

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Endodontic treatment aims to maintain periapical health or reduce the bacterial load in root canals to heal apical lesions by chemico-mechanical preparation of the root canal system, followed by hermetic obturation and coronal sealing [1]. However, failure may occur within the series of interdependent steps conducted in endodontic procedures, potentially affecting the final outcomes [2]. Several factors related to the peculiarities of each tooth may also affect whether root canal therapy has a successful prognosis [134], as well as the anatomical complexity of the root canal system [5]. Different degrees of root curvature may impair adequate instrumentation or hermetic filling, leading to the failure of endodontic treatment [6].
Non-surgical endodontic retreatment is generally the first treatment indicated for endodontically treated teeth presenting persistent apical periodontitis due to its efficacy and ability to preserve dental structures [7]. Some studies reported a success rate of 77% to 80% with retreatment [78], while another investigation reported an 84.1%–88.6% success rate after 4–10 years [9]. This procedure involves removing the filling material from the root canal and regaining access to the apical foramen [10], followed by further cleaning, shaping, and refilling to prevent re-infection [111].
The anatomical complexity of molar mesial canals may be a challenging factor for removing filling material due to the possible curvature and its position [12]. When accentuated, these curvatures may lead to complications during clinical procedures, compromising the safety and integrity of the instruments used for treatment [13]. A small angle and radius of root canal curvature are considered to be important factors that increase the tensional load on rotary nickel-titanium (NiTi) instruments and, consequently, the risk of operational accidents such as apical deviation, perforation, and instrument separation [1415]. Therefore, previous studies investigated different techniques for removing filling material from mesial canals of molars, suggesting a reduction in the working time and increased safety during endodontic retreatment when using NiTi systems [161718].
Root canal filling material can be removed using heated instruments, hand files, ultrasonic tips, and rotary or reciprocating file systems [192021222324]. The use of NiTi systems reduces the time required to clean and shape root canals and improves treatment safety [1011]. A new generation of rotary systems has shown flexibility, cutting efficiency, and more centered canal preparation due to improvements in the manufacturing process. Concomitantly, reciprocating single-file systems with increased flexibility have been produced, aiming to maintain the original canal curvature with minimal transportation, as well as to improve resistance to cyclic fatigue by reducing file contact with the canal walls [111825]. Furthermore, a filling removal technique using a reciprocating single-instrument with thermal treatment and an inactive tip, originally designed for root canal preparation, has been suggested as a technique safer filling material removal with simultaneous reinstrumentation compared to files designed only for retreatment procedures [12172627]. Nevertheless, inconsistent results have been reported regarding the safety and efficacy of rotary and reciprocating kinematics during filling material removal, especially in curved root canals [172428]. Although some studies have suggested that rotary motion enables superior filling material removal from curved canals [1228], other articles have reported enhanced efficiency with reciprocating motion [1729].
Thus, there is no consensus regarding the efficacy of different kinematics for the removal of filling material from curved root canals in non-surgical endodontic retreatment. This study conducted a systematic review of in vitro studies to compare the ability of rotary and reciprocating kinematics in removing root canal filling materials from curved root canals, in order to assist clinicians in determining which type of kinematics is more effective and safer.
MATERIALS AND METHODS
The present study was reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) checklist [3031]. This study was registered in the Open Science Framework (OSF) register (osf.io/wg7ba).
Eligibility criteria
The inclusion criterion was research on human teeth with curved root canals that compared the effects of rotary and reciprocating kinematics during the removal of root canal filling. The exclusion criteria were studies that assessed only the effects of rotary or reciprocating systems on filling material removal, and studies that compared rotary and reciprocating kinematics in removing filling material from non-curved root canals. Systematic reviews, case reports, animal studies, and editorial letters were also excluded.
The population, intervention, comparison, outcome (PICO) approach was used to address the following question: “Are rotary or reciprocating kinematics more effective or safe for filling material removal on curved root canal from extracted human permanent teeth?” In this process, the population was defined as curved root canals from extracted human permanent teeth that had been subjected to filling removal. The intervention was filling removal from curved root canals with rotary systems. The comparison was filling removal from curved root canals with reciprocating systems. The primary outcome evaluated was efficacy in removing filling material from curved root canals. The time required for filling removal, apical transportation, centering ability, instrument failure, debris extrusion, dentin removal, and NiTi alloy changes in preoperative and postoperative retreatment were considered as secondary outcomes.
Search strategy and information sources
Electronic searches were conducted in PubMed/MEDLINE, Scopus, and Cochrane Library until January 2021. The search strategy was as follows: (“root canal filling removal") OR ("gutta percha removal") OR ("root canal preparation") AND (“curved root canal”).
Manual searches of the reference lists of the included articles and in specific journals, such as the Journal of Endodontics, International Endodontic Journal, and Clinical Oral Investigations were also carried out.
Study selection
Studies were selected by 2 independent authors (L.P.S. and A.H.R.P.) in 2 steps. In step 1, the 2 authors assessed the titles/abstracts of the studies retrieved from the searches. Studies with titles and abstracts that met the eligibility criteria were included. In step 2, the 2 authors assessed the full texts. Studies in which the full text fulfilled the eligibility criteria were included. Any disagreements between the 2 authors were resolved through discussion, and when necessary, a third author (C.R.E.B.) was consulted.
Data collection and analyses
One author (L.P.S.) collected data from the included studies and tabulated them to analyze the results. The following data were retrieved: authors and year of publication, experimental model, root canal curvature, sample size, instrumentation protocol, root canal filling protocol, and filling removal protocol. Parameters related to data analysis, such as evaluation methods, and the main findings were also collected. The data were extracted from the included articles to evaluate the effectiveness and safety of the interventions. A second author (A.H.R.P.) checked the collected data. Each of the included studies was analyzed in terms of similarities so that a meta-analysis could be performed. However, after evaluation, considerable heterogeneity was found, contraindicating a meta-analysis.
Risk of bias
Two investigators (L.P.S. and A.H.R.P.) independently assessed the methodological quality of the selected studies according to their levels of evidence, following a modified version of the Joanna Briggs Institute (JBI) Critical Appraisal Checklist for Experimental Studies [313233]. The items included in the checklist were a clearly stated aim, justification of the sample size, sample randomization, blind treatment allocation, possibility of comparison between controls and treatment groups, baseline equivalence of control and treatment groups, clear root canal preparation protocol, clear root canal filling protocol, clear root canal filling removal protocol, measurement method, measurement standardization, and adequate statistical analysis. Each item was scored using a 2-point scale: 0, not reported or reported inadequately; 1, reported and adequate. Doubts and discrepancies between both investigators were discussed to achieve a consensus, and if a consensus was not reached, a third examiner (C.A.A.L.) was consulted.
RESULTS
Selected studies
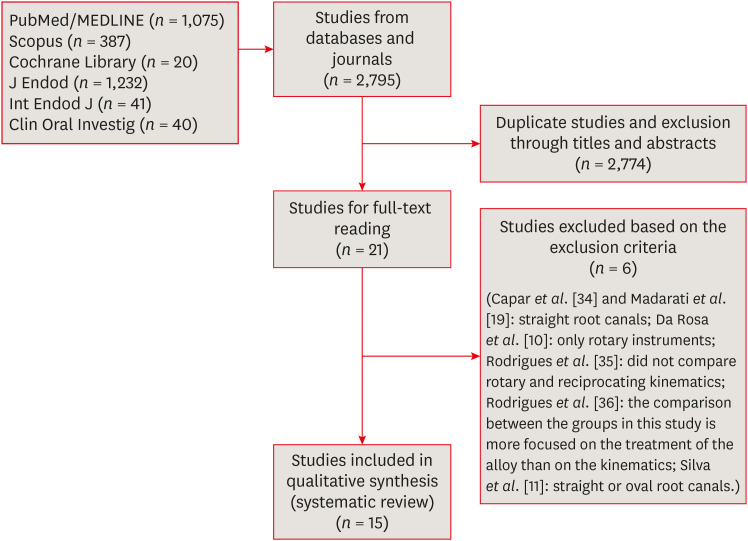
The selection process of the articles is presented in Figure 1. A total of 2,795 articles were found by database searches. After the first screening, 21 studies were selected. These studies were then subjected to a full-text evaluation that resulted in the exclusion of 6 studies [101119343536]. The reasons for the exclusion of these articles are shown in Figure 1. Lastly, 15 studies met the inclusion criteria [121617182428293738394041424344].
Figure 1
Flow diagram of the search strategy of the systematic review following the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines.
The assessed Cohen kappa coefficient value for inter-investigator agreement was 0.959 for PubMed, 1.000 for Scopus, 1.000 for the Cochrane Library, 0.888 for the Journal of Endodontics, 1.000 for the International Endodontic Journal, and 1.000 for Clinical Oral Investigations. These values indicated almost perfect agreement among reviewers according to the scale of Landis and Koch [45].
Characteristics of the included studies
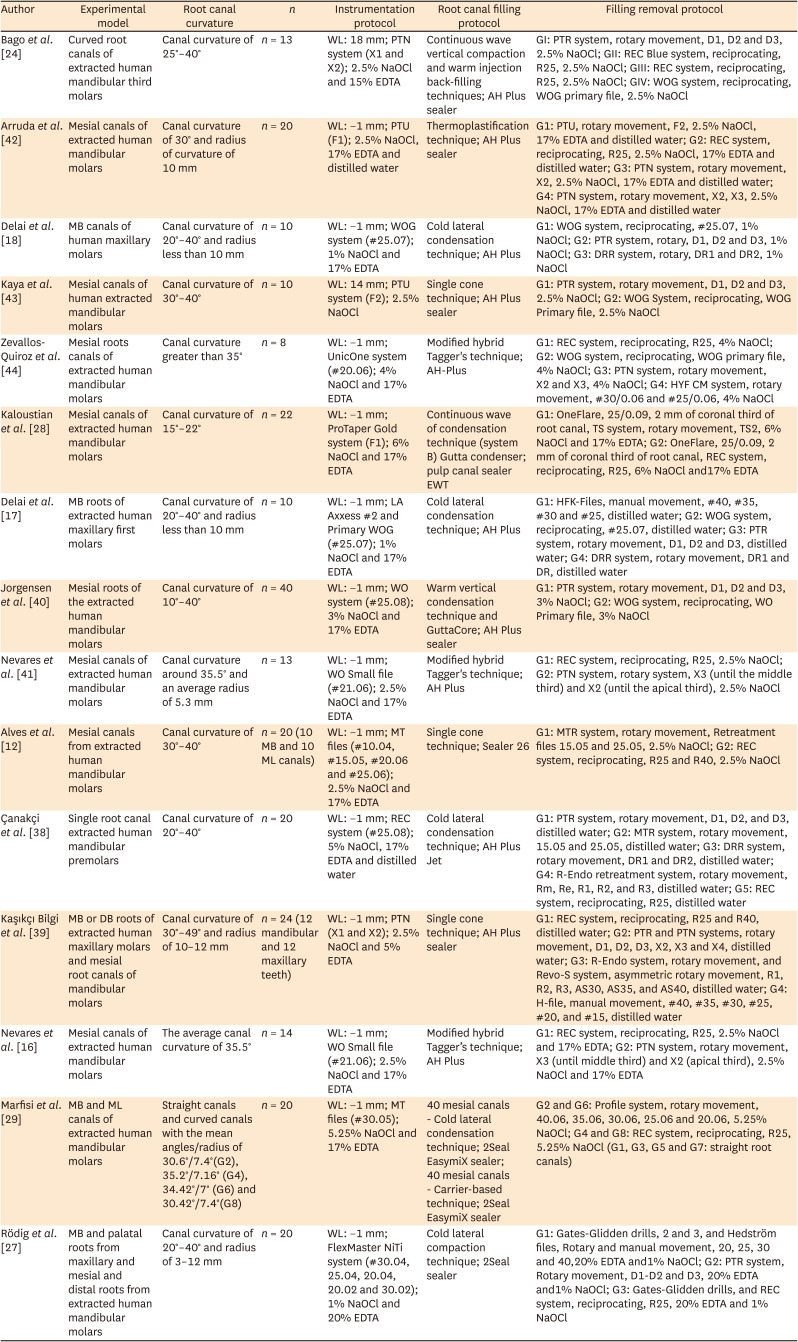
The characteristics of the studies are presented in Table 1.
Table 1
Characteristics of the included studies
| Author | Experimental model | Root canal curvature | n | Instrumentation protocol | Root canal filling protocol | Filling removal protocol |
|---|---|---|---|---|---|---|
| Bago et al. [24] | Curved root canals of extracted human mandibular third molars | Canal curvature of 25°–40° | n = 13 | WL: 18 mm; PTN system (X1 and X2); 2.5% NaOCl and 15% EDTA | Continuous wave vertical compaction and warm injection back-filling techniques; AH Plus sealer | GI: PTR system, rotary movement, D1, D2 and D3, 2.5% NaOCl; GII: REC Blue system, reciprocating, R25, 2.5% NaOCl; GIII: REC system, reciprocating, R25, 2.5% NaOCl; GIV: WOG system, reciprocating, WOG primary file, 2.5% NaOCl |
| Arruda et al. [42] | Mesial canals of extracted human mandibular molars | Canal curvature of 30° and radius of curvature of 10 mm | n = 20 | WL: −1 mm; PTU (F1); 2.5% NaOCl, 17% EDTA and distilled water | Thermoplastification technique; AH Plus sealer | G1: PTU, rotary movement, F2, 2.5% NaOCl, 17% EDTA and distilled water; G2: REC system, reciprocating, R25, 2.5% NaOCl, 17% EDTA and distilled water; G3: PTN system, rotary movement, X2, 2.5% NaOCl, 17% EDTA and distilled water; G4: PTN system, rotary movement, X2, X3, 2.5% NaOCl, 17% EDTA and distilled water |
| Delai et al. [18] | MB canals of human maxillary molars | Canal curvature of 20°–40° and radius less than 10 mm | n = 10 | WL: −1 mm; WOG system (#25.07); 1% NaOCl and 17% EDTA | Cold lateral condensation technique; AH Plus | G1: WOG system, reciprocating, #25.07, 1% NaOCl; G2: PTR system, rotary, D1, D2 and D3, 1% NaOCl; G3: DRR system, rotary, DR1 and DR2, 1% NaOCl |
| Kaya et al. [43] | Mesial canals of human extracted mandibular molars | Canal curvature of 30°–40° | n = 10 | WL: 14 mm; PTU system (F2); 2.5% NaOCl | Single cone technique; AH Plus sealer | G1: PTR system, rotary movement, D1, D2 and D3, 2.5% NaOCl; G2: WOG System, reciprocating, WOG Primary file, 2.5% NaOCl |
| Zevallos-Quiroz et al. [44] | Mesial roots canals of extracted human mandibular molars | Canal curvature greater than 35° | n = 8 | WL: −1 mm; UnicOne system (#20.06); 4% NaOCl and 17% EDTA | Modified hybrid Tagger's technique; AH-Plus | G1: REC system, reciprocating, R25, 4% NaOCl; G2: WOG system, reciprocating, WOG primary file, 4% NaOCl; G3: PTN system, rotary movement, X2 and X3, 4% NaOCl; G4: HYF CM system, rotary movement, #30/0.06 and #25/0.06, 4% NaOCl |
| Kaloustian et al. [28] | Mesial canals of extracted human mandibular molars | Canal curvature of 15°–22° | n = 22 | WL: −1 mm; ProTaper Gold system (F1); 6% NaOCl and 17% EDTA | Continuous wave of condensation technique (system B) Gutta condenser; pulp canal sealer EWT | G1: OneFlare, 25/0.09, 2 mm of coronal third of root canal, TS system, rotary movement, TS2, 6% NaOCl and 17% EDTA; G2: OneFlare, 25/0.09, 2 mm of coronal third of root canal, REC system, reciprocating, R25, 6% NaOCl and17% EDTA |
| Delai et al. [17] | MB roots of extracted human maxillary first molars | Canal curvature of 20°–40° and radius less than 10 mm | n = 10 | WL: −1 mm; LA Axxess #2 and Primary WOG (#25.07); 1% NaOCl and 17% EDTA | Cold lateral condensation technique; AH Plus | G1: HFK-Files, manual movement, #40, #35, #30 and #25, distilled water; G2: WOG system, reciprocating, #25.07, distilled water; G3: PTR system, rotary movement, D1, D2 and D3, distilled water; G4: DRR system, rotary movement, DR1 and DR, distilled water |
| Jorgensen et al. [40] | Mesial roots of the extracted human mandibular molars | Canal curvature of 10°–40° | n = 40 | WL: −1 mm; WO system (#25.08); 3% NaOCl and 17% EDTA | Warm vertical condensation technique and GuttaCore; AH Plus sealer | G1: PTR system, rotary movement, D1, D2 and D3, 3% NaOCl; G2: WOG system, reciprocating, WO Primary file, 3% NaOCl |
| Nevares et al. [41] | Mesial canals of extracted human mandibular molars | Canal curvature around 35.5° and an average radius of 5.3 mm | n = 13 | WL: −1 mm; WO Small file (#21.06); 2.5% NaOCl and 17% EDTA | Modified hybrid Tagger's technique; AH Plus | G1: REC system, reciprocating, R25, 2.5% NaOCl; G2: PTN system, rotary system, X3 (until the middle third) and X2 (until the apical third), 2.5% NaOCl |
| Alves et al. [12] | Mesial canals from extracted human mandibular molars | Canal curvature of 30°–40° | n = 20 (10 MB and 10 ML canals) | WL: −1 mm; MT files (#10.04, #15.05, #20.06 and #25.06); 2.5% NaOCl and 17% EDTA | Single cone technique; Sealer 26 | G1: MTR system, rotary movement, Retreatment files 15.05 and 25.05, 2.5% NaOCl; G2: REC system, reciprocating, R25 and R40, 2.5% NaOCl |
| Çanakçi et al. [38] | Single root canal extracted human mandibular premolars | Canal curvature of 20°–40° | n = 20 | WL: −1 mm; REC system (#25.08); 5% NaOCl, 17% EDTA and distilled water | Cold lateral condensation technique; AH Plus Jet | G1: PTR system, rotary movement, D1, D2, and D3, distilled water; G2: MTR system, rotary movement, 15.05 and 25.05, distilled water; G3: DRR system, rotary movement, DR1 and DR2, distilled water; G4: R-Endo retreatment system, rotary movement, Rm, Re, R1, R2, and R3, distilled water; G5: REC system, reciprocating, R25, distilled water |
| Kaşıkçı Bilgi et al. [39] | MB or DB roots of extracted human maxillary molars and mesial root canals of mandibular molars | Canal curvature of 30°–49° and radius of 10–12 mm | n = 24 (12 mandibular and 12 maxillary teeth) | WL: −1 mm; PTN (X1 and X2); 2.5% NaOCl and 5% EDTA | Single cone technique; AH Plus sealer | G1: REC system, reciprocating, R25 and R40, distilled water; G2: PTR and PTN systems, rotary movement, D1, D2, D3, X2, X3 and X4, distilled water; G3: R-Endo system, rotary movement, and Revo-S system, asymmetric rotary movement, R1, R2, R3, AS30, AS35, and AS40, distilled water; G4: H-file, manual movement, #40, #35, #30, #25, #20, and #15, distilled water |
| Nevares et al. [16] | Mesial canals of extracted human mandibular molars | The average canal curvature of 35.5° | n = 14 | WL: −1 mm; WO Small file (#21.06); 2.5% NaOCl and 17% EDTA | Modified hybrid Tagger’s technique; AH Plus | G1: REC system, reciprocating, R25, 2.5% NaOCl and 17% EDTA; G2: PTN system, rotary movement, X3 (until middle third) and X2 (apical third), 2.5% NaOCl and 17% EDTA |
| Marfisi et al. [29] | MB and ML canals of extracted human mandibular molars | Straight canals and curved canals with the mean angles/radius of 30.6°/7.4°(G2), 35.2°/7.16° (G4), 34.42°/7° (G6) and 30.42°/7.4°(G8) | n = 20 | WL: −1 mm; MT files (#30.05); 5.25% NaOCl and 17% EDTA | 40 mesial canals - Cold lateral condensation technique; 2Seal EasymiX sealer; 40 mesial canals - Carrier-based technique; 2Seal EasymiX sealer | G2 and G6: Profile system, rotary movement, 40.06, 35.06, 30.06, 25.06 and 20.06, 5.25% NaOCl; G4 and G8: REC system, reciprocating, R25, 5.25% NaOCl (G1, G3, G5 and G7: straight root canals) |
| Rödig et al. [27] | MB and palatal roots from maxillary and mesial and distal roots from extracted human mandibular molars | Canal curvature of 20°–40° and radius of 3–12 mm | n = 20 | WL: −1 mm; FlexMaster NiTi system (#30.04, 25.04, 20.04, 20.02 and 30.02); 1% NaOCl and 20% EDTA | Cold lateral compaction technique; 2Seal sealer | G1: Gates-Glidden drills, 2 and 3, and Hedström files, Rotary and manual movement, 20, 25, 30 and 40,20% EDTA and1% NaOCl; G2: PTR system, Rotary movement, D1-D2 and D3, 20% EDTA and1% NaOCl; G3: Gates-Glidden drills, and REC system, reciprocating, R25, 20% EDTA and 1% NaOCl |
WL, working length; PTN, ProTaper Next; NaOCl, sodium hypochlorite; EDTA, ethylenediaminetetraacetic acid; G, group; PTR, ProTaper Universal Retreatment; REC, Reciproc; WOG, WaveOne Gold; PTU, ProTaper Universal; WO, WaveOne; DRR, D-RaCe Retreatment; HYF, Hyflex; CM, controlled memory; TS, T-Wire system; MTR, Mtwo Retreatment; HF, hand files; MT, Mtwo; DB, distobuccal; ML, mesiolingual; MB, mesiobuccal.
1. Types of teeth and root canal preparation
Eleven studies were performed on mesial root canals of mandibular molars [1216282937394041424344], 2 on distal roots of mandibular molars [3739], 1 on root canals of third mandibular molars [24], 1 on single root canal teeth [38], 2 on mesiobuccal canals of maxillary molars [1718], and 1 on the mesiobuccal and palatal roots of maxillary molars [37].
Most of the studies reported the use of root canals with curvature between 30º and 40º [1216293941424344]. Only 1 study analyzed both straight and curved canals [29]; however, only the procedures conducted for curved root canals were considered. Standardized root canal curvatures were mostly used in each study.
Rotary kinematics were employed for the primary mechanical preparation of root canals in most studies, using ProTaper Next [2439], Protaper Universal [4243], ProTaper Gold [28], and Mtwo [1229] systems. In other studies, reciprocating kinematics were performed using WaveOne [161841], WaveOne Gold [1740], Reciproc [38], and other systems. A working length of 1 mm from the apex was established in most studies [121617182829373839404144].
2. Root canal filling and filling removal protocols
For obturation, lateral condensation [1718293738], thermoplasticized [1624282940414244], and single cone [123943] techniques were used. Regarding the types of materials, 11 eligible studies used AH Plus sealer combined with gutta-percha points [161718
24383941424344] or GuttaCore [40]. The remaining studies used combination of gutta-percha points with the EWT pulp canal sealer, Sealer 26, or 2Seal sealer [12272829].
Filling removal was performed using rotary kinematics with the ProTaper Universal retreatment system [17182437383943], ProTaper Next [16414244], Mtwo retreatment [1238], D-Race system [171838], ProTaper Universal [42], and others. Regarding the reciprocating motion, the filling materials were mainly removed using Reciproc [1216242829373839414244] and WaveOne Gold [1718404344]. No studies described using organic solvents.
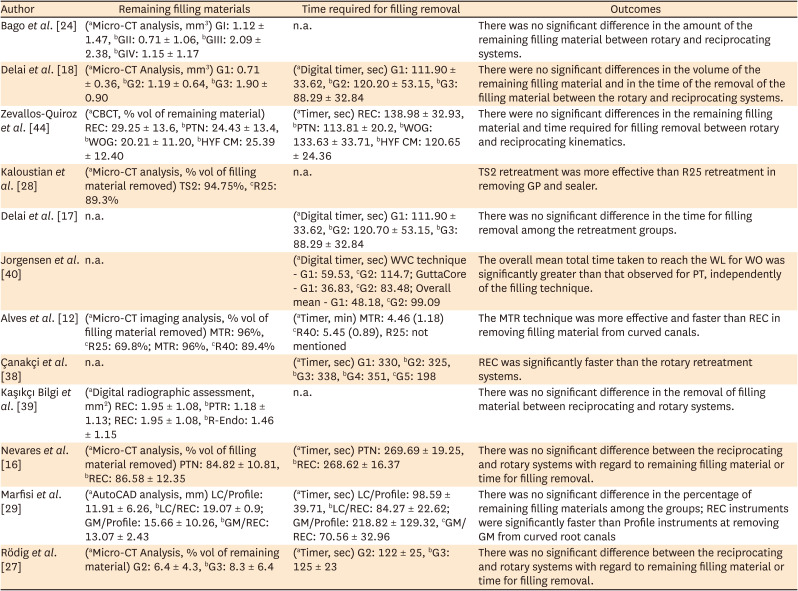
Table 2 summarizes the results related to the efficiency of both kinematics for removing the filling material in terms of the remaining filling material and the time required for filling removal. Table 3 describes the results related to safety during filling material removal, including apical transportation, centering ability, instrument fracture, dentin removal, debris extrusion, NiTi composition in preoperative and postoperative retreatment, and roughness of the instruments.
Table 2
Efficacy during root canal filling removal between rotary and reciprocating kinematics
| Author | Remaining filling materials | Time required for filling removal | Outcomes |
|---|---|---|---|
| Bago et al. [24] | (aMicro-CT analysis, mm3) GI: 1.12 ± 1.47, bGII: 0.71 ± 1.06, bGIII: 2.09 ± 2.38, bGIV: 1.15 ± 1.17 | n.a. | There was no significant difference in the amount of the remaining filling material between rotary and reciprocating systems. |
| Delai et al. [18] | (aMicro-CT Analysis, mm3) G1: 0.71 ± 0.36, bG2: 1.19 ± 0.64, bG3: 1.90 ± 0.90 | (aDigital timer, sec) G1: 111.90 ± 33.62, bG2: 120.20 ± 53.15, bG3: 88.29 ± 32.84 | There were no significant differences in the volume of the remaining filling material and in the time of the removal of the filling material between the rotary and reciprocating systems. |
| Zevallos-Quiroz et al. [44] | (aCBCT, % vol of remaining material) REC: 29.25 ± 13.6, bPTN: 24.43 ± 13.4, bWOG: 20.21 ± 11.20, bHYF CM: 25.39 ± 12.40 | (aTimer, sec) REC: 138.98 ± 32.93, bPTN: 113.81 ± 20.2, bWOG: 133.63 ± 33.71, bHYF CM: 120.65 ± 24.36 | There were no significant differences in the remaining filling material and time required for filling removal between rotary and reciprocating kinematics. |
| Kaloustian et al. [28] | (aMicro-CT analysis, % vol of filling material removed) TS2: 94.75%, cR25: 89.3% | n.a. | TS2 retreatment was more effective than R25 retreatment in removing GP and sealer. |
| Delai et al. [17] | n.a. | (aDigital timer, sec) G1: 111.90 ± 33.62, bG2: 120.70 ± 53.15, bG3: 88.29 ± 32.84 | There was no significant difference in the time for filling removal among the retreatment groups. |
| Jorgensen et al. [40] | n.a. | (aDigital timer, sec) WVC technique - G1: 59.53, cG2: 114.7; GuttaCore - G1: 36.83, cG2: 83.48; Overall mean - G1: 48.18, cG2: 99.09 | The overall mean total time taken to reach the WL for WO was significantly greater than that observed for PT, independently of the filling technique. |
| Alves et al. [12] | (aMicro-CT imaging analysis, % vol of filling material removed) MTR: 96%, cR25: 69.8%; MTR: 96%, cR40: 89.4% | (aTimer, min) MTR: 4.46 (1.18) cR40: 5.45 (0.89), R25: not mentioned | The MTR technique was more effective and faster than REC in removing filling material from curved canals. |
| Çanakçi et al. [38] | n.a. | (aTimer, sec) G1: 330, bG2: 325, bG3: 338, bG4: 351, cG5: 198 | REC was significantly faster than the rotary retreatment systems. |
| Kaşıkçı Bilgi et al. [39] | (aDigital radiographic assessment, mm2) REC: 1.95 ± 1.08, bPTR: 1.18 ± 1.13; REC: 1.95 ± 1.08, bR-Endo: 1.46 ± 1.15 | n.a. | There was no significant difference in the removal of filling material between reciprocating and rotary systems. |
| Nevares et al. [16] | (aMicro-CT analysis, % vol of filling material removed) PTN: 84.82 ± 10.81, bREC: 86.58 ± 12.35 | (aTimer, sec) PTN: 269.69 ± 19.25, bREC: 268.62 ± 16.37 | There was no significant difference between the reciprocating and rotary systems with regard to remaining filling material or time for filling removal. |
| Marfisi et al. [29] | (aAutoCAD analysis, mm) LC/Profile: 11.91 ± 6.26, bLC/REC: 19.07 ± 0.9; GM/Profile: 15.66 ± 10.26, bGM/REC: 13.07 ± 2.43 | (aTimer, sec) LC/Profile: 98.59 ± 39.71, bLC/REC: 84.27 ± 22.62; GM/Profile: 218.82 ± 129.32, cGM/REC: 70.56 ± 32.96 | There was no significant difference in the percentage of remaining filling materials among the groups; REC instruments were significantly faster than Profile instruments at removing GM from curved root canals |
| Rödig et al. [27] | (aMicro-CT Analysis, % vol of remaining material) G2: 6.4 ± 4.3, bG3: 8.3 ± 6.4 | (aTimer, sec) G2: 122 ± 25, bG3: 125 ± 23 | There was no significant difference between the reciprocating and rotary systems with regard to remaining filling material or time for filling removal. |
G: group, n.a.: not applicable, WT: working time, sec: seconds, CBCT: Cone Beam computed Tomography, vol: volume, REC: Reciproc, PTN: ProTaper Next instrument, WOG: WaveOne Gold, HYF: Hyflex, TS2: 2Shape #2, GP: gutta-percha, MTR: Mtwo-Retreatment, PTR: ProTaper Universal Retreatment, WO: WaveOne, DRR: D-RaCe Retreatment, WVC: warm vertical condensation, PT: ProTaper, MT: Mtwo, LC: lateral condensation, GM: Gutta Master.
The symbol a indicates that a test was applied; b indicates no significant differences between groups; c indicates significant differences between groups.
Table 3
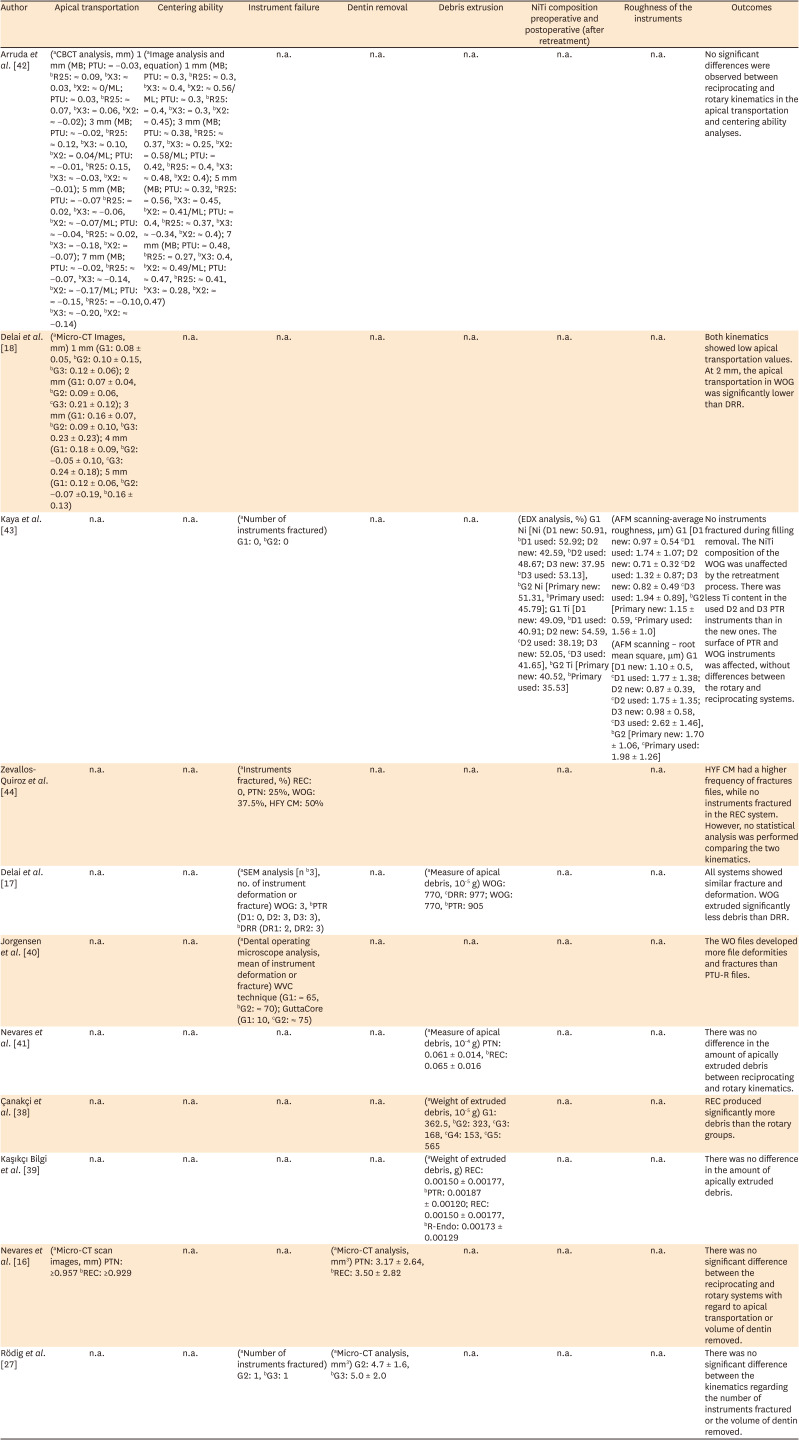
Safety during root canal filling removal between rotary and reciprocating kinematics
| Author | Apical transportation | Centering ability | Instrument failure | Dentin removal | Debris extrusion | NiTi composition preoperative and postoperative (after retreatment) | Roughness of the instruments | Outcomes |
|---|---|---|---|---|---|---|---|---|
| Arruda et al. [42] | (aCBCT analysis, mm) 1 mm (MB; PTU: ≈ −0.03, bR25: ≈ 0.09, bX3: ≈ 0.03, bX2: ≈ 0/ML; PTU: ≈ 0.03, bR25: ≈ 0.07, bX3: ≈ 0.06, bX2: ≈ −0.02); 3 mm (MB; PTU: ≈ −0.02, bR25: ≈ 0.12, bX3: ≈ 0.10, bX2: ≈ 0.04/ML; PTU: ≈ −0.01, bR25: 0.15, bX3: ≈ −0.03, bX2: ≈ −0.01); 5 mm (MB; PTU: ≈ −0.07 bR25: ≈ 0.02, bX3: ≈ −0.06, bX2: ≈ −0.07/ML; PTU: ≈ −0.04, bR25: ≈ 0.02, bX3: ≈ −0.18, bX2: ≈ −0.07); 7 mm (MB; PTU: ≈ −0.02, bR25: ≈ −0.07, bX3: ≈ −0.14, bX2: ≈ −0.17/ML; PTU: ≈ −0.15, bR25: ≈ −0.10, bX3: ≈ −0.20, bX2: ≈ −0.14) | (aImage analysis and equation) 1 mm (MB; PTU: ≈ 0.3, bR25: ≈ 0.3, bX3: ≈ 0.4, bX2: ≈ 0.56/ML; PTU: ≈ 0.3, bR25: ≈ 0.4, bX3: ≈ 0.3, bX2: ≈ 0.45); 3 mm (MB; PTU: ≈ 0.38, bR25: ≈ 0.37, bX3: ≈ 0.25, bX2: ≈ 0.58/ML; PTU: ≈ 0.42, bR25: ≈ 0.4, bX3: ≈ 0.48, bX2: 0.4); 5 mm (MB; PTU: ≈ 0.32, bR25: ≈ 0.56, bX3: ≈ 0.45, bX2: ≈ 0.41/ML; PTU: ≈ 0.4, bR25: ≈ 0.37, bX3: ≈ −0.34, bX2: ≈ 0.4); 7 mm (MB; PTU: ≈ 0.48, bR25: ≈ 0.27, bX3: 0.4, bX2: ≈ 0.49/ML; PTU: ≈ 0.47, bR25: ≈ 0.41, bX3: ≈ 0.28, bX2: ≈ 0.47) | n.a. | n.a. | n.a. | n.a. | n.a. | No significant differences were observed between reciprocating and rotary kinematics in the apical transportation and centering ability analyses. |
| Delai et al. [18] | (aMicro-CT Images, mm) 1 mm (G1: 0.08 ± 0.05, bG2: 0.10 ± 0.15, bG3: 0.12 ± 0.06); 2 mm (G1: 0.07 ± 0.04, bG2: 0.09 ± 0.06, cG3: 0.21 ± 0.12); 3 mm (G1: 0.16 ± 0.07, bG2: 0.09 ± 0.10, bG3: 0.23 ± 0.23); 4 mm (G1: 0.18 ± 0.09, bG2: −0.05 ± 0.10, cG3: 0.24 ± 0.18); 5 mm (G1: 0.12 ± 0.06, bG2: −0.07 ±0.19, b0.16 ± 0.13) | n.a. | n.a. | n.a. | n.a. | n.a. | n.a. | Both kinematics showed low apical transportation values. At 2 mm, the apical transportation in WOG was significantly lower than DRR. |
| Kaya et al. [43] | n.a. | n.a. | (aNumber of instruments fractured) G1: 0, bG2: 0 | n.a. | n.a. | (EDX analysis, %) G1 Ni [Ni (D1 new: 50.91, bD1 used: 52.92; D2 new: 42.59, bD2 used: 48.67; D3 new: 37.95 bD3 used: 53.13], bG2 Ni [Primary new: 51.31, bPrimary used: 45.79]; G1 Ti [D1 new: 49.09, bD1 used: 40.91; D2 new: 54.59, cD2 used: 38.19; D3 new: 52.05, cD3 used: 41.65], bG2 Ti [Primary new: 40.52, bPrimary used: 35.53] | (AFM scanning-average roughness, μm) G1 [D1 new: 0.97 ± 0.54 cD1 used: 1.74 ± 1.07; D2 new: 0.71 ± 0.32 cD2 used: 1.32 ± 0.87; D3 new: 0.82 ± 0.49 cD3 used: 1.94 ± 0.89], bG2 [Primary new: 1.15 ± 0.59, cPrimary used: 1.56 ± 1.0] | No instruments fractured during filling removal. The NiTi composition of the WOG was unaffected by the retreatment process. There was less Ti content in the used D2 and D3 PTR instruments than in the new ones. The surface of PTR and WOG instruments was affected, without differences between the rotary and reciprocating systems. |
| (AFM scanning – root mean square, μm) G1 [D1 new: 1.10 ± 0.5, cD1 used: 1.77 ± 1.38; D2 new: 0.87 ± 0.39, cD2 used: 1.75 ± 1.35; D3 new: 0.98 ± 0.58, cD3 used: 2.62 ± 1.46], bG2 [Primary new: 1.70 ± 1.06, cPrimary used: 1.98 ± 1.26] | ||||||||
| Zevallos-Quiroz et al. [44] | n.a. | n.a. | (aInstruments fractured, %) REC: 0, PTN: 25%, WOG: 37.5%, HFY CM: 50% | n.a. | n.a. | n.a. | n.a. | HYF CM had a higher frequency of fractures files, while no instruments fractured in the REC system. However, no statistical analysis was performed comparing the two kinematics. |
| Delai et al. [17] | n.a. | n.a. | (aSEM analysis [n b3], no. of instrument deformation or fracture) WOG: 3, bPTR (D1: 0, D2: 3, D3: 3), bDRR (DR1: 2, DR2: 3) | n.a. | (aMeasure of apical debris, 10-5 g) WOG: 770, cDRR: 977; WOG: 770, bPTR: 905 | n.a. | n.a. | All systems showed similar fracture and deformation. WOG extruded significantly less debris than DRR. |
| Jorgensen et al. [40] | n.a. | n.a. | (aDental operating microscope analysis, mean of instrument deformation or fracture) WVC technique (G1: ≈ 65, bG2: ≈ 70); GuttaCore (G1: 10, cG2: ≈ 75) | n.a. | n.a. | n.a. | n.a. | The WO files developed more file deformities and fractures than PTU-R files. |
| Nevares et al. [41] | n.a. | n.a. | n.a. | n.a. | (aMeasure of apical debris, 10-4 g) PTN: 0.061 ± 0.014, bREC: 0.065 ± 0.016 | n.a. | n.a. | There was no difference in the amount of apically extruded debris between reciprocating and rotary kinematics. |
| Çanakçi et al. [38] | n.a. | n.a. | n.a. | n.a. | (aWeight of extruded debris, 10-5 g) G1: 362.5, bG2: 323, cG3: 168, cG4: 153, cG5: 565 | n.a. | n.a. | REC produced significantly more debris than the rotary groups. |
| Kaşıkçı Bilgi et al. [39] | n.a. | n.a. | n.a. | n.a. | (aWeight of extruded debris, g) REC: 0.00150 ± 0.00177, bPTR: 0.00187 ± 0.00120; REC: 0.00150 ± 0.00177, bR-Endo: 0.00173 ± 0.00129 | n.a. | n.a. | There was no difference in the amount of apically extruded debris. |
| Nevares et al. [16] | (aMicro-CT scan images, mm) PTN: ≥0.957 bREC: ≥0.929 | n.a. | n.a. | (aMicro-CT analysis, mm3) PTN: 3.17 ± 2.64, bREC: 3.50 ± 2.82 | n.a. | n.a. | n.a. | There was no significant difference between the reciprocating and rotary systems with regard to apical transportation or volume of dentin removed. |
| Rödig et al. [27] | n.a. | n.a. | (aNumber of instruments fractured) G2: 1, bG3: 1 | (aMicro-CT analysis, mm3) G2: 4.7 ± 1.6, bG3: 5.0 ± 2.0 | n.a. | n.a. | n.a. | There was no significant difference between the kinematics regarding the number of instruments fractured or the volume of dentin removed. |
n.a., not applicable; CBCT, Cone Beam Computed Tomography; mm, millimeters; mm3, cubic millimeters; MB, mesiobuccal root canal; ML, mesiolingual root canal; PTU, ProTaper Universal; CT, computed tomography; G, group; EDX = energy dispersive X-ray spectrophotometry; Ni, Nickel; Ti, Titanium; AFM, atomic force microscopy; WOG, WaveOne Gold; PTR, ProTaper Universal Retreatment; REC, Reciproc; PTN, ProTaper Next instrument; HYF, Hyflex; CM, controlled memory; MTR, MTwo Retreatment; WO, WaveOne; n, number per group; DRR, D-RaCe Retreatment; WVC, warm vertical condensation; PT, ProTaper.
The symbol a indicates that a test was applied; b indicates no significant differences between groups; c indicates significant differences between groups.
Remaining filling materials
The amount of remaining filling material was measured in 9 studies, mainly using micro-computed tomography (micro-CT) [121618242837] and cone-beam computed tomography (CBCT) [44]. In 2 studies, rotary movement was more effective in removing filling material from curved root canals than reciprocating systems [1228]. In contrast, most studies found no significant difference in filling material removal from curved root canals between these kinematics [16182429373944].
Time required for filling removal
Nine studies measured the time required for filling removal [121617182937384044]. Reciprocating kinematics showed significantly faster filling removal than rotary kinematics in 2 of these studies [2638], while the opposite occurred in 2 studies [1240]. No significant differences were stated in 5 studies [1617183744].
Dentin removal and debris extrusion
No significant difference was found in the volume of dentin removed between both kinematics [1637]. Of 4 studies [17383941], 2 studies found no significant differences between the evaluated kinematics in the amount of apically extruded debris [3941]. A reciprocating system was associated with less apical extrusion in 1 study compared to a rotary system [17], while another study found the opposite [38].
Alterations in the instruments
One study measured NiTi composition and the average roughness of instruments both before and after retreatment [43]. The NiTi composition remained unaffected by the reciprocating system, but it was affected by the rotary system. However, no significant differences in the surface topography were observed between both systems.
Risk of bias and meta-analysis
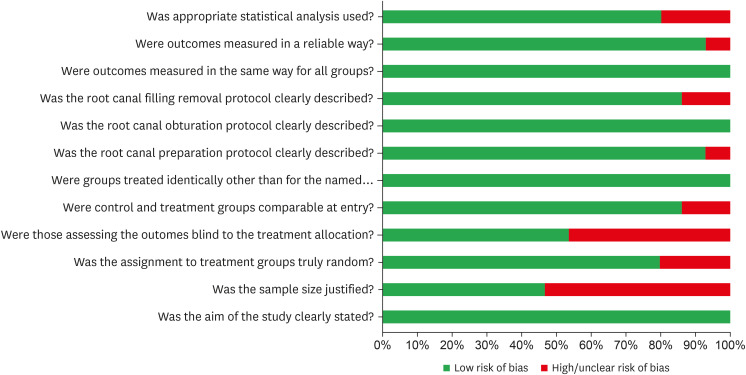
Figure 2 summarizes the results of the risk of bias assessment. Five studies had the highest possible score [1639414244], due to the justification of the sample size and an indication of the presence of a blinded operator. All the included articles showed a clearly stated aim. A low risk of bias was also found for sample randomization, possibility of comparison between control and treatment groups, baseline equivalence of control and treatment groups, clear root canal preparation protocol, clear root canal filling protocol, clear root canal filling removal protocol, measurement method, measurement standardization, and adequate statistical analysis. Nevertheless, a high risk of bias was observed for specific items, such as justification of the sample size and blind treatment allocation.
Figure 2
Assessment of the risk of bias in the included studies according to the percentage of the scores assigned to each evaluated study.
A meta-analysis was not performed due to wide variations in materials, systems, and protocols used for root canal filling and filling removal among the included in vitro studies. In addition, a lack of available data was observed for some evaluated outcomes.
DISCUSSION
This systematic review compared rotary and reciprocating kinematics with respect to their efficacy and safety in the removal of filling material from curved root canals. Efficacy was analyzed based on the remaining filling material in the canal and the time required for filling material removal. For safety, the centering ability, instrument failure, debris extrusion, dentin removal, and NiTi alloy composition before and after retreatment were analyzed. Only studies that directly compared filling removal using at least 1 instrument from each kinematic system were eligible for this review. Based on the review results, most studies showed no differences in efficacy and safety between rotary and reciprocating kinematics during filling material removal from curved canals. A meta-analysis was not performed due to the heterogeneity among the groups of the included studies.
During non-surgical retreatment, complete removal of the root canal filling material was encouraged for the success of retreatment [363946]. This procedure is challenging, mainly in well-filled curved canals due to their complex anatomy, which jeopardizes the cleaning process and increases the risk of accidents [1229]. The studies considered in this review evaluated the performance of systems in filling material removal from mostly severe to moderately curved root canals, where the degree of root canal curvature was classified as moderate when it ranged between 10º and 25º, and severe when the curvature was > 25º [15].
Among the 15 selected studies, 9 studies measured the volume of filling material remnants, of which 7 studies reported no difference between rotary and reciprocating kinematics [16182429373944]. Other investigations using straight root canals [26274647] also found that most of the instruments were not able to completely remove the filling material.
The persistence of the residual filling material could be attributed to the incapacity of instruments to touch all parts of the dentinal walls [24]. Unlike most investigations, only 1 study reported complete removal of the filling material in more than half of the samples [12]. According to the authors, the circular shape of the mesial root canals examined may explain these findings [12]. Furthermore, the combination of instruments with organic solvents during gutta-percha removal was not reported in the studies included in this systematic review. Therefore, the efficacy of the systems for removing gutta-percha may not have been influenced by the use of additional agents.
Differences in the materials used for root canal filling and the filling removal protocols may influence the results. Previous studies have described superior performance of reciprocating systems in the removal of epoxy resin-based and calcium silicate-based sealers from straight and oval canals [4647]. In this systematic review, most studies used gutta-percha as a standard material with different endodontic sealers, primarily using epoxy resin-based sealers. Unlike previous studies using straight canals, the type of instrument did not influence filling removal from curved root canals regardless of the sealer used. Therefore, the complex anatomy of curved canals may potentially impact these research findings.
Another factor that can influence the results is the taper of instruments. Instruments with a greater taper have superior filling removal ability and promote higher root canal enlargement [47], although they may cause weakening of the root due to excessive dentin removal [1628]. Thus, it is important that other systematic reviews consider other instrument characteristics to identify whether there are any specific characteristics that influence the removal of filling material, as we did not find such factors when comparing the efficacy of filling removal between rotary and reciprocating kinematics.
Most studies reported no differences between rotary and reciprocating systems with respect to the time required to reach the working length [1617183744]. Nine studies carried out this analysis, and the Reciproc system (REC) was the most frequently analyzed. This system was developed with an S-shaped cross-section with sharp cutting edges, which increases its cutting ability and removes the obturating material more rapidly [12222946]. Perhaps for this reason, REC was the most frequently studied reciprocating system. Despite this, we found no significant difference in 3 studies that compared REC with rotary systems. In 1 study, the Mtwo retreatment (MTR) system was faster than REC. MTR was designed for retreatment and presents an active angle in the transition between the tip and the helical shaft that increases its cutting ability [12]. However, in another study, REC was faster than MTR and other rotary systems [38].
Although some systems are specially designed for retreatment, either they were not fast enough or did not remove more filling material than regular reciprocating systems [182438]. Likewise, single-file reciprocating systems were not superior to other systems. These results may also be influenced by the operator’s experience and anatomical variations of the teeth. From the included articles, only 2 studies reported the presence of an experienced endodontic specialist who performed all the procedures [2428]. This variable is often associated with superior operator training with rotary and reciprocating file systems, and it may impact the quality of filling removal, particularly in cases of complex root canal anatomy. Additionally, different materials may interfere with the adherence of the obturation material to canal walls, thus influencing the time spent for filling removal [39].
In the safety analysis, few articles assessed apical transportation and centering ability during filling material removal in curved canals. We did not find other systematic reviews that evaluated these factors, even in straight root canals during filling removal. One review compared rotary and reciprocating kinematics in endodontic instrumentation considering these factors [25]. The authors concluded that reciprocating instruments have a lower tendency for apical transportation than rotary instruments [25]. However, due to the small number of studies that evaluated apical transportation and centering ability during retreatment of curved canals, we were unable to conclude which type of kinematics was superior.
Significant flexural fatigue stresses at the point of maximum canal curvature can increase the incidence of file separation in curved root canals, mainly in the mesiobuccal roots of mandibular molars [48]. Although most articles concluded that there were no significant differences in the amount of file plastic deformation and fractures between rotary and reciprocating kinematics [173743], some studies argued that instruments with a low modulus of elasticity should be preferred for canal filling removal in severely curved root canals due to their increased flexibility [4044]. In addition, files were discarded and evaluated after 1–4 uses, depending on the study, or if a visible deformation occurred. Some authors preferred to use each instrument in 3–4 root canals [173740], simulating a molar retreatment. The incidence of instrument failure was considerably low, and it may have been related to differences in canal curvature among the specimens used in each article. Although 1 study reported the use of each set of files in a single canal [44], only mesial canals with curvature angles > 35° were chosen, which may have caused an increase in the number of fractured instruments.
Some factors, such as the number of instruments, instrument design, and kinematics, may favor apical debris extrusion [41]. Clinically, extruded debris is related to the persistence of periradicular tissue inflammation [3941]. There was no difference in the amount of apically extruded debris between rotary and reciprocating kinematics in 2 studies [3941]. One study showed more debris extrusion with the REC system [38], while another showed less debris with the WaveOne system [17]. These studies differed in some of the systems compared and in the final preparation protocols. Nevertheless, similar to this review, other systematic reviews [2549] stated that there were no significant differences in the amount of apically extruded debris between both kinematics.
Few studies have assessed other safety-related variables such as dentin removal and NiTi alloy composition before and after retreatment between rotary and reciprocating kinematics in curved canals, making it difficult to discuss this issue thoroughly. For instance, only 1 article evaluated NiTi composition and the average roughness of instruments both before and after retreatment procedures, which makes it impossible to systematically analyze the data. Thus, more investigations are required to obtain strong evidence for these outcomes.
A crucial step in systematic reviews is to evaluate the individual risk of bias of eligible records. In this review, a version of the JBI critical appraisal tool was chosen for assessing methodological and reporting quality of the studies. Failures to describe the sample size justification and evaluator blinding were problems observed in almost half of eligible studies. These items should be implemented in the study design and reporting of in vitro studies, since they can directly impact the validity and level of confidence in the research findings. However, a low risk of bias and adequate reporting were present for the majority of the items, which may lead to more accurate overall conclusions in this systematic review.
This systematic review elucidated that there is no difference in the efficacy of root canal filling removal between rotary and reciprocating kinematics. Although most studies in this systematic review showed a low risk of bias, some limitations, such as no justification of the sample size and absence of blinding, were noticed. Additionally, a high level of methodological heterogeneity among the studies was observed, such as wide variations in the rotary and reciprocating systems that were used, for which reason a meta-analysis could not be performed. These limitations need to be considered when interpreting the results, especially regarding the design of the included studies, and special care should be taken in making assumptions about the results in the clinical context. Future studies should address these methodological issues. Moreover, most assessments followed an in vitro methodology in straight root canals, disregarding local anatomical complexity and using combined filling-removal techniques. Additional investigations considering different anatomical variations, single preparation protocols or other filling materials, and clinical/longitudinal evaluations should be performed to confirm the results.
CONCLUSIONS
The high-quality evidence from this review suggests that the type of kinematics (rotary or reciprocating) does not influence the efficacy of root canal filling removal from curved root canals. Further studies are needed to compare the safety of the rotary and reciprocating kinematics in the removal of filling material from curved root canals.
 XML Download
XML Download