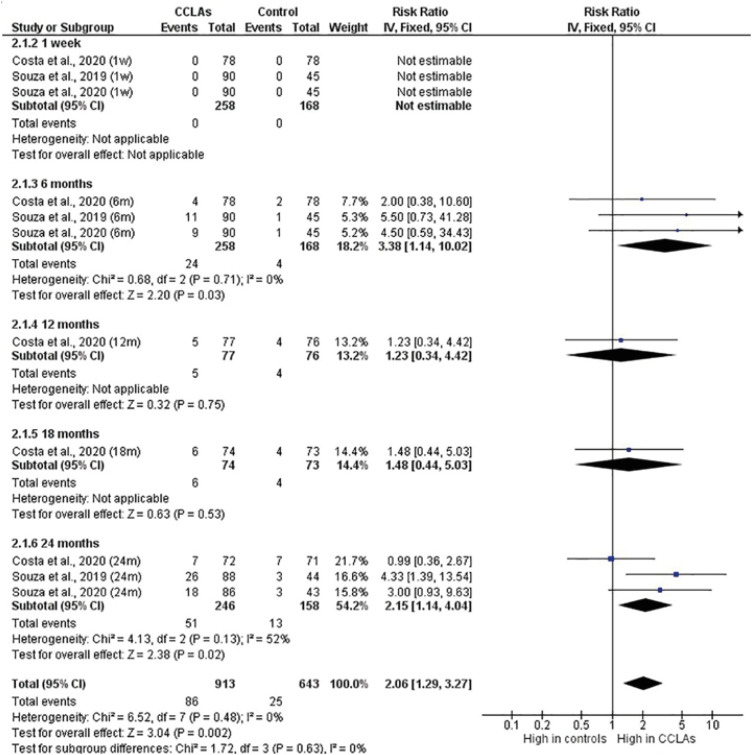
1. Retention
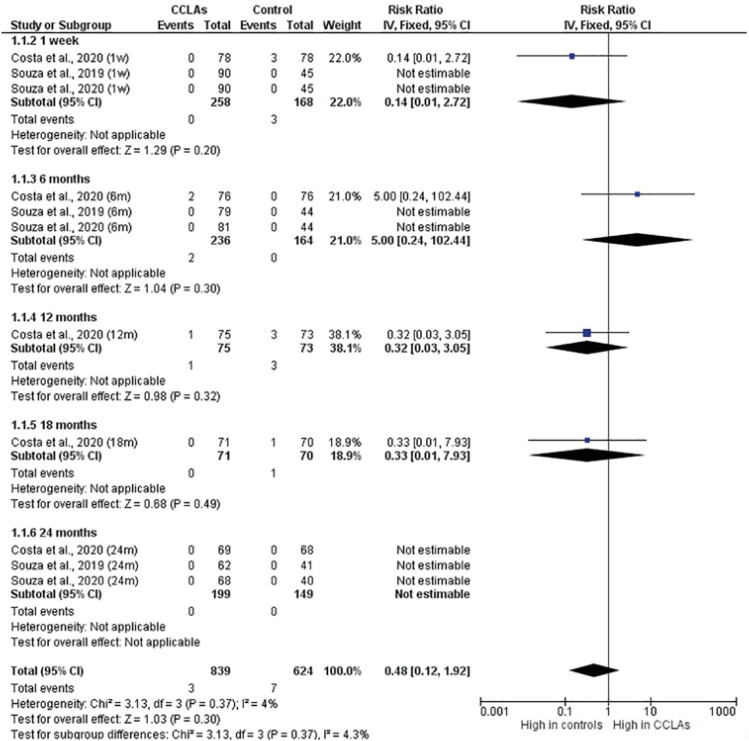
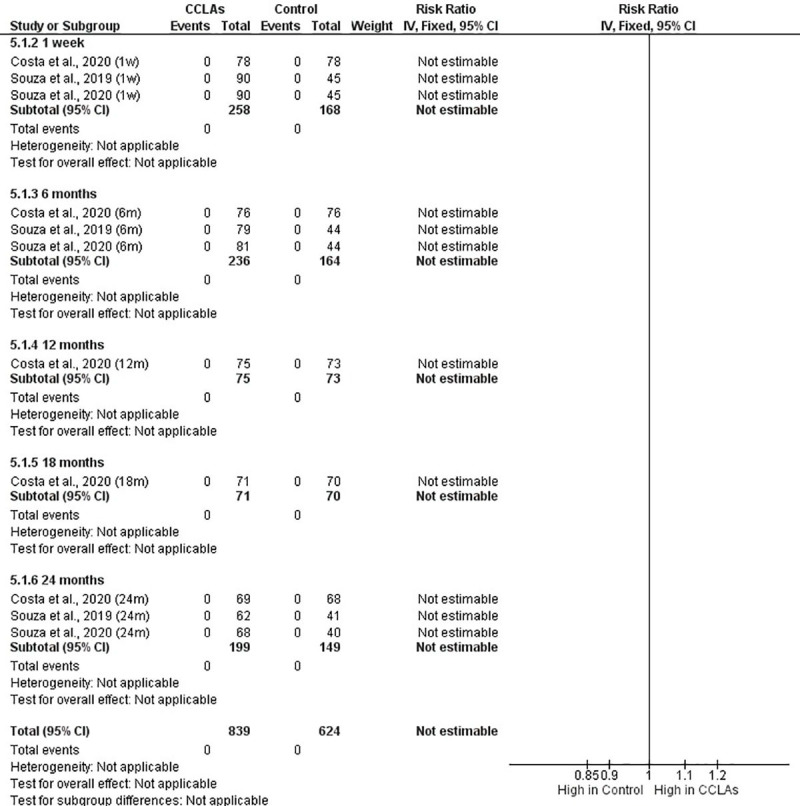
The scores for the retention of restorations showed there was a significant increase in the number of events in the CCLA group, with a relative risk of 2.06 (95% confidence interval [CI], 1.29–3.27) times greater in that group. There was no significant heterogeneity (p = 0.480, I2 = 0%) or differences between the subgroups (p = 0.630). In the first week of evaluation, there was no loss of retention (p = 1.000). After 6 months, the relative risk for loss of retention was 3.38 times higher (95% CI, 1.14–10.02) in the CCLA group (p = 0.030). After 12 and 18 months, only Costa et al. [13] had evaluations, which showed no increased risk, whereas after 24 months, there was a 2.15-fold increase (95% CI, 1.14–4.04) in the risk of loss of retention in the CCLA group (p = 0.020). In the leave-one-out analysis, the removal of de Souza et al. [12] (p = 0.120) and de Souza et al. [14] (p = 0.090) in the 6-month period diluted the increased risk of restoration loss. The removal of these 2 works in the 24-month period also diluted the increased risk of loss of restorations (p = 0.240 and p = 0.100), respectively (Figure 3).
2. Postoperative sensitivity
No significant difference was found in postoperative sensitivity between the CCLA and control groups (p = 0.300). There was no significant influence of the evaluated period (p = 0.370) or significant heterogeneity between the studies (p = 0.370, I2 = 4%). There were no significant differences between groups in any of the evaluated periods. The leave-one-out analysis showed no significant favoring of any individual study (Figure 4).
3. Marginal staining
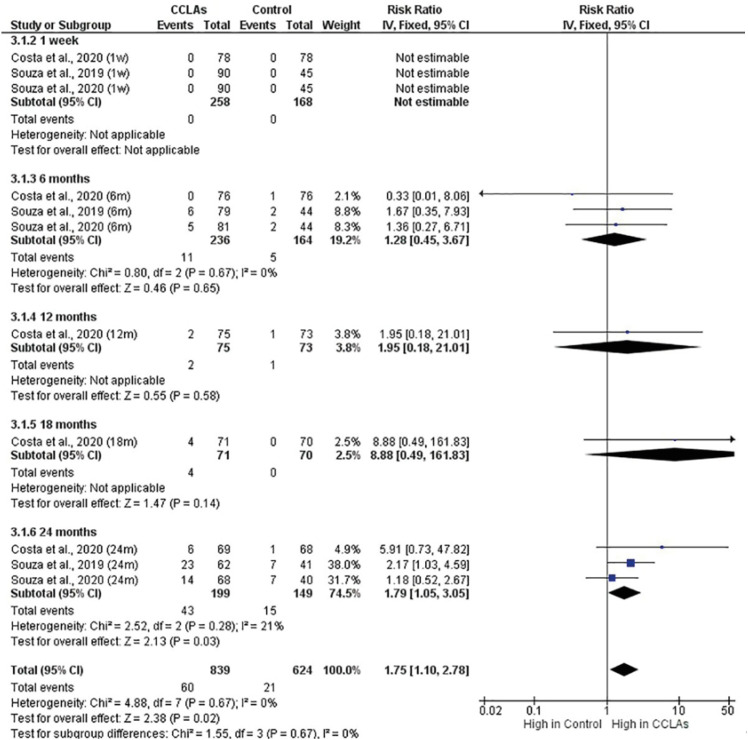
Pigmentation scores showed a significant increase in the CCLA group, with a relative risk of 1.75 (95% CI, 1.10–2.78) (p = 0.020). There were no significant differences between subgroups (p = 0.670) or significant heterogeneity between the studies (p = 0.670, I2 = 0%). There were no events in the first week (p = 1.000), nor a significant increase in the risk of pigmentation after 6 (p = 0.650), 12 (p = 0.580), or 18 (p = 0.140) months. After 24 months, the CCLA group showed a 1.79 times increase (95% CI, 1.05–3.05) in the risk of pigmentation (p = 0.030). The leave-one-out analysis showed no significant effects at the 6-month period, but significant effects were found at 24 months for the removal of Costa et al. [13] (p = 0.080) and de Souza et al. [12] (p = 0.330), but not de Souza et al. [14] (p = 0.010) (Figure 5).
4. Marginal adaptation
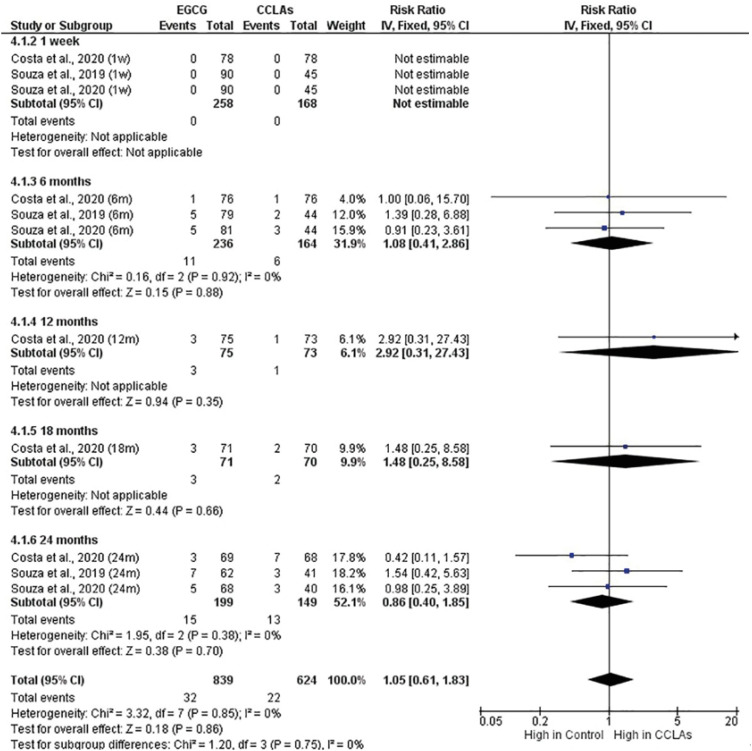
The adaptation failure scores showed no significant difference between the CCLA and control groups (p = 0.860). There were no differences between subgroups (p = 0.750), nor significant heterogeneity (p = 0.850, I2 = 0%). There were no events in the first week (p = 1.000), nor a significant increase in the risk of failure on marginal adaptation after 6 (p = 0.880), 12 (p = 0.350), 18 (p = 0.660), or 24 (p = 0.700) months. The leave-one-out analysis showed no significant favoring of any individual study (Figure 6).
5. Incidence of caries
There were no caries events in any group during the 24-month evaluation period (Appendix 1).
6. Additional analysis and confidence in cumulative evidence
According to the GRADE statements, which were based on certain aspects (e.g., RoB, inconsistency, and imprecision), certainty was estimated as high for all outcomes (retention of restorations, marginal staining, postoperative sensitivity, and marginal adaptation). Further explanations of evidence appraisal are available in Table 3.
Table 3
Grading of Recommendations, Assessment, Development and Evaluation (GRADE) evidence profile
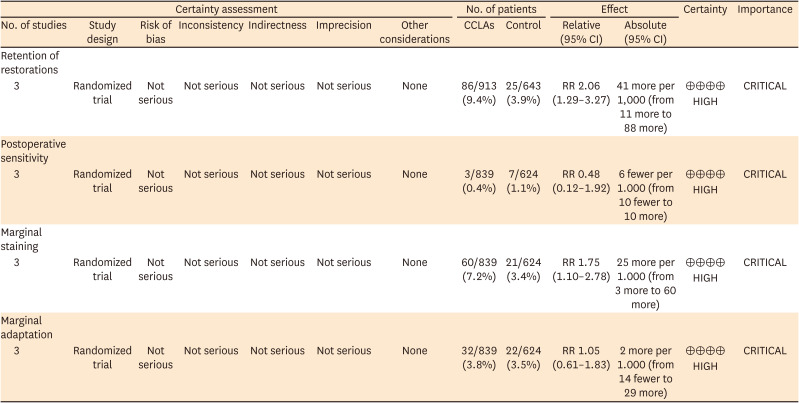
GRADE Working Group grades of evidence - High certainty: We are very confident that the true effect lies close to that of the estimate of the effect. Moderate certainty: We are moderately confident in the effect estimate. The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low certainty: Our confidence in the effect estimate is limited. The true effect may be substantially different from the estimate of the effect. Very low certainty: We have very little confidence in the effect estimate. The true effect is likely to be substantially different from the estimate of the effect.
CCLA, collagen cross-linking agent; CI, confidence interval; RR, risk ratio.
DISCUSSION
The achievement of a stable and lasting dentin-resin bonding interface is one of the main challenges of adhesive dentistry, and it has been the subject of several studies. One of the strategies to improve the quality of this interface is the use of CCLAs. Among these agents, glutaraldehyde, which is of synthetic origin, and EGCG and PACs, which are of natural origin, stand out [8222324].
The present systematic review compared the efficiency of procedures performed with the use of CCLAs, combined or not with the adhesive technique. Thus, the main objective of this investigation was to assess the effectiveness of CCLAs in combination with the adhesive technique in the performance of the restorative procedure. The articles included in this study have in common the use of CCLAs of natural origin. The studies performed by de Souza et al. [12] and de Souza et al. [14] used PACs from grape-seed extract as CCLAs, whereas the study conducted by Costa et al. [13] used EGCG from green tea. These substances contain polyphenols, which can interact with the collagen in dentin by forming multiple hydrogen bonds [25]. The meta-analysis showed no significant clinical benefit for the evaluated outcomes in the restorative procedures performed with the use of CCLAs when compared to those performed without the use of CCLAs.
The results obtained in the present meta-analysis showed that the addition of CCLAs had no significant clinical benefit on the retention of restorations. All studies included in this review reported that no additional mechanical preparation was performed, so the retention was based only on the adhesive system performance. It is worth mentioning that the presence of micromechanical retentions could positively interfere with this outcome. It is important to highlight that, 6 and 24 months after the use of CCLAs, there was a significant decrease in the quality of the retention of the restorations in the CCLA group. However, after 1 week, and at the 12- and 18-month time points evaluated only by Costa et al. [13], CCLA use showed no influence on retention. These findings raise the hypothesis that the studies conducted by de Souza et al. [12] and de Souza et al. [14] showed a major decrease in the retention of restorations in the CCLA group. However, the study of Costa et al. [13] supports the hypothesis of the clinical benefit caused by the addition of CCLAs to the adhesive technique. This investigation, unlike the others included in this meta-analysis, used EGCG, which is the major polyphenol present in green tea, as the CCLA; the effects of EGCG on reducing biodegradation and stabilizing collagen fibrils have already been demonstrated in laboratory studies [2627]. Furthermore, Du et al. [28] showed that, depending on the concentration, EGCG increased the immediate bond strength compared to the control group. In addition, Costa et al. [13] used the Single Bond Universal adhesive system (3M ESPE), which contains a functional monomer with a phosphate group, known as 10-methacryloyloxydecyl dihydrogen phosphate, that is able to bind to hydroxyapatite, providing a chemical adhesion mechanism [29]. A polyalkenoic acid copolymer is also present in the composition of this adhesive system, which has functional carboxylic groups capable of chemically interacting with hydroxyapatite [3031]. High retention rates with the use of this adhesive system have been previously demonstrated by other clinical trials [3132]. Therefore, the presence of these components may have improved the retention rate.
Marginal staining demonstrated that using CCLAs in combination with the adhesive technique had no significant clinical benefits within the evaluation periods used in the studies. After 1 week and 6, 12 and 18 months, the latter 2 time points evaluated only by Costa et al. [13], the use of these agents had no influence on marginal staining. After 24 months, the use of CCLAs increased the risk of pigmentation. The leave-one-out analysis showed that the removal of all studies within 6 months and the study of Costa et al. [13] and de Souza et al. [12] within 24 months did not change the outcomes. Conversely, the removal of the study of de Souza et al. [14] (within 24 months) demonstrated had a significant impact. The literature has described that dentin specimens treated with PAC agents presented a brownish color [33]. This pigmentation may be attributed to the oxidative properties of these compounds, the dark color of solutions, and the content of high-molecular-weight polymeric polyphenols [33343536]. The application mode seems to be associated with staining, once only the application as pretreatment resulted in increased pigmentation, as demonstrated by de Souza et al. [14].
The studies conducted by Costa et al. [13] and de Souza et al. [12] used CCLAs through the pretreatment approach. This technique has been the target of several laboratory studies [82427]. The time of application of CCLAs as a pretreatment is an important topic to be evaluated. Costa et al. [13] and de Souza et al. [12] carried out the application for 60 seconds, as well as Neri et al. [37] and Zheng and Chen [38], which showed in vitro that the application of EGCG and PAC, respectively, for that time was effective in preserving the resin-dentin bond durability. Although this application period is clinically feasible, it involves adding a step to the adhesive technique, thereby increasing the clinical time of the procedure, which goes against the trend of simplifying materials and restorative techniques [1213].
In order to simplify the use of CCLAs with the adhesive technique, several studies have investigated their incorporation into adhesive systems [282939404142]. Daood et al. [10] showed that the incorporation of 3% riboflavin in an adhesive improved the immediate bond strength and maintained the durability of the resin-dentin bond, without adversely affecting its degree of conversion. Another study showed that the degree of conversion of a commercial adhesive was not affected by the addition of 200 mg/mL EGCG [28]. In contrast, Epasinghe et al. [41] observed that up to 1% of grape seed extract can be incorporated into a dental adhesive resin without interfering with the mechanical properties or solubility of the resins. These adverse effects are associated with the antioxidant potential of CCLAs, which have free radicals that negatively interfere with the polymerization reaction of adhesives [3942]. During the polymerization process, PACs donate hydrogen radicals present in the phenolic groups, making it difficult to initiate and propagate the polymerization chain [39]. For EGCG, it was assumed that the interference in the polymerization reaction was due to its effect of scavenging free radicals [28].
There were no caries events in any group within 24 months of evaluation, and this result may be related to the multifactorial etiology of caries, the development of which requires the presence of specific microorganisms and frequent consumption of fermentable carbohydrates that facilitate their activity [43]. Furthermore, the studies used in this systematic review reported that, to be included in RCTs, all patients were required to have an acceptable or satisfactory standard of oral hygiene, which eliminates the RoB for this outcome.
When evaluating the GRADE, good levels of certainty were observed in the scientific evidence, in which the certainty was classified as high for all outcomes (Table 3). This certainty of scientific evidence is related to the quality of the selected articles, the study methodology (RCTs), and the number of restorative procedures performed. This result reflects a low RoB in the selected studies, which presented only a single criterion with a high RoB (blinding of participants and personnel). Due to the methodological design of the primary studies, the operator could not be blinded to the interventions performed, since the technique included the addition of an extra step in the application of the adhesive system or an adhesive system with changes in the commercial composition.
There are some other RCTs using other CCLAs; for instance, glutaraldehyde, a chemical compound of synthetic origin, has already demonstrated a potential biomodifying effect during in vitro studies, and it is one of the components of Gluma, a dental adhesive system available on the market [44]. Some RCTs have evaluated the performance of this adhesive system in restorative procedures; however, these works compared Gluma to other commercial adhesive systems with different formulations [4546474849]. Therefore, it would be impracticable to attribute effects to the use of this CCLA, without considering effects arising from the different compositions of the evaluated products. As previously mentioned, all articles included in this review compared the use or non-use of CCLA with the same adhesive system [1314].
The main methodological limitation of this systematic review is related to the small number of studies available in the literature and the short follow-up time, as well as the origin of the same country. Systematic reviews with meta-analysis are studies of great relevance to clinical practice, as they are able to summarize the best evidence with regard to clinical conduct and interventions [17]. Although few studies have been included in the present work, it followed all the steps of PRISMA and, according to GRADE, all papers presented a high certainty of the scientific evidence. Furthermore, this investigation shows a gap in the literature that can help guide new research in order to obtain more solid scientific evidence on the subject.
 XML Download
XML Download