

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The primary goal of root canal treatment is to eliminate and prevent re-infection of the root canal system [1]. In necrotic teeth, microorganisms can colonize anatomical complexities, such as isthmuses, ramifications and dentinal tubules [2]. Instrumentation can reduce the bacterial load by approximately 80% [3]. However, the microorganisms cannot be completely eliminated, because the instruments are unable to fully reach the anatomical complexities of the root canal system [2]. For this reason, irrigation is the key to successful treatment, since it is the only way to reach areas left untouched by instrumentation [4].
Sodium hypochlorite (NaOCl) is the most widely used solution, owing to its antimicrobial/antibiofilm activity, and organic tissue dissolution capacity [567]. Additionally, since NaOCl cannot remove inorganic tissue, 17% ethylenediaminetetraacetic acid (EDTA) is recommended to address this limitation [8].
Traditionally, the irrigant is delivered to the root canal through a needle coupled to a syringe, a system known as conventional syringe irrigation (CSI) [9]. CSI has a rinsing effect, which is an important part of the irrigation process [10]. However, it does not guarantee that the irrigant will reach the working length and anatomical complexities [911]. Furthermore, CSI can exert positive pressure that could trigger the extrusion of the irrigant [12]. For this reason, different methods have been introduced to improve the safety and cleaning of the root canal system, such as negative pressure irrigation (EndoVac), and passive ultrasonic irrigation (PUI) [1314].
The GentleWave system (GW) (Sonendo, Laguna Hills, CA, USA) was introduced on the US market in 2014, and represents a type of endodontic device developed for cleaning and disinfection of the root canal [15]. According to its manufacturer, GW can be used in situations that need only minimal instrumentation, instead of using conventional instrumentation, which may contribute to maintain tooth resistance [1617]. That is because the widening of the root canal can lower the fracture resistance of the root; however, there is still no consensus that minimal instrumentation has this effect [1819].
GW creates a powerful, high speed shear force that dispenses irrigants into the root canal system, without having to place the tip of the handpiece into the canal orifice [2021]. Specifically, the implosion of microbubbles creates an acoustic field of broadband frequencies that travel through the fluid to reach the entire root canal system, thereby cleaning the soft tissues, and eliminating the bacteria within the root canals [2021]. Additionally, GW provides negative pressure irrigation, which ensures less apical extrusion of the irrigant [1222]. The equipment can be used with NaOCl, EDTA and distilled water [17]. The irrigant is dispensed from the handpiece, coupled to the tooth, at a speed of 45 mL/min [23], and the excess irrigant is removed concurrently [22].
Currently, GW costs approximately $85,000.00 per console, and $100.00 for a onetime use handpiece. However, several doubts have been raised in regard to GW: Is it worth investing in such high-cost equipment? Does it produce better results than conventional root canal treatment? What are the effects of GW on endodontic treatment? Therefore, the present literature review addressed the scientific evidence on the use of the GW, providing a detailed description of in vitro and clinical studies.
REVIEW
Electronic search
The electronic search was performed on MEDLINE (PubMed platform), Web of Science, Scopus, Science Direct and Embase databases. The search string was (“Gentlewave” OR “Multisonic Ultracleaning”) AND (“endodontics” OR “root canal treatment”). The last search was conducted in July 2021. In addition, a manual search was performed in Google Scholar, and the following journals: Journal of Dentistry, Journal of Endodontics, International Endodontic Journal, Clinical Oral Investigations, Restorative Dentistry & Endodontics, and Australian Endodontic Journal. The language was restricted to English.
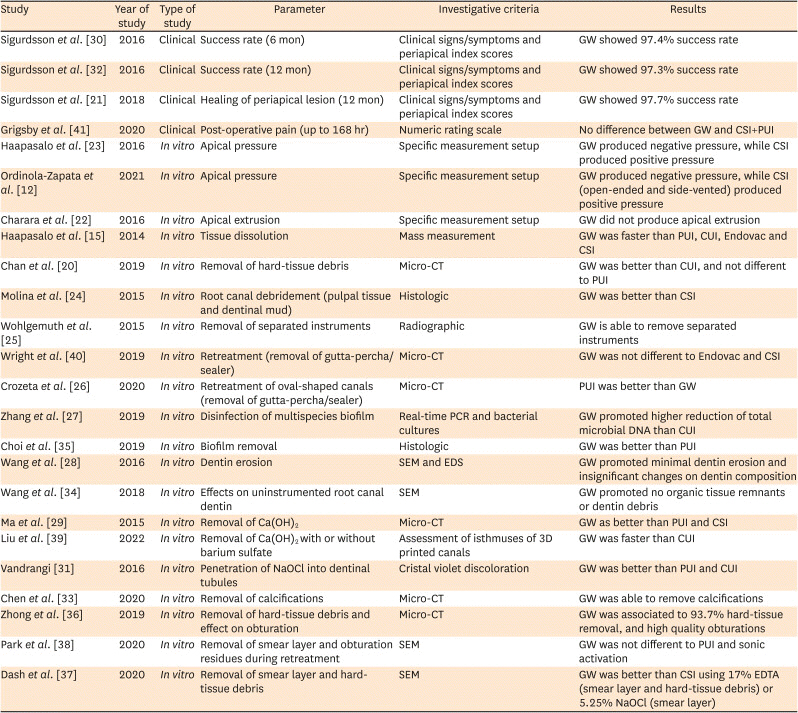
A total of 24 studies from August/2014 to July/2021 were collected (20 in vitro and 4 clinical-focused), and all focused on relating the effects of GW on root canal treatment (Table 1).
Table 1
Summary of in vitro and clinical studies that used the GentleWave system on root canal treatment
| Study | Year of study | Type of study | Parameter | Investigative criteria | Results |
|---|---|---|---|---|---|
| Sigurdsson et al. [30] | 2016 | Clinical | Success rate (6 mon) | Clinical signs/symptoms and periapical index scores | GW showed 97.4% success rate |
| Sigurdsson et al. [32] | 2016 | Clinical | Success rate (12 mon) | Clinical signs/symptoms and periapical index scores | GW showed 97.3% success rate |
| Sigurdsson et al. [21] | 2018 | Clinical | Healing of periapical lesion (12 mon) | Clinical signs/symptoms and periapical index scores | GW showed 97.7% success rate |
| Grigsby et al. [41] | 2020 | Clinical | Post-operative pain (up to 168 hr) | Numeric rating scale | No difference between GW and CSI+PUI |
| Haapasalo et al. [23] | 2016 | In vitro | Apical pressure | Specific measurement setup | GW produced negative pressure, while CSI produced positive pressure |
| Ordinola-Zapata et al. [12] | 2021 | In vitro | Apical pressure | Specific measurement setup | GW produced negative pressure, while CSI (open-ended and side-vented) produced positive pressure |
| Charara et al. [22] | 2016 | In vitro | Apical extrusion | Specific measurement setup | GW did not produce apical extrusion |
| Haapasalo et al. [15] | 2014 | In vitro | Tissue dissolution | Mass measurement | GW was faster than PUI, CUI, Endovac and CSI |
| Chan et al. [20] | 2019 | In vitro | Removal of hard-tissue debris | Micro-CT | GW was better than CUI, and not different to PUI |
| Molina et al. [24] | 2015 | In vitro | Root canal debridement (pulpal tissue and dentinal mud) | Histologic | GW was better than CSI |
| Wohlgemuth et al. [25] | 2015 | In vitro | Removal of separated instruments | Radiographic | GW is able to remove separated instruments |
| Wright et al. [40] | 2019 | In vitro | Retreatment (removal of gutta-percha/sealer) | Micro-CT | GW was not different to Endovac and CSI |
| Crozeta et al. [26] | 2020 | In vitro | Retreatment of oval-shaped canals (removal of gutta-percha/sealer) | Micro-CT | PUI was better than GW |
| Zhang et al. [27] | 2019 | In vitro | Disinfection of multispecies biofilm | Real-time PCR and bacterial cultures | GW promoted higher reduction of total microbial DNA than CUI |
| Choi et al. [35] | 2019 | In vitro | Biofilm removal | Histologic | GW was better than PUI |
| Wang et al. [28] | 2016 | In vitro | Dentin erosion | SEM and EDS | GW promoted minimal dentin erosion and insignificant changes on dentin composition |
| Wang et al. [34] | 2018 | In vitro | Effects on uninstrumented root canal dentin | SEM | GW promoted no organic tissue remnants or dentin debris |
| Ma et al. [29] | 2015 | In vitro | Removal of Ca(OH)2 | Micro-CT | GW as better than PUI and CSI |
| Liu et al. [39] | 2022 | In vitro | Removal of Ca(OH)2 with or without barium sulfate | Assessment of isthmuses of 3D printed canals | GW was faster than CUI |
| Vandrangi [31] | 2016 | In vitro | Penetration of NaOCl into dentinal tubules | Cristal violet discoloration | GW was better than PUI and CUI |
| Chen et al. [33] | 2020 | In vitro | Removal of calcifications | Micro-CT | GW was able to remove calcifications |
| Zhong et al. [36] | 2019 | In vitro | Removal of hard-tissue debris and effect on obturation | Micro-CT | GW was associated to 93.7% hard-tissue removal, and high quality obturations |
| Park et al. [38] | 2020 | In vitro | Removal of smear layer and obturation residues during retreatment | SEM | GW was not different to PUI and sonic activation |
| Dash et al. [37] | 2020 | In vitro | Removal of smear layer and hard-tissue debris | SEM | GW was better than CSI using 17% EDTA (smear layer and hard-tissue debris) or 5.25% NaOCl (smear layer) |
Ca(OH)2, calcium hydroxide; CSI, conventional syringe irrigation; CUI, continuous ultrasonic irrigation; EDS, energy dispersive X-ray spectroscopy; EDTA, Ethylenediaminetetraacetic acid; Micro-CT, microcomputed tomography; NaOCl, sodium hypochlorite; PCR, polymerase chain reaction; PUI, passive ultrasonic irrigation; SEM, scanning electron microscopy; GW, GentleWave system.
1. The GentleWave system
The GW system consists of a console, a handpiece similar to a conventional dental handpiece, and a trash container. A prerequisite for using GW is making sure that the pulp chamber is sealed to prevent communication with the oral cavity, thus preventing NaOCl mist from spreading to the work area. The handpiece tip should be positioned 1mm above the pulp chamber floor when used, to ensure that it does not enter the canal orifices. A touchscreen control panel on the console allows high speed flow regulation of the irrigant to the handpiece, where the irrigant strikes a metal strike plate at the end of the tip, thereby triggering the release of a spray from the tip [15]. The irrigants undergo a degassing process to eliminate the dissolved gas present in the solution, thus optimizing the energy supply through the root canal, and eliminating the vapor-lock effect [16]. When the solution passes from the handpiece into stagnant fluids in the pulp chamber, hydrodynamic cavitation is triggered by shear forces, forming thousands of microbubbles called cavitation clouds. These bubbles implode and create sound waves that cover a wide spectrum of frequencies (Multisonic Ultracleaning spectra) and reverberate throughout the root canal system to achieve more thorough cleaning [2425]. The handpiece has a 5-point vented suction system that collects excess NaOCl from the pulp chamber [15]. Usually, the protocol is 3% NaOCl for 3 or 5 minutes, followed by rinsing with water for 15 or 30 seconds, 8% EDTA for 2 minutes, and a final rinse with distilled water for 15 or 30 seconds [242526272829]. The irrigation flow is 45 mL/min; in other words, 3 or 5 minutes of irrigation with NaOCl is equivalent to 135 mL or 225 mL [15].
2. Root canal instrumentation for the GentleWave procedure
The GW is designed to reduce the need for enlarged instrumentation by applying a minimally invasive endodontic technique designed to preserve dentin [30]. Irrigation protocols with GW call for minimal instrumentation, which includes the use of small files, usually 15.04, S1 ProTaper file with #17 size tip, F1 ProTaper file (20.07), 20.04 or 20.06 [212224272830313241]. Furthermore, GW follows a conservative philosophy by recommending its use without cervical preflaring [22]. In fact, depending on the research objectives, there are studies that have used GW in non-instrumented canals [3334]. However, this does not mean that GW cannot be used in canals submitted to conventional instrumentation, defined as enlargement to a minimum size of 25.06, or else 25.07, 30.04, 40.04 or greater [122034].
3. Apical pressure and apical extrusion
NaOCl extrusion is an accident that can lead to complications, such as pain, swelling, and ecchymosis [42]. The apical pressure exerted by GW has been previously evaluated in maxillary and mandibular molars [1223]. The first study evaluated the apical pressure generated by GW versus CSI, using 30G open-ended and side-vented needles at 1 and 3 mm of the working length of the palatal and distobuccal canals of maxillary molars. Apical pressure levels were measured after no instrumentation, minimal instrumentation with 15.04, conventional instrumentation up to 40.04, and also after enlargement of the apical foramen to size #40. Irrigation with GW generated negative apical pressure (between −13.07 and −17.19 mm Hg), whereas CSI generated positive pressure (6.46 mmHg for side-vented, and 110.34 mmHg for open-ended). The negative apical pressure of GW was not affected by the size of the instrumentation or by the apical foramen [23]. The second study corroborated these observations. The authors evaluated the apical pressure produced by GW in mesial and distal canals of mandibular molars, compared with CSI using 30G open-ended and side-vented needles. The GW generated negative pressure (−30.79 mm Hg), and the 2 needles generated positive pressure, which was lower for the side-vented needle in mesial canals −0.77 mmHg [12].
The apical extrusion of the irrigant produced by GW was compared with that of CSI using a 30G side-vented needle and EndoVac in mesial and distal canals of mandibular molars. The teeth were instrumented up to different sizes (minimal instrumentation up to 15.04, conventional instrumentation up to file 35.06, and over-instrumentation with the 35.06 file exceeding the working length by 1 mm). There was no apical extrusion in the GW and EndoVac groups. In the CSI group, extrusion ranged between 0.000–1.373 g, and was higher in the distal canals, especially after conventional instrumentation and over-instrumentation [22]. As described in the aforementioned studies, GW produces negative apical pressure, which prevents significant extrusion of the irrigant.
4. Organic dissolution ability
Bovine muscle was exposed to 0.5%, 3% and 6% NaOCl for 5 minutes at 21°C and 40°C using GW, PUI (Piezon Master 700 agitation), and continuous ultrasonic irrigation (CUI; Piezon Master 700 agitation plus irrigation), EndoVac and CSI. GW promoted the fastest dissolution, at a rate of 1.0% per second in 0.5% NaOCl, 2.3% per second in 3% NaOCl, and 2.9% per second in 6% NaOCl. This rate was significantly greater than all other devices. The authors suggested that some form of physical energy created by GW may be responsible for this rapid tissue-dissolving effect [15].
5. Effects on root canal dentin
Wang et al. [34] evaluated the morphology of the dentin of non-instrumented premolars irrigated with GW. The analysis of the scanning electron microscopy (SEM) images showed no remains of organic tissue, biofilm, or debris, and more open dentinal tubules. They concluded that the root canals could be cleaned completely without instrumentation, when using GW. Regarding the effects on dentin erosion and dentin composition, a study using SEM images and energy-dispersive X-ray spectroscopy, respectively, revealed that irrigation with GW (using 3% NaOCl, 8% EDTA and water) caused minimal dentin erosion, and minor or insignificant changes in the relative proportions of carbon, oxygen, calcium, and phosphorus in circumpulpal dentin, similar to the effects of CSI using NaOCl followed by final irrigation with EDTA [28].
6. Removal ability
1) Biofilm
The ability of GW to remove multi-species or Enterococcus faecalis (E. faecalis) biofilm compared with CUI and PUI has already been assessed [2735]. In the first study reviewed, GW was compared in vitro with CUI (ProUltra PiezoFlow) for removing multispecies oral biofilms from canals using quantitative real-time polymerase chain reaction. Root canals were minimally instrumented up to 15.04 (Vortex Blue) for the GW group, and up to 35.04 for the CUI group. Although both systems demonstrated a highly effective reduction in intracanal bacterial DNA, GW showed a more constant and significantly greater reduction in total microbial DNA, E. faecalis DNA and Streptococcus spp DNA, compared with CUI [27]. Another study was conducted to evaluate the efficacy of GW and PUI (Piezon Master 700 ESI tip activation) in removing E. faecalis biofilm. The teeth were submitted to conventional instrumentation (F2 ProTaper + 35.04 EndoSequence) plus PUI, and minimal instrumentation (15.04, EndoSequence) plus GW. Histological analysis indicated that GW enabled higher biofilm removal in the main canal and isthmus regions, compared with PUI [35].
2) Pulp tissue
The efficacy of GW in removing debris (a combination of soft pulp tissue and dentinal mud) was assessed histologically in comparison with CSI. The teeth from the “conventional instrumentation + CSI” group were instrumented using .04 taper files (Vortex Blue), depending on the apical size of each specimen, and irrigated with a 30G side-vented needle, whereas the teeth of the GW group were minimally instrumented (15.04, EndoSequence), and irrigated with GW. The GW eliminated 97.2% and 98.1% of debris in the apical and middle thirds of the mesial canals in mandibular molars, and mesiobuccal canals in maxillary molars, respectively, while CSI eliminated 67.8% and 87.3% respectively. In the distal root, debridement was similar in both groups. The authors concluded that GW promoted greater debridement than CSI [24].
3) Calcifications
The ability of GW to remove calcifications of distal canals of non-instrumented mandibular molars was assessed using micro-computed tomography (micro-CT) images. By using GW, the average total volume of the canals increased from 5.11 mm3 to 5.50 mm3, and 86.4% of the calcifications were reduced. It was concluded that GW can eliminate the calcifications totally or partially, even without previous root canal instrumentation [33].
4) Hard-tissue debris and smear layer
Although GW proved effective in removing hard-tissue (93.7%) after minimal instrumentation, based on micro-CT assessment [36], a study that used SEM images revealed no differences compared with CSI using 17% EDTA as a final irrigation, with photodynamic therapy (PDT) or with Er:YAG laser irradiation [37]. The exception was in the apical third, where GW removed more hard-tissue debris than CSI using 17% EDTA [37]. Another study, using micro-CT images in mandibular molars instrumented with “Small” and “Primary” files (WaveOne Gold), reported that GW promoted higher removal of hard-tissue debris in root canals (96.4%) and isthmuses (97.9%) than CUI (80.0% and 88.9%, respectively); however, the results for GW were no different from those of PUI (91.2% and 93.5%, respectively) [20].
Regarding smear layer removal, GW was no different from the ultrasonic systems, PDT or Er:YAG [2037]; however, GW was better than CSI using 17% EDTA or 5.25% NaOCl as a final irrigation [37]. A study analyzing retreated distal canals of molars reported that GW, a PUI system (ENDOSONIC Blue system coupled to a 17.02 file), and sonic agitation with EDDY tips showed higher smear layer removal than another PUI system (Piezon Master 700 coupled to a ESI 15.02 tip), and the negative control (CSI in non-obturated canals), in the middle third. In the apical third, GW, both PUI systems (ENDOSONIC and Piezon Master 700) and EDDY tips provided higher smear layer removal than the negative control [38].
5) Root canal dressing
Regarding this topic, there are 2 studies available [2939]. In the first one, mandibular molars were instrumented up to 25.08 (mesial canals, WaveOne Gold) and 40.08 (distal canals, WaveOne Gold), and the root canals were filled with Metapaste (containing calcium hydroxide and barium sulfate). After 7 days, the Metapaste was removed using: 1) GW, 2) conventional instrumentation (using the same WaveOne Gold file) plus CSI, or 3) conventional instrumentation plus PUI. The micro-CT analysis revealed that CSI and PUI did not completely remove Ca(OH)2. In the apical third of the mesial and distal canals, CSI removed 47.82% and 77.68%, PUI removed 61.66% and 88.85%, and GW removed significantly more Ca(OH)2, that is, 100% and 98.78%, respectively [29]. The second study compared CSI (open-ended needle and double-side-vented needle), PUI (EndoUltra, coupled to 15.02 tip), CUI (ProUltra PiezoFlow) and GW in the removal of Ca(OH)2 with and without barium sulfate at different proportions from isthmuses of 3D printed transparent root canals. The authors reported that only GW and CUI removed the pastes completely, being GW faster than CUI (2–3 times) [39]. Considering that only 2 studies are available on this important topic, further research should be conducted to derive a stronger clinical correlation.
6) Root canal obturation residues
GW has been compared with CSI, PUI, EndoVac and sonic irrigation [263840]. Crozeta et al. [26] performed a micro-CT assessment, and reported that both GW and PUI significantly reduced the volume of obturation material (gutta-percha and AHPlus sealer) remaining from previously instrumented oval canals (R40, Reciproc). Both GW and PUI played a complementary role after initial retreatment using the R50 file (Reciproc). GW was able to remove approximately 10% of the remaining obturation material from the entire canal, while PUI removed 18%, hence achieving better performance. However, another study that used SEM images to assess the debris (residual filling material, dentinal mud and smear layer) revealed no significant differences among GW, PUI systems (Piezon Master 700 and ENDOSONIC Blue system), sonic agitation using EDDY tips, and the negative control (CSI in non-obturated canals) in distal root canals previously retreated with ProTaper Retreatment and ProTaper files [38]. Moreover, the ability of GW to remove root canal obturation was found to be no different from EndoVac or CSI (using a side-vented needle) in canals whose initial retreatment was performed using a .06 tapered heated plugger and ProFile files (up to 20.04) [40].
7) Separated instruments
A study revealed that GW removed separated stainless steel instruments from the root canal [25]. Briefly, 2.5 mm fragments of #10, #15 and #20 K-type files were placed in the middle and apical thirds of extracted molars. The molars were distributed into 2 groups according to the curvature of the root (< 30º and > 30º) and treated with GW. GW promoted greater fragment removal in the middle third (83%) compared to the apical third (61%). Regarding root curvature, GW was more successful in less curved canals (91%) than in more curved canals (42%). The #10, #15, and #20 K-type file fragments were removed 75%, 92%, and 50%, respectively. Additionally, the mean treatment time to remove the fragment was 10 minutes and 44 seconds.
7. Penetration of NaOCl into dentinal tubules
The penetration of irrigants into dentinal tubules is important because bacterial invasion in teeth that present pulpal necrosis has been previously reported [43]. This aspect of GW was compared with that of PUI (Piezon Master 700 coupled to ESI 15.02 tip), and that of CUI (Piezon Master 700 using ESI tip with maximum irrigation rate) in minimally instrumented molars (15.04, EndoSequence) pre-stained with crystal violet. GW promoted higher penetration depth of NaOCl in the coronal, middle and apical thirds than PUI and CUI. The authors concluded that the penetration promoted by GW was 4 times as deep as that of ultrasonic systems [31].
8. Effect of GW on final obturation
The effect of GW on the final obturation after minimal instrumentation of root canals of maxillary molars (15.04, Vortex Blue) was evaluated using micro-CT images [36]. The root canals were filled using a modified single cone technique with 3 different sealers: GuttaFlow Bioseal, GuttaFlow 2 and MTA Fillapex. The sealers provided an 89.5%–98.9% filled canal, pointing out that GuttaFlow Bioseal (96.9%–98.9%) and GuttaFlow 2 (94.7%–97.5%) were higher than MTA Fillapex (89.4%–89.5%). It was concluded that the modified single cone technique using GuttaFlow 2 and GuttaFlow Bioseal sealers resulted in a high-quality obturation after using GW in minimally instrumented molar canals.
9. Clinical studies
Two of the clinical studies that included GW in the protocol treatment assessed the success rate of endodontic treatment after 3 months, 6 months and 12 months, and a third evaluated healing of the periapical lesion after 12 months [213032]. Regarding the studies reporting the success rate of endodontic treatment using GW, a multicenter prospective study using 89 teeth indicated that the success rate after 3 months was 92% [32]. After 6 months, 77.9% of the vital or necrotic teeth were classified as “healed,” 19.5%, as “healing,” and 2.6%, as “diseased.” In other words, when combining “healed” with “healing,” 97.4% were classified as “successful”. No comparison was made with any other type of treatment protocol. Additionally, the preoperative presence of a periapical lesion (periapical index [PAI] ≥ 3), and a single session were correlated with a “diseased” episode [30]. After 12 months, the success rate was 97.3% [32]. The third study aforementioned resulted from 2 clinical studies. It reported that the healing of periapical lesions (PAI ≥ 3) was 97.7% after 12 months. Of these, 81.8% were classified as “healed,” and 15.9%, as “healing.” Only one tooth was classified as “diseased” [21].
These 3 studies also evaluated postoperative pain associated with GW, using the visual analog scale [213032]. In the first study, which assessed 6-month healing rates, no patient experienced severe pain, while only 3% of the patients experienced moderate pain 2 days after treatment [30]. These observations were updated in the second study, which assessed the 12-month success rate, and in which only 3.8% of the patients experienced moderate pain 2 days after treatment [32]. The third study addressed teeth with a pre-existing periapical lesion (PAI ≥ 3), and indicated that 15.6% of the patients reported mild pain 2 days after treatment. Additionally, at 2, 7, and 14 days after treatment, no patient experienced moderate or severe pain [21]. Another randomized clinical study evaluated the incidence and intensity of postoperative pain using the numeric rating scale for patients who received instrumentation (at least 25.04) plus CSI and PUI (control group), or minimal instrumentation (20.04 or 20.06) plus irrigation with GW (GW group). After 168 hours (7 days), 72% of the patients in the control group had at least one episode of low to mild pain, versus 83.3% of those in the GW group. There was no significant difference between the 2 groups [41].
Although the manufacturer suggests the use of GW in a single-visit [16], different impediments such as time constraints, presence of separated file, device availability make necessary to perform endodontic treatment in multiple visits [21]. The same studies that evaluated postoperative pain, success rate (clinical and radiographic) and healing of periapical lesions also took into consideration the number of visits [21303241]. After 6 months, a 93.3% success rate was observed in patients who were treated with GW in a single visit. A positive correlation was observed between single-visit and success [30]. However, after 12 months (84.3% recall rate), although the success rate remained high when single-visit was performed, 97.2%, there was no correlation between the number of visits and success [32]. A study that assessed healing of periapical lesions after 12 months (97.7% success rate) revealed that most of the patients (88.9%) were treated in a single visit [21]. Another study that evaluated postoperative pain revealed that 83.3% of patients were treated in 2 visits, with most of the pain eliminated between appointments [41].
10. Limitations
The main limitation of GW is its cost, which would require a financial effort from the clinician. Additionally, GW uses a maximum of 3% NaOCl and 8% EDTA, which can be supplemented with water rinse [32]. This could be considered as a limitation since irrigants at higher concentrations, with different additives (such as surfactants) or alternative/experimental irrigants cannot be used. Regarding the handpiece, it needs vertical space to be attached to the tooth, therefore, structurally compromised teeth should be sufficiently restored to allow a proper attachment, i.e., 1 mm above the pulp chamber floor [15]. Another important aspect to be considered is that most of the studies about GW are in vitro, and the number of studies that evaluated the topics of the present review was minimal. Additionally, studies that evaluated clinical/radiographic success did not compare GW with other irrigation protocols, nor the association of minimal or conventional instrumentation on success. Thus, more research, especially clinical, is needed to justify the use of GW over other irrigation methods.
CONCLUSIONS
Based on the limited evidence/literature available, the GW System was not associated with extrusion of the irrigant, promoted faster organic dissolution than CSI, PUI CUI and EndoVac, reduced more bacterial DNA and biofilm than PUI and CUI, promoted higher penetration of NaOCl into dentinal tubules than PUI and CUI in vitro, and removed more intracanal medication than CSI and PUI. GW was able to remove pulp tissue and calcifications. Moreover, its ability to remove hard-tissue debris and smear layer was better than CSI, and its ability to remove root canal obturation residues was lower or similar to PUI, and similar to CSI and EndoVac. Regarding the root canal obturation of minimally instrumented molar canals, GW was associated with high-quality obturations. Clinically, the success rate of endodontic treatment using GW was 97.3%, and the short-term postoperative pain was no different between the GW and the CSI groups. Further research, mainly clinical, is needed to establish whether GW has any advantages over other available irrigation methods.
 XML Download
XML Download