

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Duraplasty is a repair procedure that involves the patching of a dural defect with a graft to ensure dural closure [1]. This intervention aims to recreate the watertight seal between the subdural and epidural spaces through mechanical re-approximation of the defect margins. Compared to other types of dural substitutes, duraplasty is associated with lower rates of postoperative cerebrospinal fluid (CSF) leakage, which is a major source of morbidity and healthcare costs [23]. Complications of CSF leakage include infection, pseudomeningoceles, CSF fistulas, and intracranial hypotension syndrome [3]. However, outcomes vary based on graft material and technique [2]. The ideal dural substitute is malleable, cost-effective, readily available, nontoxic, nonimmunogenic, and unlikely to cause scarring [4]. Dural reconstruction may be accomplished with either synthetic grafts or biological grafts; the latter includes autographs, allografts, and xenografts [15]. Whether biological or synthetic products are used, the effects on operative time, cost, material composition, related complications, and availability must be taken into consideration. Unlike biological dural grafts, synthetic products lack a basement membrane, which may come at the cost of impaired graft adherence and keratinocyte differentiation [267]. However, there is still a lack of consensus regarding archetypal materials or techniques for best practice, and the choice of a dural substitute often depends on surgeon preference [1].
A continuous area of interest in the development of material for dural reconstruction is the collagen matrix [8]. Derived from collagen sponge, collagen matrix has shown to demonstrate wet strength and tissue integration, without induction of an inflammatory response or adhesions [489]. Acellular collagen matrix readily molds to the native brain and forms a watertight seal, eliminating the need for sutures [48]. With its optimized pore size and matrix structure, this material encourages fibroblast ingrowth and dural healing [4810]. Here, we describe our experience with 33 patients who underwent a duraplasty procedure using the novel DuraMatrix-Onlay® Plus (Stryker, Kalamazoo, MI, USA). The dural substitute is derived from a purified bovine Achilles tendon [11]. The matrix provides a scaffold for collagen synthesis and is intended for use without the need for dural sutures [4811]. We aim to address the knowledge gap regarding the optimal material for dural repair by reporting our findings on primary and secondary outcomes associated with the usage of DuraMatrix-Onlay® Plus for duraplasty.
MATERIAL AND METHODS
Study population
This is a retrospective case series of 33 patients who underwent a duraplasty procedure at a single academic hospital in Los Angeles, CA, USA between May 2016 and March 2017. In addition, we present a case illustration of a patient who required a multi-layer dural closure to achieve a watertight seal following a retrosigmoid craniotomy for the resection of a cerebellar lesion. The study was reviewed by the ethics committee and approved by the Institutional Review Board (IRB #21-001718).
Duraplasty procedure
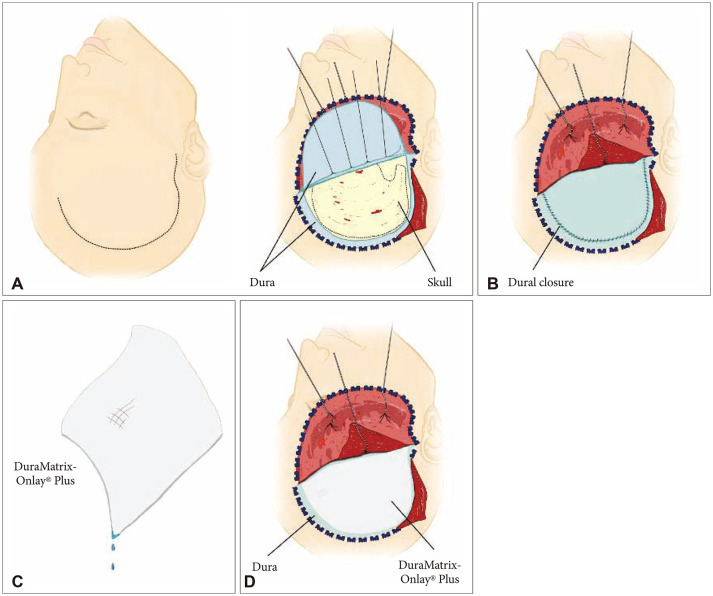
In brief, the duraplasty was performed in three steps: 1) the dura was loosely re-approximated whenever possible using running 4-0 Neurolon® (Ethicon, Somerville, NJ, USA) nylon sutures, 2) the material was chosen according to the size of the dural defect and was soaked in a solution of antibiotic and saline irrigation, and 3) the onlay was placed over the dural defect. Of note, multiple layers of the material can be used to cover the defect. In addition, dural sutures can be incorporated into surgical repair, depending on surgeon preference. DuraSeal® (Integra, Plainsboro, NJ, USA) can also be placed over the suture line to reinforce a watertight closure (Fig. 1).
Outcome measures
The primary outcome was the incidence rate of CSF leak, often detected by CSF escape through the dura and out the nose or ear. CSF leak can be diagnosed with a positive beta-2 transferrin test and identification of the possible site of the fistula on standard imaging sequences. Secondary outcomes included the rates of patient infection, dural substitute complication, and removal.
RESULTS
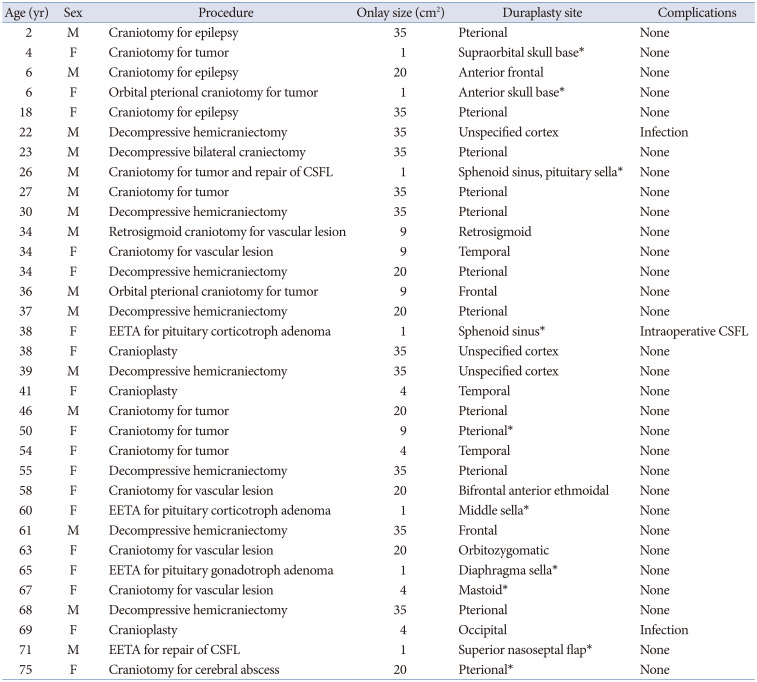
Thirty-three patients, 18 (54.5%) females and 15 (45.5%) males, underwent a duraplasty procedure using the DuraMatrix-Onlay® Plus material. The average age of the patients was 41.12±7.34 years (range 2–75 years). The majority of procedures were elective and for the resection of a lesion (n=19, 58%). The remaining procedures were for evacuation of intracranial hemorrhages (n=9, 27%), cranioplasty (n=3, 9%), or repair of a CSF leak (n=2, 6%). The average graft size used for dural repair was 17.69±4.73 cm2. The dural substitute was placed at the skull base in 10 cases (specifically at the right pterional lobe, anterior skull base, superior nasoseptal flap, supraorbital skull base, postauricular to the mastoid, in the middle sella, at the sphenoid sinus and pituitary sella, and in the cavity at the junction of the nasal floor mucosa and sphenoid sinus). The details of each procedure and cost of DuraMatrix-Onlay® Plus are summarized in Table 1 and Supplementary Table 1 (in the online-only Data Supplement), respectively. Of all the procedures, five watertight seal closures were obtained, three procedures resulted in no watertight closure, and 25 did not test the closure with Valsalva while in surgery. Seven patients had subgaleal or subdural drains placed, and three patients had epidural drains placed during the surgery.
There were no postoperative CSF leaks in our series. As previously mentioned, two patients underwent duraplasty to repair a primary CSF leak that was related to a prior intracranial procedure. The rates of infection, complication, and removal were 6%, 6%, and 3%, respectively. The two infected cases included a hemicraniectomy and a cranioplasty. Dural substitute complications included one case of an infected dural substitute and one case of an infected subdural collection. The infected dural substitute was removed from the former patient. In the case of the infected subdural collection, the patient’s CSF cultures showed the presence of Cutibacterium acnes, which was successfully treated with antibiotics. The infection resolved within days of beginning the antibiotics. The average follow-up duration was 3 months (0–10 months).
Case illustration
A 34-year-old male patient presented with progressive dizziness and vertigo. MRI was compatible with a right cerebellar cavernous hemangioma with evidence of several previous hemorrhages. The patient underwent a retrosigmoid craniotomy. The lesion was dissected away in its entirety, and running 4-0 Neurolon® nylon sutures were used for primary dura closure. The exposed mastoid air cells were waxed using bone wax. DuraSeal® was applied over the suture line to augment primary closure. DuraMatrix-Onlay® Plus was then placed over the suture line in two layers to fill the dura defect. The bone flap was placed over the dura onlay. The patient did not develop a CSF leak at the 4-month clinical follow-up, and there was no sign of dural substitute complication, infection, or removal.
DISCUSSION
Here, we report our experience with the DuraMatrix-Onlay® Plus collagen dura membrane in 33 duraplasty procedures in the setting of intracranial surgeries. The product is marketed as pliable, non-adherent to instruments, conformable, and repositionable [11]. Importantly, it has a top layer that is said to be resistant to CSF leaks [11]. While these features are advantageous, there is a paucity of literature concerning the clinical use of the DuraMatrix-Onlay® Plus membrane. Moreover, the product’s reported ability to prevent CSF leakage is based on pre-clinical and in vitro studies [11]. While the results of this study support the in vitro models, future randomized clinical studies with large numbers are warranted to support these findings.
The majority of procedures in the present study were elective and for resection of a mass, while the remaining procedures were either reconstructive or decompressive in nature. In our series, we did not observe any postoperative CSF leaks. Three patients underwent duraplasty procedures to repair CSF leaks associated with prior intracranial procedures, none of whom developed a leak after the procedure. In accordance with our findings, the available literature also suggests that duraplasty with collagen matrix is not associated with an increased risk of CSF leak compared to its dural substitute counterparts [48]. Although the results are encouraging, our study has low power and will need to be validated by a larger, multi-institutional study. In a large series of patients who underwent duraplasty using TissuDura® (Baxter, Deerfield, IL, USA), Esposito et al. [9] and Biroli et al. [12] reported only one patient who developed a CSF leak following an endoscopic endonasal transsphenoidal approach (EETA). The authors of the study also reported no local or systemic complications attributed to the equine-derived collagen biomatrix [912]. Those results were later confirmed in a 5-year observational follow-up study [13]. These qualities, along with the material’s weak immunogenicity, establish type I collagen as a particularly appealing dural substitute. There is added benefit for cases in which reoperation is anticipated, as collagen does not form adhesions to nearby neural tissues [91213].
While there are several materials available for dural repair, the literature does not support a definitively superior graft composition [11415]. Autologous grafts can be taken from the patient’s galea-pericranium, fascia latae, or temporalis fascia for dural repair. These grafts are inexpensive, nonimmunogenic, noninflammatory, and nontoxic dural substitutes that fuse with native dura to create a watertight seal [14]. However, autologous grafts are associated with longer operative times and surgical trauma, and may be limited by poor availability at the harvest site [914]. Allogenic materials, such as human dermis (AlloDermTM; LifeCell, Branchburg Township, NJ, USA) and dried human amniotic membrane, have also been used as dural substitutes. However, the relatively low availability of these materials has limited their operative use [16]. Xenografts (i.e., DuraMatrix®, DuraGen®, TissuDura®) are prepared from extracellular or collagen matrices of porcine, bovine, equine, and other animal sources [1416]. These grafts are routinely used as dural substitutes due to wide availability, ease of use, simulation of native dura development, and a low risk of short-term complications [1415]. Sutureless Xenografts provide the additional advantage of reduced surgical time compared with suturable dura substitutes. Danish et al. [17] found that duraplasty using non-suturable DuraGen® collagen matrix had significantly reduced operative times relative to AlloDermTM, an allogenic material requiring sutures for closure (92 minutes and 128 minutes, respectively). Unlike the biological dural substitutes, synthetic grafts (i.e., polytetrafluoroethylene) allow for the design of materials with ideal properties for dural replacement, such as safety, strength, elasticity, and resistance to traction [14]. Additionally, synthetics are inert, do not form adhesions to nearby neural tissues (a desirable quality in cases of expected resection), and are generally safe for prolonged use [1415]. In the selection of a dural substitute, the initial costs of the products should be taken into account [15], along with the potential costs that could result from complications and longer operation times [17]. Each dural substitute has its own benefits and limitations, and future large-scale, prospective studies are required to compare the efficacy, complications, and cost of the various dural repair materials, particularly the newer substitutes such as DuraMatrix-Onlay® Plus.
We performed duraplasty procedures in four EETAs (three for pituitary adenoma resection and one for repair of a primary CSF leak). None of those four patients developed a post-operative CSF leak or any other complication related to the use of DuraMatrix-Onlay® Plus. A nasoseptal flap was used in the patient undergoing repair of a prior CSF leak, and autologous fat grafts were placed in two of the three pituitary EETAs. The three pituitary tumor resections were performed through a non-extended endoscopic endonasal approach. Since the late 1960s, transsphenoidal surgery has been the standard approach to the suprasellar region for access to the pituitary [18]. However, EETA has significantly higher rates of CSF leakage [1819]. Thus, the identification of effective dural grafts and other methods of reducing CSF leaks is critical to the continued refinement of the transsphenoidal surgical approach [18].
Studies have shown that patients undergoing duraplasty following posterior fossa decompression demonstrate higher rates of CSF-related complications, but lower rates of reoperation compared to bony decompression alone [20]. Our consecutive series did not include patients who underwent Chiari decompression surgery, but several other dural substitutes have been investigated for such cases. Bowers et al. [21] compared the incidence of dural substitute-related complications across DuraGen®, DuraGuardTM, DurepairTM, and AlloDermTM materials in patients who underwent duraplasty following Chiari decompression. The authors concluded that the use of the human dermis allograft, AlloDermTM resulted in lower rates of pseudomeningocele formation and less need for reoperation when compared to the use of other products [21]. However, due to the limited power of studies like Bowers et al. [21], conclusions cannot yet be drawn about the relative performance of these graft materials among patients undergoing Chiari decompressions. Future studies should aim to address these disparities, as pseudomeningocele prevention is key for the improvement of clinical outcomes.
The postoperative infection rate following duraplasty with collagen matrix ranges from 2%–17%, with some variation according to the indication and site of placement [4810152223242526272829303132]. The postoperative infection rate of 6% in our series falls within an acceptable range and is comparable to rates of similar studies [4102631]. Nonetheless, taking measures to promote sterility when placing dural substitutes is critical. To lower the risk of infection in our study, the dural substitute was soaked in an antibiotic solution prior to implantation. The use of subgaleal drains may also lower the risk of infection [3334]. Sterile technique and the use of antibiotics are widely used in other graft implantations [35]. For example, the use of topical vancomycin in neurosurgical and spinal operations has been shown to significantly reduce surgical site infections, with minimal direct adverse effects or systemic toxicity [35]. While vancomycin-resistant bacterial strains exist and the preference among some surgeons to administer a second, postoperative dose of antibiotics has cultivated the development of antibiotic-resistant microbiota, vancomycin resistance typically occurs following co-infection, rather than a result of overuse of the antibiotic, itself [35].
These results suggest that the DuraMatrix-Onlay® Plus is a safe dural substitute that can be used to prevent CSF leaks in patients undergoing various cranial procedures. Our series describes a small, heterogeneous surgical patient population with limited follow-up duration, factors that should be considered when interpreting our results. Larger, multi-institutional prospective studies must be conducted to validate the complication rate associated with DuraMatrix-Onlay® Plus and to quantify its relative performance in duraplasty procedures.
In conclusion, our experience with DuraMatrix-Onlay® Plus demonstrated a low rate of postoperative CSF leak and dural substitute-related complications in a heterogenous group of neurosurgical patients requiring duraplasty. These results support the use of collagen matrices for dural closure in general neurosurgical procedures. However, further studies are needed to determine the safety and efficacy of this novel dural substitute.
 XML Download
XML Download