

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Meningioma en plaque (MEP) is a benign tumor which usually grows with a spreading pattern or sheath-like appearance along the planes of the meninges and frequently occurs in the skull base such as the sphenoid bone of middle cranial fossa [123]. It has rarely been reported in other parts of the skull. Adjacent bony hyperostosis associated with MEP is more common than other types of meningioma [24]. We report a patient with a unique hyperostotic tumor that showed extensive hyperostotic changes on calvaria involving the sphenoid bone, peri-orbital bone, and other membranous bones.
CASE REPORT
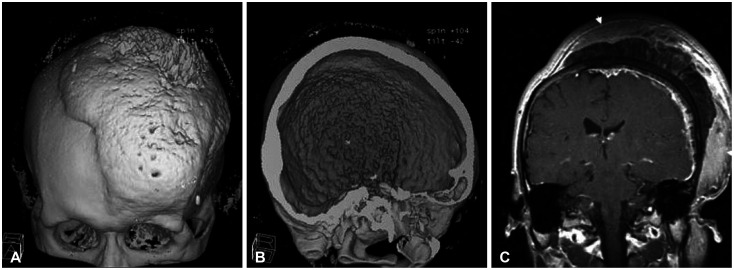
A 34-year-old man presented to our institution suffering from a slowly growing scalp mass based on the left fronto-parieto-temporal area with left exophthalmos. The mass was first detected by the patient 8 years ago. After exophthalmos aggravation, the patient decided to visit our clinic. Scalp swelling had progressively gotten worse for the previous 8 years. On ophthalmologic examination, visual acuity and visual field ranges were normal. The patient disclaimed of having any history of either head trauma or systemic disease. Preoperatively, the lesion was regarded to be a cranial hyperostotic bony lesion such as fibrous dysplasia, primary bony tumor, or diffuse calvarial meningioma (left dominant growing meningioma extracranially and intracranially). Laboratory and clinical findings showed no evidence of hyperthyroidism, gynecomastia, acromegaly, Cushing’s disease, and other metabolic hyperostotic diseases (Fig. 1).
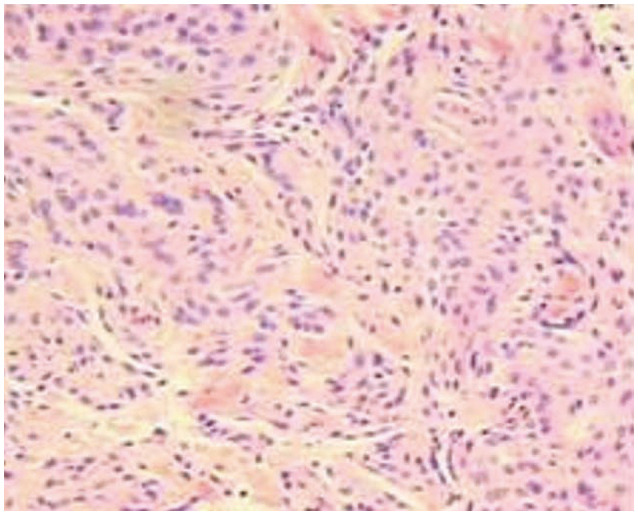
Surgical removal was planned. After bicoronal incision, the mass lesion was partially removed. The lesion was observed to extend from the pterional region to the zygoma level. Grossly, the tumor showed pinkish colored and jelly-like appearance under the skin. Hypertrophic calvarium on the parietal bossing had a moth-eaten appearance upon fragile bone removal with rongeur. The temporalis muscle showed hypertrophy. After removal of extracranial mass, bone wax and gelatin glue were used in the scattered small calvarial defect. We closed the operative field with plans for staged craniectomy with cranioplasty after pathologic confirmation. Pathologic findings showed a grossly dark brownish colored mass, with microscopic findings showing the bony tissue having tumor tissue consistent of meningothelial cells arranged in solids sheets with whirling around vessels. The lesion was diagnosed with meningioma. Soft tissue scalp biopsy also was observed to be meningioma. No tumor was found in the skin. We confirmed the tumor pathologically to be MEP with diffuse calvarial hyperostosis (Fig. 2).
A secondary operation was performed 6 months later. Pathologic diagnosis showed gray white to brownish soft tissue. In microscopic findings, bundles of meningothelial cells without significant atypia were observed. Also, focal new bone formation with bony sclerosis that disclosed portions of nodular tumor sections was detected. The patient later underwent radiotherapy. Follow-up brain CT images performed 6 months and 1 year after treatment showed no residual or recurring tumor.
DISCUSSION
Most MEP cases are still usually classified as WHO grade 1 tumors for their low proliferative index [5]. However, some anatomical locations, such as being in the close proximity of the orbit or cavernous sinus, create a higher chance for MEPs to become symptomatic. Therefore, surgical resection is the preferred initial treatment of choice [6]. Surgical outcomes of MEP were observed to vary in previous literature, as the possibility of gross total resection varies depending on the location and infiltration of the tumor [5]. Fariselli et al. [7] reported that if growth total resection was capable, the recurrence rate of MEP was similar to those of conventional Simpson grade. However, recurrence rates of MEP involving the orbit and cavernous sinus were shown to be significantly higher, with the 10-year recurrence rate being as high as 54% [89]. Management of recurred MEP includes re-surgery, radiotherapy, and gamma knife radiosurgery [10].
MEP usually occurs in the cranial base and is characterized more by its clinical and biological behavior than by histological appearance [3]. MEP is often associated with hyperostosis of the skull in the same area where the tumor grows [311] and is commonly located in the middle cranial fossa. Therefore, hyperostotic change of bone frequently occurs at the sphenoid wing but rarely in other sites such as the membranous bone of the cranial vault [1213]. In this case, hyperostosis of the cranium along the tumor showed massive bony growth crossing the sagittal suture as well as the sphenoid bone and peri-orbital bone. Akutsu et al. [12] reported a case that had shown diffuse hyperostotic bone by tumor invasion very similar to our case. This 34-year-old patient did not show a definite intradural tumor and had the characteristics of sclerotic type fibrous dysplasia that involved the orbital rim.
We were confused with the diagnosis between fibrous dysplasia and MEP plaque that involved the same area. Several authors suggested that the surface of hyperostosis tends to be smooth in fibrous dysplasia [1415]. Sclerotic type fibrous dysplasia has characteristics of overgrowth of sphenoidal bone and periorbital bone leading to optic foramen stenosis but has homogeneous thickening of the bone with a smooth bony surface. Regarding the imaging findings of our case, the bony growth pattern of the periosteal surface showed irregular and spiculated appearance on both sides of the cranial bone.
Although the exact mechanism of hyperostosis in meningioma remains unclear, tumor invasion of the bone is generally accepted among many hypotheses. As for hyperostotic change, several theories have been proposed; vascular disturbance of the bone that is caused by the tumor, irritation of the bone by the tumor without invasion, stimulation of the osteoblasts in the normal bone by the factors secreted by the tumor cells, production of bone by the tumor itself, and tumor invasion of the bone [1617]. Among four types of hyperostosis suggested by Kim et al. [16], our case demonstrated a three-layer pattern.
In conclusion, even if the tumor mimics fibrous dysplasia which has a diffuse massive hyperostotic tumor involving the sphenoid bone, periorbital bones, and membranous calvarial bones, we should keep in mind the possibility of MEP in case of an irregular bony surface.
 XML Download
XML Download