

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Periapical lesions are inflammatory lesions that form around roots of the teeth as a consequence of bacterial infection within the pulp canal [1]. The most common human periapical inflammatory lesions encountered in clinical practice are periapical abscesses, granulomas, and cysts. They can form in response to chronic irritation due to microbial and chemical stimuli, activated immune response, and bone resorption in periapical tissues [23]. Periapical cysts (PCs) evolve from epithelial remnant cells within periapical granulomas (PGs), with the formation of the cystic lumen caused by a chronic inflammatory reaction [4]. The accurate diagnosis of a periapical lesion as a cyst or granuloma helps dentists choose a precise treatment strategy [5].
Biopsy and histopathological evaluation are the gold standard to confirm the type of periapical lesions [6]. However, the accurate diagnosis and differentiation of periapical lesions become challenging when the cyst epithelium has degenerated and been replaced by an inflammatory granulomatous lesion. This may occur due to severe bacterial infections or the effects of irrigation during endodontic procedures [7].
Collagen fibers help to maintain structural integrity, determine tissue function, and provide tensile strength. Picrosirius red staining accentuates the natural birefringence of collagen fibers and imparts a red, orange, yellow, or green color when viewed under polarized light [8]. The collagen fiber orientation produced by mechanical stress persists for a long time in tissues and can be detected using a polarizing microscope [7]. This property helps to distinguish various skin lesions, odontogenic cysts, and tumors [910].
A vast number of inflammatory cells, chiefly lymphocytes, macrophages, plasma cells, eosinophils, mast cells, and several cytokines, are present in periapical lesions [11]. Mast cells have been detected in the inflammatory infiltrates of granulomas and cysts, suggesting that they may play a role in the inflammatory mechanism of these lesions [2].
Mast cells contain numerous granules that secrete several substances, including leukotrienes and prostaglandins, as well as various pro-inflammatory or mitogenic cytokines [2]. Mast cells influence tissue repair and exhibit properties of collagen synthesis by activating fibroblasts to produce collagen, thereby contributing to wound healing and fibrosis [12]. On the contrary, mast cells also secrete proteolytic enzymes such as tryptase and chymase, which possess collagenolytic properties that lead to the destruction of fibrillar collagen in connective tissue, destroying the extracellular matrix and promoting tissue remodeling [1314].
To date, no study has evaluated the correlation of collagen fibers, mast cells, and their combined role in the behavior of periapical lesions.
Keeping in mind the dual nature of the effect of mast cells on collagen, the present study was conceived with an intent to evaluate collagen fiber bundles and localize mast cell expression in PGs and PCs by polarizing microscopy and immunohistochemistry using picrosirius red staining and mast cell tryptase, respectively.
Go to : 
MATERIALS AND METHODS
Study design and tissue samples
Sixty-eight specimens (34 PGs and 34 PCs) were obtained by retrieving formalin-fixed paraffin-embedded tissue blocks, as well as new biopsy specimens submitted to the Department of Oral and Maxillofacial Pathology and Oral Microbiology, Post Graduate Institute of Dental Sciences, Rohtak, India. The study was approved by the Institutional Ethics Committee (protocol no: PGIDS/IEC/2018/19 dated November 30, 2018).
All PGs and PCs were obtained from human permanent, mature teeth from all dental groups (anterior and posterior) prior to endodontic treatment and their diagnoses were confirmed based on well-defined clinical, radiographic, and histopathological criteria. All selected specimens were cases of periapical radiolucent lesions, associated with non-vital pulp in cases of cysts. PGs showed granulomatous tissue with infiltration of inflammatory cells and without evidence of epithelial lining. PCs were diagnosed as presenting fully developed cavities lined by stratified squamous epithelium with variable thickness and a fibrous wall [2] (Figure 1A-1D).
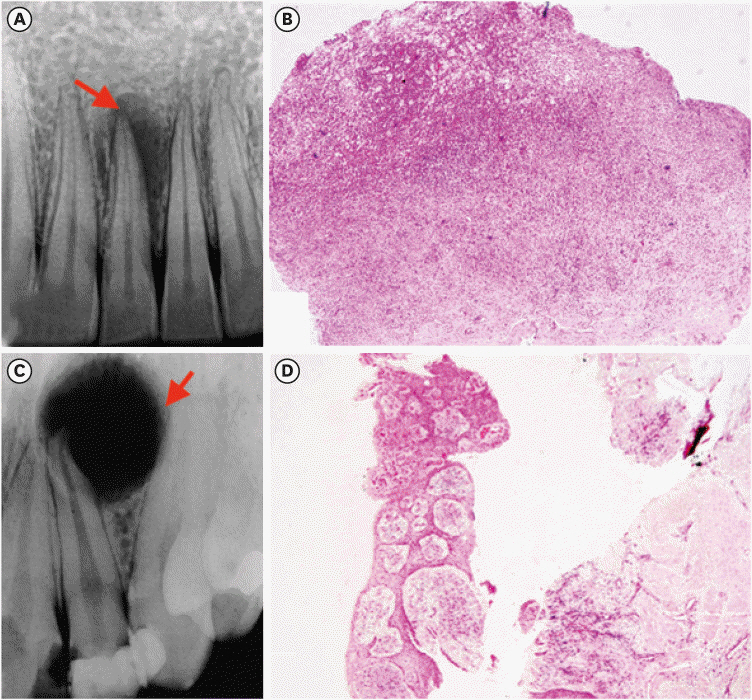 | Figure 1(A, B) A selected periapical granuloma; a periapical radiograph shows a well-defined radiolucency located over the root apex of the right maxillary central incisor (red arrow), and histological sections reveal fibro-cellular connective tissue stroma infiltrated by inflammatory cells and abundant foamy macrophages (H&E ×40). (C, D) A selected periapical cyst; a periapical radiograph shows a well-defined radiolucency, located over the root apex of the right maxillary lateral incisor (red arrow), and histological sections reveal stratified squamous, nonkeratinized epithelial lining with an arcading pattern and underlying fibro-collagenous connective tissue capsule with inflammatory cell infiltrate (H&E ×40).H&E, hematoxylin and eosin.
|
Cases not histologically proven as periapical lesions, as well as patients unwilling to undergo biopsy or who refused to give consent for participating in the study, were excluded. Patients with a history or symptoms of chronic systemic conditions, such as diabetes and hypertension, or endodontically treated teeth were also excluded.
Biopsies were performed in patients willing to participate in the study. The procedure was carried out under local anesthesia. Granulomatous tissue associated with the defective bone was curetted. Osteotomy of 3–4 mm was performed if intact bone was present around the lesion in order to enter into the lesion, followed by removal of the granulation tissue until the root apex was visible. Resection of 3 mm of the root tip was performed perpendicular to the long axis of the root, and further root apex preparation was executed with ultrasonic tips followed by retrofilling [15].
Morphological analysis
1. Hematoxylin and eosin staining
For morphological analysis, 5-µm-thick tissue sections were stained with hematoxylin and eosin for a histopathological diagnosis and evaluation of inflammatory cells. The procedure used Harris hematoxylin and eosin Y staining solutions. The formalin-fixed tissue sections were deparaffinized, followed by rehydration in decreasing grades of alcohol. The tissue sections were stained with hematoxylin for 10 minutes, the slides were then washed with tap water for 2 minutes, and the process of bluing (color change from red to blue) took place. The slides were stained with a filtered eosin stain (4 minutes) and rinsed in tap water. The slides were then cleared in xylene, dehydrated in ascending grades of alcohol, and mounted [16]. Under a bright-field microscope, the intensity of the inflammatory infiltrate was evaluated on a 4-grade scale [17]. Inflammatory cells were counted in 10 random fields at ×100 magnification and divided into 4 grades: grade 0, no inflammation; grade 1, < 15 cells/field; grade 2, 15–50 cells/field; and grade 3, > 50 cells/field. After grading, 2 groups were formed based on the inflammatory score. Group A included grades 0–2, and group B corresponded to grade 3.
2. Picrosirius red staining
Another section was stained with picrosirius red, prepared using the method recommended by Puchtler et al. [18] to determine the collagen fiber birefringence and thickness. In this process, 0.1 g of Sirius Red F3BA was dissolved in 100 mL of saturated picric acid (both from Sigma Aldrich, St. Louis, MO, USA). Next, 5-µm-thick tissue sections were deparaffinized, followed by rehydration in decreasing grades of alcohol and hydration with deionized water. Staining was then done with 0.1% picrosirius red stain for 1 hour at room temperature. Sections were rinsed thoroughly in distilled water, counterstained with Mayer’s hematoxylin (5–6 minutes), and cover-slipped. Tissue sections of fibroma served as a positive control.
3. Assessment of collagen fibers
The color of the collagen fibers was divided into 3 groups for analysis: green (ranging from blue to green), yellow (including yellowish-green and yellowish-orange), and red (including orange and red) [17]. The overall birefringence of the fibers, along with the color patterns of thick and thin fibers, was noted. The percentage of different color fibers in each group was calculated. A total of 150 fibers (50 each in 3 high-power fields at ×40) were measured; based on their width, they were classified as thick (1.2–2.4 μm) or thin (< 0.8 μm), and the mean number of thick and thin collagen fibers was calculated.
Immunohistochemical methods
For the immunohistochemical staining, 4-µm-thick tissue sections were deparaffinized, followed by rehydration in descending grades of alcohol and hydration with deionized water. Antigen retrieval was then done with Tris-EDTA (pH 9) in a pressure cooker. Sections were then incubated with anti-tryptase antibody (monoclonal mouse anti-human mast cell tryptase, clone AA1; Diagnostic Biosystems, Pleasanton, CA, USA) diluted to 1:450 for 50 minutes at room temperature in a humidifying chamber. After 2 washes with phosphate-buffered saline solution, sections were incubated with streptavidin-biotin-peroxidase complex (Biogenex; Telangana, India) for 30 minutes to bind the primary antibodies. Peroxidase activity was visualized by immersing sections in diaminobenzidine (HK124-5K; Biogenex, Telangana, India) chromogen for 10 minutes at room temperature, resulting in a brown reaction product. The sections were counterstained with Mayer’s hematoxylin and cover-slipped. Sections of tonsils and lymph nodes served as positive controls. The negative control comprised sections in which the primary antibody was omitted and replaced by phosphate-buffered saline.
1. Immunostaining assessment
The slides were evaluated under a bright-field research microscope using computerized image software to conduct a morphometric analysis of mast cells. All tissue sections were observed under the light microscope at ×100 magnification to determine the areas presenting with the highest number of tryptase positive mast cells and then their quantification was done at ×400 magnification. Tryptase-positive mast cells were noted in 6 different areas, out of which 3 microscopic fields corresponded to the central portion of the connective tissue and 3 in peripheral portion based on the criteria adapted from Costa Neto et al. [13]. The immunoreactive mast cells were graded according to their granulated or degranulated state, and mean count of tryptase-positive mast cells was calculated.
Three independent observers evaluated the birefringence pattern, thickness of collagen fibers, and mast cell number, along with their granulated or degranulated status. To avoid inter-observer bias, the mean count of the thick and thin collagen fibers and mast cells of all 3 observers was taken as the final value.
Statistical analysis
The results were presented and analyzed using SPSS version 21.0 (IBM Corp., Armonk, NY, USA). The data obtained from the study were checked for normality by applying the Shapiro-Wilk test. Since the data showed non-normality, the Mann-Whitney U test was applied for between-group comparisons. The Spearman rho correlation test was performed to analyze the relationship of collagen fibers with mast cells and inflammatory cells. A p < 0.05 was considered to indicate statistical significance.
Go to :
RESULTS
Morphological analysis
1. Mean inflammatory cell density
The analysis of the intensity of inflammatory infiltrate revealed 13 PCs with mild to moderate inflammation and 21 with severe inflammation. Seven and 27 PGs presented with mild to moderate and severe inflammation, respectively (Table 1).

Table 1
Mean and standard deviation of types of collagen fibers and inflammatory cell density in periapical cysts and granulomas
![]()
2. Collagen fiber characteristics
Using the non-parametric Mann-Whitney U test, a higher mean number of thick collagen fibers was found in PCs, while thin collagen fibers predominated in PGs. A statistically significant difference was found for both thick and thin fibers (p = 0.00). The detailed analysis of collagen fibers is tabulated in Table 1.
Red birefringence predominated in both thick and thin collagen fibers in PCs. In contrast, in PGs, the thick collagen fibers were mostly yellow, while the thin collagen fibers were green. The mean number of thick and thin fibers with their polarization colors was also evaluated. The thick fibers in PGs appeared yellow (22.00 ± 11.01), while those in PCs were red (54.97 ± 14.01). The thin fibers in PGs emitted green birefringence (45.85 ± 21.94), while those in PCs emitted red r (36.68 ± 14.22) (Figure 2A-2F). A comparison of the mean number of collagen fibers according to polarization color in each group is presented in Table 2.

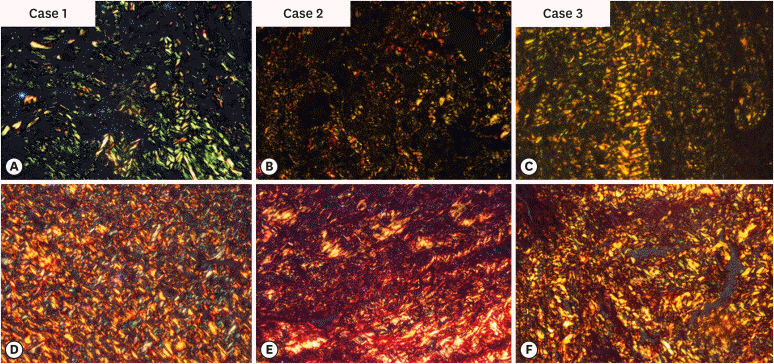 | Figure 2Photomicrographs of 3 cases showing predominant green birefringence of collagen fibers in periapical granulomas (A-C); case 1A shows predominantly green birefringence, case 2B depicts immature and thin fibers, and case 3C depicts greenish-yellow birefringence and immature fibers of a periapical granuloma. Predominantly red birefringence of collagen fibers in periapical cysts (D-F). Case 1D shows the ‘basket weave’ pattern associated with a periapical cyst, case 2E shows predominant orangish-red birefringence, and case 3F depicts the mature pattern formation associated with a periapical cyst. The sections were stained with picrosirius-red stain and analyzed under polarized light (×400).
|
Table 2
Mean, standard deviation, and comparison of thick and thin collagen fibers with polarization colors in periapical cysts and granulomas
![]()
Immunohistochemical analysis
1. Mean number of total mast cells
The immunohistochemical expression of tryptase in mast cells exhibited a cytoplasmic pattern, and immunoreactivity was observed in all cases of PCs and PGs (Figure 3A-3F). The mean number of mast cells in the center and periphery of connective tissue was higher in PGs. A statistically significant difference in the total number of mast cells was observed between PCs and PGs (p = 0.00) respectively. The intergroup differences were significant in both the central (p = 0.00) and peripheral (p = 0.01) areas (Table 3).

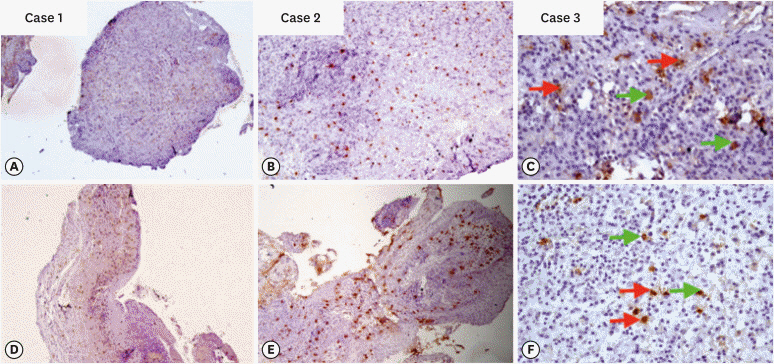 | Figure 3Photomicrographs of 3 cases of periapical granulomas (A-C); case 1A shows immunoexpression of tryptase positive mast cells (×40), case 2B depicts hot spots for the evaluation of mast cells (×100), and case 3C shows granulated (green arrow) and degranulated (red arrow) mast cells in fibro-cellular connective tissue stroma (×400). Photomicrographs (D-F) depicting 3 cases of periapical cysts; case 1D reveals immunoexpression of tryptase-positive mast cells (×40), case 2E shows hot spots for the evaluation of mast cells (×100), and case 3F depicts granulated (green arrow) and degranulated (red arrow) mast cells in fibro-cellular connective tissue stroma (×400).
|
Table 3
Comparison of mean mast cell density in the central and peripheral parts of connective tissue in periapical cysts and granulomas
| Groups | Mast cell density | ||
|---|---|---|---|
| Peripheral | Central | Total | |
| Periapical cysts | 23.88 ± 8.07 | 23.79 ± 7.71 | 47.67 ± 14.21 |
| Periapical granulomas | 29.74 ± 9.57 | 29.58 ± 9.52 | 59.32 ± 17.39 |
| p value* | 0.010 | 0.000† | 0.000† |
![]()
2. Degranulated versus granulated mast cells
The density of degranulated mast cells was higher in PCs than in PGs in the peripheral connective tissue stroma. In contrast, the number of granulated mast cells was higher in PGs in both the central and peripheral connective tissue (Table 4).

Table 4
Comparison of mean degranulated and granulated mast cells in the central and peripheral parts of connective tissue
![]()
Upon application of the Spearman correlation test for the associations of collagen fibers with mast cells and inflammatory cells, mast cells were significantly and inversely associated with total collagen fibers in PCs (r = −0.424, p = 0.013). Significant inverse correlations were also observed between thick fibers and inflammation as well as mast cells in PCs (r = −0.352, p = 0.041; r = −0.182, p = 0.032, respectively). Furthermore, degranulated mast cells in the central part of the connective tissue of PCs were inversely correlated with thick fibers in PCs (r = −0.35, p = 0.04). Thin fibers in PCs were not significantly correlated with any of the factors. No significant correlations were found in PGs.
Go to :
DISCUSSION
The findings of the current study regarding thick fiber birefringence of PCs, but not thin fibers, concurred with those reported by Hirshberg et al. [19]. The present study findings are in contrast with the results of Shetty et al. [20], who reported that the green-yellow color predominated in both thick and thin fibers of PCs. The slight predominance of the green-yellow color in radicular cysts in previous studies might be attributed to inflammation, which could affect the packing of collagen fibers.
The mean numbers of thick and thin fibers according to their polarization colors were also evaluated. Similar results have been reported in previous studies with respect to PCs [2122]. The findings of the present study, however, were discordant with those of other studies [82324]. This discrepancy could be attributed to differences in study designs.
In the present study, high inflammation (an inflammatory score of 3) was observed in 27 of 34 cases PGs and 21 of 34 PCs. A significant inverse association was observed between the number of thick fibers in PCs and inflammatory cell density (p = 0.04). It was also observed that inflammation deteriorated the original structure of collagen fibers, leading to their structural disorganization. Concordant results were observed by Vij et al. [10]. It was stated that inflammation could change the microenvironment of the extracellular matrix, which directly influences collagen synthesis and assembly. It was also postulated by previous authors that the proteoglycan content of collagen fibers changes at the time of maturation, leading to dehydration and an increase in the diameter of collagen fibers, and thereby causing an enhanced intensity of birefringence and change in the polarization color [101725]. Inflammatory cells play a dual role in periapical lesions by releasing various cytokines, lymphokines, and growth factors, which sometimes lead to the formation of thick, mature, orange to red, closely packed collagen bundles with an absence of intense collagenolytic activity. In contrast, increased collagenolytic activity could cause local destruction of collagen fibers, which then appear green to yellow under a polarized microscope.
When a mast cell becomes degranulated/activated, the secretory granules release tryptases along with other extracellular matrix mediators [13]. Mast cells are said to play a pivotal role in the pathogenesis and progression of periapical lesions, especially in PCs, leading to their expansion, resorption of bone, vasodilatation and angiogenesis, an inflammatory cell response, and increased content of cystic fluid [26].
The comparison of mast cell density revealed significantly higher counts in PGs than in PCs. This finding is consistent with previous studies conducted on PCs and PGs [31314]. However, this does not agree with other studies that reported higher number of mast cells in PCs than in PGs [27282930]. The difference may be due to previous studies’ use of toluidine blue histochemical staining, which is non-specific for mast cells and tends to yield false results.
In this study, the mean number of mast cells was correlated with the mean number of collagen fibers, and a significant inverse correlation was found in PCs (p = 0.013), whereas the association was non-significant in PGs. These findings indicate that the number of immature fibers and mast cells are directly associated. Activated mast cells release tryptase, which in turn activates fibroblasts, leading to the production of new loosely packed and immature collagen fibers. This study found that in the presence of inflammatory cells and an increased number of mast cells, the number of thin, immature, and loosely packed collagen fibers was greater, while thick, mature, and densely packed collagen fibers were infrequent.
A higher recurrence rate was observed with an increased size of the periapical lesions by Toskos et al. [31]. Thus, mast cells, which plays a role in the expansion of periapical lesions, may aid in the prediction of recurrence and prognosis. Moreover, a reciprocal correlation of inflammatory cells and healing, as well as recurrence, was reported by Thakur et al. [32]. Hence, the overall grade of inflammation could serve as a preliminary indicator for the detection of recurrence and healing of periapical lesions.
Go to :
CONCLUSIONS
The present study observed a significant role of the mean number of collagen fibers, their birefringence, and mast cell density in predicting the nature, pathogenesis, and biological behavior of periapical lesions. Future studies could validate these findings and further explore the characteristics of collagen fibers in periapical lesions using picrosirius red staining.
Go to :
 XML Download
XML Download