

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Previous prospective epidemiological studies have indicated an association between increased plasma homocysteine levels and elevated vascular risk factors, such as hypertension (HTN),1) diabetes mellitus (DM),2) coronary heart disease,3) and ischemic stroke,4) and all-cause5) and cardiovascular disease (CVD) morality. In a recent meta-analysis of observational studies,5) the high homocysteine level was associated with high mortality. However, since homocysteine levels are affected by folate intake6) and chronic disease states,7) such as cardiovascular and renal diseases, reverse causation or confounding variables may have affected the outcomes of these observational studies.
As a methyl donor, folate converts homocysteine to methionine, lowering blood homocysteine levels. In a meta-analysis of randomized controlled trials (RCTs) in which homocysteine levels were reduced using folic acid, the preventive effect of folic acid supplementation on premature death was not significant.8) However, there were insufficient follow-ups or heterogeneity in pre-existing conditions of the patients included in the RCTs. In addition, since these RCTs were conducted on patients, it is difficult to apply the results to the general population.
Mendelian randomization (MR) is a method that evaluates the causal effect of exposure on an outcome by using genetic variants as instrumental variables for modifiable exposure.9) This approach, conceptually similar to a RCT, is based on the principle that genetic variants are randomly allocated during gamete formation; consequently, these genetic variants are independent of confounding factors that bias observational studies. Therefore, genetic variants that influence homocysteine levels can be used to examine causality because they partially determine lifetime exposure to homocysteine. MR has been used previously to investigate the potential causal role of homocysteine in coronary artery disease10) and stroke6) using a single nucleotide polymorphism (SNP) in the gene encoding the enzyme 5,10-methylenetetrahydrofolate reductase (MTHFR) as an instrumental variable for predicting circulating homocysteine concentrations. This SNP, known as MTHFR C677T (rs1801133), consists of a cytosine to thymidine substitution at nucleotide 677 in MTHFR. This results in an alanine to valine substitution at amino acid 222 of the enzyme, which is detrimental to its activity and leads to an increase in blood homocysteine concentrations. In addition, large-scale GWAS reported that rs1801133 is the strongest genetic instruments of homocysteine levels.11)12) However, the association between homocysteine and mortality was not evaluated by MR in the general population.
The aim of this study was to assess the hypothesis that plasma homocysteine levels are causally associated with all-cause and CVD mortality in Korean adults by applying an MR study design.
Go to : 
METHODS
Ethical statement
This study was approved by the Institutional Review Board (IRB) of Chonnam National University Hospital (IRB No. I-2007-07-062), and informed consent was obtained from each subject.
Study population
This study was based on the Namwon Study, a prospective population-based cohort study conducted in Namwon, Republic of Korea. The framework of the Namwon Study has been described elsewhere.13) The Namwon Study involved 10,667 participants aged 45 years or older. A baseline survey was conducted from May 2007 to July 2010; MTHFR rs1801133 genotyping was missing for 572 participants, plasma homocysteine levels were missing for 82 participants, smoking history were missing for 47 participants, alcohol consumption were missing for 76 participants, body mass index (BMI) were missing for 52 participants, serum folate were missing for 235 participants, fasting serum glucose were missing for 58 participants, serum creatinine were missing for 58 participants, urine albumin-creatinine ratio (ACR) were missing for 108 participants, systolic and diastolic blood pressure were missing for 59 participants, medication history of HTN were missing for 54 participants, medication history of diabetes were missing for 55 participants, medical history of myocardial infarction were missing for 75 participants, and medical history of cerebral stroke were missing for 77 participants. Ultimately, 10,005 participants without missing values were included in the analyses.
Ascertainment of death
Causes and dates of death were obtained by linkage with National Statistical Office data. The dates of death were ascertained until December 31, 2020. Events were coded according to International Classification of Diseases, 10th Revision. Causes of death were categorized as CVD (codes I20–25 and I60–69), cancer (codes C00–C96), and others.
Methylenetetrahydrofolate reductase rs1801133 genotyping and measurement of plasma homocysteine
The MTHFR rs1801133 genotyping method and measurement of homocysteine has been reported previously.14) In brief, genomic DNA was extracted from peripheral blood using a QIAamp DNA Blood Mini Kit (QIAGEN, Valencia, CA, USA) according to the manufacturer’s protocol. Genotyping was performed by polymerase chain reaction–restriction fragment length polymorphism. Plasma homocysteine level was estimated with fluorescence polarization immunoassay using Abbott AxSYM analyzer (Abbott Laboratories, Abbott Park, IL, USA).
Covariates
Information on medical history, demographics, and lifestyle characteristics was collected using interviewer-administered standardized questionnaires. The smoking status categories were never smokers, ex-smokers, or current smokers. Alcohol consumption categories were nondrinkers, ex-drinkers, or current drinkers. Height was measured to the nearest 0.1 cm. Body weight was measured in light clothing without shoes. BMI was calculated as weight (kg) divided by height (m2). Blood pressure was measured on the right upper arm on 3 consecutive occasions at 1-minute intervals using a mercury sphygmomanometer (Baumanometer; WA Baum, Copiague, NY, USA) fitted with a cuff of the appropriate size. Blood pressure was measured when the subject was seated after having rested for at least 5 minutes. The means of 3 measurements were used in the analysis.
Venous blood samples were collected in the morning after 12 hours of fasting. Serum and plasma were separated on-site and stored at −70°C until the time of analysis. Serum folate level was estimated with ion capture assay using Abbott AxSYM analyzer (Abbott Laboratories). Serum fasting blood glucose levels were measured by enzymatic methods on an automated analyzer (Model 7600; Hitachi, Tokyo, Japan). Urinary albumin concentrations were measured using a turbidimetric immunoassay, and creatinine concentrations were measured by the Jaffe method on an automated analyzer (Hitachi-7600; Hitachi).
The estimated glomerular filtration rate (eGFR) was calculated using the 2021 Chronic Kidney Disease Epidemiology Collaboration creatinine equation.15) The ACR was defined as the urinary albumin value divided by the urinary creatinine concentration (mg/g).
HTN was defined as being on HTN medication, systolic blood pressure ≥140 mmHg, or diastolic blood pressure ≥90 mmHg. DM was defined as being on DM medication or having fasting serum glucose ≥126 mg/dL. Chronic kidney disease (CKD) was defined as eGFR <60 mL/min/1.73 m2. Microalbuminuria was defined as ACR ≥30 mg/g. The history of myocardial infarction and cerebral stroke was ascertained using a self-reported questionnaire. Given the low prevalence of myocardial infarction, it was redefined and included in the analysis as the combined prevalence of myocardial infarction or cerebral stroke.
Statistical analysis
The baseline characteristics of participants are presented as means ± standard deviations or numbers (%). To examine differences in variables across quartiles of plasma homocysteine, a trend test was performed.
In conventional multivariate analysis, multivariate Cox proportion hazard regression was used to evaluate the association between plasma homocysteine levels and all-cause and CVD mortality. In the first model, age, sex, and survey years were adjusted. In the second model, lifestyles (BMI, smoking history, and alcohol consumption) and socioeconomic status were additionally adjusted. In the third model, comorbidities (HTN, DM, CKD, microalbuminuria, myocardial infarction, and cerebral stroke) were additionally adjusted. In the fourth model, serum folate level was additionally adjusted.
MR using a 2-stage least squares regression was performed to evaluate the association between genetically predicted plasma homocysteine levels and mortality. In MR analysis, log2-transformed plasma homocysteine levels were used because the distribution of plasma homocysteine was right-skewed. Predicted plasma homocysteine levels of individual participants were only dependent on their MTHFR rs1801133 genotype. In the first stage, log2-transformed plasma homocysteine levels according to MTHFR rs1801133 genotypes were estimated in the model adjusted for age, sex, and survey years. In the second stage, we evaluated the association between genetically predicted plasma homocysteine levels and mortality in a multivariate Cox proportional hazard model adjusted for age, sex, and survey years.
Statistical significance was set at p<0.05. All analyses were performed using R (version 4.2.2; R Foundation, Vienna, Austria).
Go to :
RESULTS
Table 1 shows the baseline characteristics of the study population according to quartiles of plasma homocysteine. During a median of 14.9 years of follow-up, 1,693 (16.9%) participants died, 242 (2.4%) from CVD. Participants in the upper homocysteine quartile had a significantly lower serum folate level, shorter follow-up durations, higher rs1801133 T-allele frequencies, enrolled in the cohort later, were older, and were more likely to be men; they had lower BMIs, higher rates of smoking and drinking, and higher prevalences of HTN, DM, CKD, myocardial infarction, and cerebral stroke.
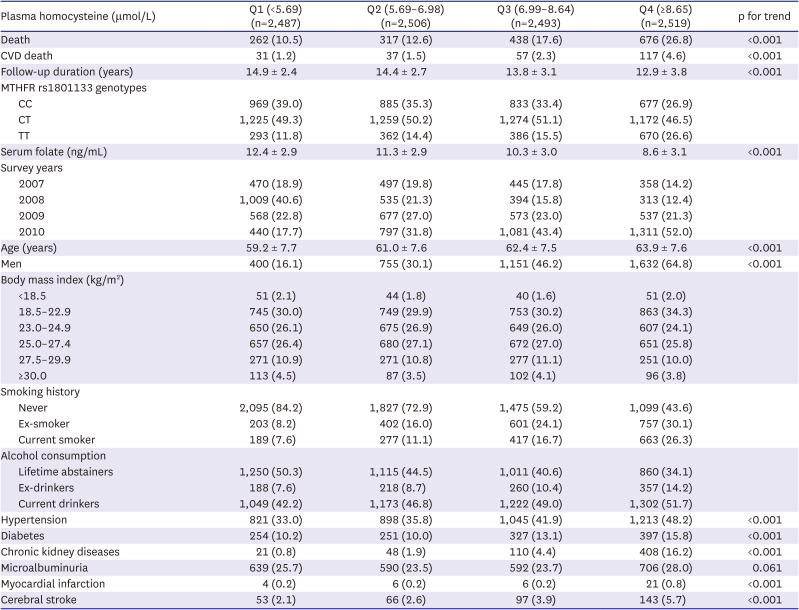
Table 1
Baseline characteristics of study population according to plasma homocysteine levels
All values are presented as means ± standard deviations or number (percentages).
CVD = cardiovascular disease; MTHFR = methylenetetrahydrofolate reductase.
![]()
Table 2 shows the hazard ratios (HRs) for all-cause and CVD mortality according to homocysteine quartile. HRs for plasma homocysteine were calculated using the first quartile as a reference. The HRs for all-cause mortality of the second, third, and fourth quartiles were attenuated as additional variables were added. When comparing the HRs in models 4 and 1, the HR of the second quartile changed from 0.96 (95% confidence interval [CI], 0.81–1.14) to 0.97 (95% CI, 0.82–1.14), the HR of the third quartile changed from 1.18 (95% CI, 1.00–1.38) to 1.16 (95% CI, 0.98–1.37), and the HR of the fourth quartile changed from 1.57 (95% CI, 1.33–1.84) to 1.33 (95% CI, 1.12–1.59). The strength of association was stronger for CVD mortality than all-cause mortality. In model 4, compared with the first quartile, HRs for CVD mortality of the second, third, and fourth quartiles were 0.98 (95% CI, 0.60–1.59), 1.31 (95% CI, 0.82–2.09), and 2.03 (95% CI, 1.26–3.26), respectively.
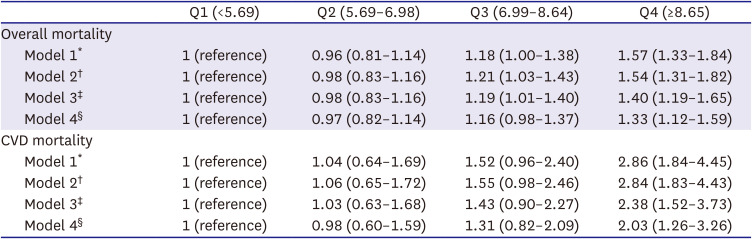
Table 2
Association between quartiles of plasma homocysteine levels and overall and cardiovascular mortality
*Age, sex, and survey years were adjusted.
†Smoking history, alcohol consumption, and body mass index were additionally adjusted.
‡Comorbidities (hypertension, diabetes, chronic renal diseases, microalbuminuria, myocardial infarction, and cerebral stroke) were additionally adjusted.
§Serum folate level was additionally adjusted.
![]()
Table 3 shows the association between log2-transformed plasma homocysteine and all-cause and CVD mortality in MR analysis and conventional multivariate analysis. In the first stage of MR analysis, the F statistic and R2 of MTHFR rs1801133 were 280.4 and 3.9%, respectively. Although the association between log-transformed homocysteine and mortality was positively associated in the conventional multivariate analysis, it was not significant in the MR study. In the conventional observational study, HRs of all-cause and CVD mortality for twice increment of plasma homocysteine were 1.40 (95% CI, 1.26–1.54) and 1.62 (95% CI, 1.28–2.06), respectively. In the MR study, those of all-cause and CVD mortality were 0.99 (95% CI, 0.62–1.57) and 1.76 (95% CI, 0.54–5.76), respectively.

Table 3
Results of MR and conventional multivariate analysis
| MR analysis* | Conventional multivariate analysis† | |
|---|---|---|
| All-cause mortality | 0.99 (0.62–1.57) | 1.40 (1.26–1.54) |
| CVD mortality | 1.76 (0.54–5.77) | 1.62 (1.28–2.06) |
Results are expressed per 2-fold increase in plasma homocysteine. All values are presented as hazard ratio (95% confidence interval).
CVD = cardiovascular disease; MR = Mendelian randomization.
*Age, sex, and survey years were adjusted.
†Age, sex, survey years, body mass index, smoking history, alcohol consumption, comorbidities (hypertension, diabetes, chronic kidney diseases, microalbuminuria, myocardial infarction, and cerebral stroke), and serum folate level were adjusted.
![]()
Go to :
DISCUSSION
Overall, our findings supported a positive association between homocysteine concentration and all-cause and CVD mortality in the conventional multivariate analysis. However, MR analysis did not provide evidence of a causal relationship between plasma homocysteine levels and all-cause mortality risk. These findings suggest that confounding variables may have influenced previous observational epidemiological associations.
The results of our conventional multivariate analysis were consistent with previous prospective studies. In the recent meta-analysis of previous prospective studies in the general population, HR for all-cause mortality was 1.34 (95% CI: 1.25–1.42) for each 5 µmol/L increase in homocysteine.5) However, there was significant heterogeneity among studies. This heterogeneity could be due to differences in fortification policies,6) patterns of folate intake,16) serum folate levels,17)18) or distributions of rs1801133 (MTHFR C677T)19)20) among study populations. Meanwhile, the preventive effect of reduced homocysteine on premature death has not been significant in RCTs. The meta-analysis study of Clarke et al.8) reported that folic acid supplementation has no statistically significant effect on premature all-cause, CVD, or cancer deaths.
The preventive effect of folic acid supplementation on disease differed by the combination therapy administered. In the meta-analysis of RCTs for patients with HTN and hyperhomocysteinemia,21) cardiovascular and cerebrovascular events were lower in the group receiving folic acid supplements and antihypertensive medication than in the group receiving antihypertensive medication alone. Also, Wald et al.22) reported that homocysteine reduction significantly increased the risk of ischemic heart disease in RCTs with a high prevalence of antiplatelet therapy. However, the effect of treatment based on the degree to which homocysteine was lowered was inconsistent. The preventive effect on stroke or CVD was higher in RCTs that achieved larger reductions in homocysteine levels.23) In contrast, in the RCT for the hypertensive population,24) although homocysteine levels decreased more in patients with MTHFR rs1801133 TT genotypes than in those in MTHFR rs1801133 CC/CT genotypes, the preventive effect of folic acid combination on stroke was significant in those with MTHFR rs1801133 CC/CT genotypes, but not in those with MTHFR rs1801133 TT genotypes.
To our knowledge, there have been no MR studies comparing homocysteine levels and mortality; however, many MR studies have evaluated the association between homocysteine levels and various disease and intermediate phenotypes. In 2-sample MR studies, the associations between homocysteine and blood pressure25) and homocysteine and fasting glucose26) were not significant. In addition, genetically increased homocysteine levels were not significantly associated with diabetes26) or coronary heart disease.11) However, in the MEGASTROKE consortium,12) genetically increased homocysteine was positively associated with small vessel stroke risk but not with risks of other subtypes of ischemic strokes, such as large artery and cardioembolic strokes. Because dietary folate intake levels16) or fortification policies6) differ according to population, further evaluation of the effect of gene–environment interactions on the association between homocysteine levels and disease is needed.
Our study has several strengths. This is the first MR analysis to examine the causal association of homocysteine and mortality in general population. In addition, the genetic instrument used in our study, MTHFR C677T, is strong (F statistic=280.4), indicating that weak instrumental biases are unlikely to affect the effect estimates. Furthermore, this MR study had sufficient statistical power to detect the association between homocysteine levels and all-cause mortality. Because there is no available tool to calculate power for survival outcomes in MR analysis, we took a conservative approach, treating survival as a binary outcome and using the methods described by Brion et al.27) With a total of 10,005 participants and 16.9% deaths, we have power >90% to detect an odds ratio (OR) of 1.50 for the association between homocysteine levels and all-cause mortality at a significance level of 0.05, assuming a 3.9% variance of homocysteine explained by MTHFR rs1801133. However, potential limitations of this study should be considered. First, our MR analyses of CVD mortality were underpowered. Statistical power was 61% to detect an OR of 1.75 for CVD death because the proportion of CVD death was only 2.4% in our study. Consequently, additional research is necessary to evaluate the association between homocysteine levels and specific CVD, as CVD mortality encompasses a range of health outcomes resulting from various cardiovascular conditions. Second, folate levels in a population may influence the association between homocysteine levels and disease.6) Koreans have higher folate levels than other population groups.28) Also, the folate levels of our cohort were higher than that of the general Korean population.14) Thus, relatively small differences in homocysteine levels between MTHFR C677T genotypes appeared in our study population with high folate concentrations, which may have attenuated the genetically predicted association between homocysteine and mortality.
In conclusion, homocysteine concentration is associated with all-cause and CVD mortality in conventional observational analysis. However, our MR analysis did not support a causal role for plasma homocysteine concentrations on premature deaths. These results suggest that the positive associations of homocysteine and mortality could be the result of confounding variables.
Go to :
 XML Download
XML Download