

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Reproduction of the dental structure and of its visual features is one of the greatest challenges in restorative dentistry. Therefore, the accurate selection of shades is mandatory for clinical success. Although visual shade selection can be as precious as the use of a spectrophotometer, it is subject to factors such as the observer's subjectivity and the quality of ambient light, in addition to considerable experience of the dentists [123].
The selection of restorative composite shades is problematic. Previous studies have reported that matching with shades of different materials was not accurate enough. Some shades produce more reliable matches than others [45]. Vitapan Classical shade guide (Vita Zahnfabrik, Bad Säckingen, Germany), one of the most widespread tools for shade selection, was initially developed for ceramic materials. Previous studies have shown differences between restorative composites and Vitapan Classical (Vita Zahnfabrik) shade guide [678]. Besides, the teeth on the Vitapan Classical shade guide (Vita Zahnfabrik) have different shades, thicknesses, and translucency according to cervical, middle, or incisal thirds. Other limitations of commercial shade guides include the material of which they are usually made — plastic, which is, at best, similar to the actual color of the restorative composites. Some guides do not allow overlapping the enamel color over the dentin color to simulate a more real clinical situation or predict the thickness of restorative composite to be used clinically [9]. Therefore, the final restoration outcome can be unpredictable sometimes [10].
To reduce color mismatches, many manufacturers have started to provide specific shade guides, but that is subjective and relies on dentists' skills and on lighting conditions. Portable spectrophotometers are considered objective, reliable, and accurate because ambient light does not influence the quality of spectral acquisitions [1112]. Shade information via the International Commission on Illumination (CIE)'s color notation system based on the L*, a*, b* axis is exported in numerical values related to visual shades, eliminating the influence of ambient light and the observer's subjectivity [131415].
Many studies compare different resins of the same shade to each other and compare various resins with shade guides. However, these studies usually use cylindrical-shaped specimens, utterly different from the shade guide and the clinical conditions. Considering the importance of the resin's surface shape and thickness at the time of shade selection, the present sought to reproduce the same conditions as the teeth of the Vita shade guide, avoiding distortions in the shade selection conditions. Therefore, considering the difficulties in shade selection through the use of visual guides, the aim of this study was: 1) to compare pairs of dentin shades on restorative composites with the reference shade on Vitapan Classical guide (Vita Zahnfabrik) using a portable spectrophotometer; 2) to compare the shade variation (ΔE) among the restorative composites from different manufacturers. The tested null hypothesis was that there would be no color variation between each shade and the reference on the shade guide, nor among the restorative composites from different manufacturers.
MATERIALS AND METHODS
Materials and specimens preparation
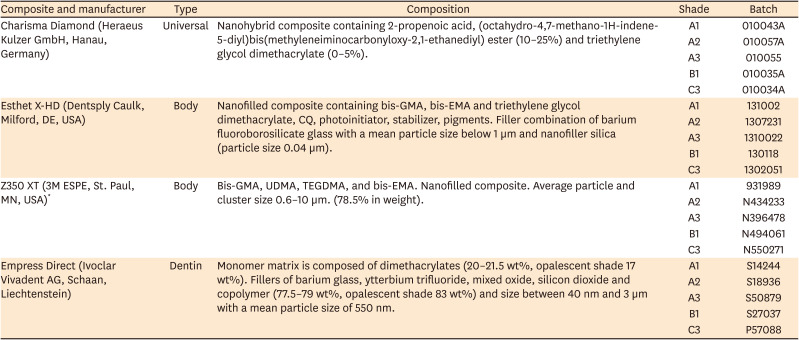
Five shades of 4 widely used restorative composites represented on Vitapan Classical shade guide (Vita Zahnfabrik) were selected. Data on the composites are shown in Table 1.
Table 1
Restorative composites and their characteristics
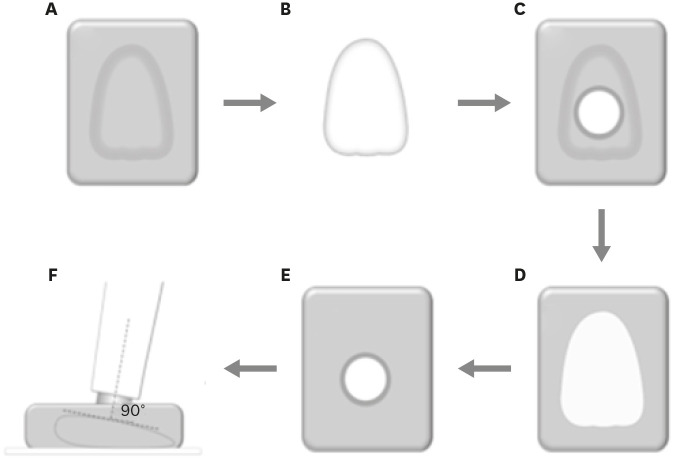
To standardize shape and thickness readings, polyvinyl siloxane molds (Express, 3M ESPE, St. Paul, MN, USA) were built and filled with 2 mm increments of each composite and light-cured for 20 seconds with a single-peak LED light source (Radii-Cal, SDI, Victoria, Australia) with 1,190 mW/cm2 irradiance, until the mold was filled up (n = 5). The specimens were stored in a lightproof environment for 24 hours. Details of the method are shown in Figure 1.
Figure 1
Illustration showing the experimental procedure. (A) Polyvinyl siloxane shade guide mold used to build the restorative composite specimens. (B) Restorative composite specimen reproducing shape and size of the shade guide pattern. (C) Back view of the polyvinyl siloxane positioning guide for standardization of the shade measurement with the spectrophotometer. (D) Restorative composite specimen seated on the positioning guide. (E) Front view of the positioning guide with the restorative composite specimen ready for the shade measurement. (F) Portable spectrophotometer positioned perpendicularly to the specimen to perform the shade measurement.
Shade measurement
Vitapan Classical (Vita Zahnfabrik), a new shade guide without previous use, was adopted as the standard for calculating color differences (ΔE*) in restorative composites. Prior to the measurement, the metallic stems were removed to avoid interferences on shade readings, and the back of the guide was gently worn to obtain a flat surface.
Three L*, a*, and b* values were measured according to the CIELAB color scale at the middle third for each tooth selected on the shade guide with an intraoral spectrophotometer (Vita Easyshade; Vita Zahnfabrik) on a white background. Three readings were performed for each coordinate, and the average was used to calculate the ΔE of composites. The composite specimens were measured following the same parameters described for the teeth on the shade guide.
After data collection, the final shade of specimens was determined, and so was the ΔE* between each shade of the guide. The corresponding shade of the restorative composite was calculated by the mathematical equation:
The values of ΔE ≥ 3.7 were considered clinically detectable as aforementioned. The ΔE values were separately compared for each shade using one-way analysis of variance and Tukey's post hoc test (α = 0.05).
RESULTS
All shades presented ΔE higher than 3.7, compared with the corresponding shade of the guide and were classified as clinically detectable. Most shades showed significant differences among the restorative composites, such as A3, B1, and C3, which were different for all manufacturers.
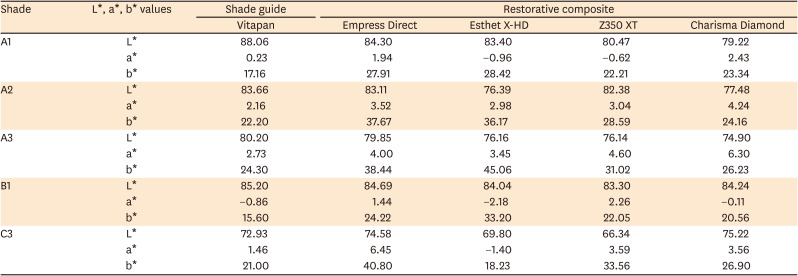
ΔE values for each shade and comparisons among the manufacturers are displayed in Table 2. Except for C3, all composite showed lower L* values (darker) than the Vita guide. For the shade C3, Esthet X-HD (Dentsply Caulk, Milford, DE, USA) and Z350 XT (3M ESPE) resins showed lower L* values (darker) than the Vita shade guide, while Empress Direct (Ivoclar Vivadent AG, Schaan, Liechtenstein) and Charisma Diamond (Heraeus Kulzer GmbH, Hanau, Germany) resins showed higher values (lighter) than the guide. A variable behavior was observed for the a* coordinate values, except for the shades A2 and A3 that all resin systems showed positive a* values (reddish). Regarding the b* coordinate, all resin systems showed positive values in all 5 evaluated shades, revealing that all composites tended to yellowish (Table 3).
Table 2
Means of ΔE followed by standard deviation
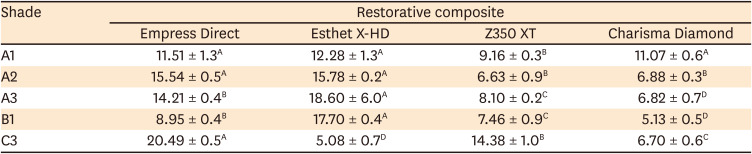
Table 3
The L*, a*, b* values of the composites
DISCUSSION
As shown in Table 2, considerable ΔE was found for each shade and its corresponding shade on the guide. Besides, the results also showed clinically unacceptable ΔE among the equivalent shades of the restorative composites for all manufacturers. Therefore, the null hypothesis was rejected.
The ΔE of shades of the restorative composites proved to be clinically unacceptable according to their corresponding shade on the guide. This helps to understand the difficulty in selecting shades accurately, as mentioned earlier [45]. In this study, the lowest ΔE value was recorded for Esthet X-HD shade C3 (5.08). Nevertheless, it is well above the clinically accepted limit (≥ 3.7), which would probably result in a shade restoration that is unacceptable to current aesthetic standards [416]. Interestingly, the largest ΔE was also recorded for a C3 color, for the Empress Direct composite (20.49). Compared with the shade guide, all shades presented different levels of variation depending on the manufacturer. Therefore, it was not possible to identify a more acceptable change, as previously described [517]. Previous studies have also reported large ΔE among restorative composites from different manufacturers, and this variation could change depending on the chosen guide, even for those from the same manufacturer [6131618]. The manufacture of a shade guide by dentists themselves using the composites available in the dental office could be a more precise alternative to commercial guides. However, this procedure is time-consuming and costly and would make it difficult to replace the material used in the office with that from another manufacturer because a new scale would need to be made. Another problem with this technique is that commercial restorative materials are continually being modified or replaced in the market, which would require changing or replacing the custom-made shade guide.
The significant difference among the ΔE of the equivalent shades from different manufacturers is also noteworthy, corroborating the findings of a previous investigation, in which the ΔE of A2, B2, and C2 shades from 5 restorative composite systems ranged between 1.7 and 13.3, depending on the analyzed shade, only 25% of the specimens were within clinically acceptable limits (ΔE < 3.7) [16]. Similar results were found in a previous study, in which shade A3 from 14 restorative systems presented ΔE between 3.25 and 14.04, as compared with the same shade guide used in the present study [13]. Considering the differences in the formulation of commercial composites, it is not easy to establish the reason for this variation (there might be multiple reasons, indeed). All components of the composite (e.g., photoinitiator, filler particles) can interfere with the optical properties of the restorative material, and even the monomer blend can probably interfere in the final shade of the composite, making the shade selection even more difficult [4519202122]. This can be even more problematic when the shade guide and composite manufacturers are not the same, as was the case with Vitapan, since this standard of shade may not match with the composite of several manufacturers, as occurred in the present study, in which shades A3, B1, and C3 presented significant differences for all manufacturers, corroborating the findings of a previous investigation [111723].
Although several studies have reported the same accuracy for visual shade selection and spectrophotometer, the use of the spectrophotometer could be a good alternative, since it would not be necessary to determine the hue and chroma visually, but to establish the values on the L*, a*, and b* axes and then select the composite with the closest parameters [12]. However, the dental structure is polychromatic, with different degrees of saturation, opacity, and translucency between the enamel and the dentin and between the different thirds of the tooth, thus making the clinical use of the spectrophotometer difficult. Besides, in an in vitro study, the background used for reading the sample does not vary, as occurs in clinical situations. Moreover, the modulation of the layers of enamel and dentin shades with different thicknesses can influence the aesthetic features of restorative composite restorations [92024]. The fact that the samples have the same thickness and shape as the shade guide pattern may have evidenced these differences since this makes it possible to standardize the optical behavior concerning the guide highlighting the characteristics of each composite. In this way, the sample shape's influence on shade measurements was minimized as much as possible. In contrast, variations in form and thickness can influence the optical behavior of the incident light rays when measuring. This modulation will influence properties such as translucency and opacity, helping to mimic the composite restoration and the tooth. Therefore, the professional's training and experience are essential factors in the color selection stage.
Despite the aforementioned difficulties, the initial color mismatch is not usually reported as a reason for restoration replacement [252627]. This probably occurs due to the great variations in lighting that affect the teeth during the day, the presence of saliva on the teeth, the distance while engaging in daily conversation, and the observer's subjective capacity that prevents perceiving color with the same precision as in a controlled environment. Some clinical strategies can minimize the mismatch between the prefabricated shade scales and the different shade systems available on the market: 1) Making custom guides with the composite resin itself, as mentioned earlier. 2) Use of clinical spectrophotometers for primary shade reference, as they cannot differentiate dentin and enamel shades, considering only the tooth's shade as a whole. 3) Use of commercial shade guides as an initial reference. After selection, confirmation must be made with small increments of the resin destined for each tooth portion. Carry out light curing, as composite resins generally change the shade after polymerization and recheck the shade, preferably with the reflector off.
CONCLUSIONS
Therefore, according to the findings of this study and despite its limitations, it was possible to conclude that:
None of the restorative composite shades of the investigated restorative systems showed a clinically acceptable difference in color compared with the shade guide. The equivalent shades of the tested restorative composites from different manufacturers may show clinically noticeable shade differences.
 XML Download
XML Download