

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Coronary artery disease (CAD) is the leading cause of death worldwide.1) Effective prevention relies on early detection and management of risk factors such as high blood pressure, dyslipidemia, hyperglycemia, smoking, and obesity.2)3)4)5)6)7) Controlling these risk factors has been the basis for CAD prevention.8)9)10) Although the prognosis of CAD has improved with the development of many therapeutic drugs and diagnostic methods, CAD-related morbidity and mortality rates are still high.11) Furthermore, it is suggested that a significant number of patients without traditional risk factors suffer from CAD,12)13) stimulating interest in non-traditional risk factors as potential areas for enhancing CAD prognosis.
Interest in sex differences in CAD has grown, acknowledging that these differences play a critical role in cardiovascular health. Historically, studies largely focused on men, leaving a deficit of data on women’s clinical characteristics, prognosis, and treatment responses.14) Recently, developed Western nations have increased focus on women’s heart disease, implementing sex-specific treatment and reducing disparities.15) This has led to a significant decrease in CAD-related mortality among women in the United States (US).16) In 2011, the Women’s Heart Disease Research Working Group in Korea started the KoRean wOmen’S chest pain rEgistry (KoROSE) to study sex differences in CAD. This review explores the differences among Korean CAD patients by utilizing both domestic and international data, along with the findings from the KoROSE database.
Go to : 
KoRean wOmen'S chest pain rEgistry
The KoROSE was established in 2011 by the Women’s Heart Disease Research Working Group to study heart disease in women.17) With 32 Korean cardiovascular centers participating, the registry aimed to determine clinical characteristics and prognosis of women with CAD in Korea. Men were also included to identify sex differences. Among the patients who visited the outpatient department due to chest pain, those who required a coronary angiogram (CAG) for additional evaluation of angina pectoris were identified by the cardiologist and subsequently enrolled in the registry. Most patients underwent invasive CAG (ICA), but some were evaluated with computed tomography angiography. Patients with unstable vital signs, end-stage renal disease, chronic obstructive lung disease, and certain other conditions were excluded. Prior to ICA, patients usually underwent transthoracic echocardiography and noninvasive stress tests. Data collected included anthropometric information, reproductive factors, occupation, cardiovascular risk factors, current medications, physical activity, chest pain characteristics, and results of examinations. Information on mortality and various cardiovascular events during follow-ups was also gathered. As of March 2023, approximately 3,700 subjects have been registered in the KoROSE database, with ongoing enrollment.
Go to :
EPIDEMIOLOGY OF CARDIOVASCULAR DISEASE
Cardiovascular disease (CVD) is a major health concern globally, particularly for women. In 2019, there were an estimated 275 million cases of CVD in women globally, and CVD is responsible for nearly one-third of all female deaths globally, making it the leading cause of death for women.18) The global age-standardized CVD prevalence in women for 2019 was about 6,403 per 100,000.18) In the US, over 60 million women, or 44% of the female population, live with some form of heart disease.1) CVD-related deaths rose from 6.1 million in 1990 to 8.9 million in 2019.18) In Europe, CVD is responsible for over 4 million deaths annually, representing 45% of all deaths, with more women affected than men. Of these deaths, 2.2 million were women and 1.8 million were men, which equates to 49% and 40% of all deaths, respectively.19) In South Korea, CVD is the second and third leading cause of death, with heart disease having a mortality rate of 61.5 per 100,000 people, and cerebrovascular disease 44.0 per 100,000.19) In 2021, the mortality rate of CVD was 1.1 times higher in men than women.19) Interestingly, the mortality rate of ischemic heart disease was higher in men, while hypertensive disease and cerebrovascular disease rates were higher in women.19)
Collectively, although the epidemiology of CVD can vary depending on the region and population studied, CVD is a leading cause of death worldwide, and it affects both men and women. Previously, CVD was considered a disease that mainly affects men. However, recent data show an increase in the prevalence of CVD among women, and some studies have reported higher mortality and morbidity rates from CVD in women than in men.
Go to :
SEX DIFFERENCE IN CLINICAL CHARACTERISTICS OF CORONARY ARTERY DISEASE
Age
Age is the main risk factor for developing CAD.20)21) Generally, the prevalence of CAD is higher in men than in women. The age-adjusted prevalence of CAD in the US in 2018 was 7.4% for men and 4.1% for women.22) CAD prevalence rises with age in both sexes, but the increase is more pronounced in women.21) According to the American Heart Association, about 40% of men and women aged 40–59 develop CVD, and this proportion increases to 75% in individuals aged 60–79 and 86% in those over 80.21) Men typically develop CAD in their 40s or 50s, while women usually develop it after menopause, in their 60s or 70s. The prevalence of CVD among patients aged 70 years or older is similar to that of men or higher in women. Studies using Korean data have confirmed these trends. In a study analyzing ICA findings of 2,348 Korean patients from KoROES database, women were significantly older than men (64.4 vs. 59.5 years, p<0.001).23) Similarly, in a study analyzing 44,967 individuals who underwent percutaneous coronary intervention (PCI), women were older than men (71.1 vs. 62.9 years, p<0.001).24)
The increased cardiovascular risk in older women may be due to factors like lower estrogen levels, a higher prevalence of cardiovascular risk factors, and genetic predisposition.
Risk factors
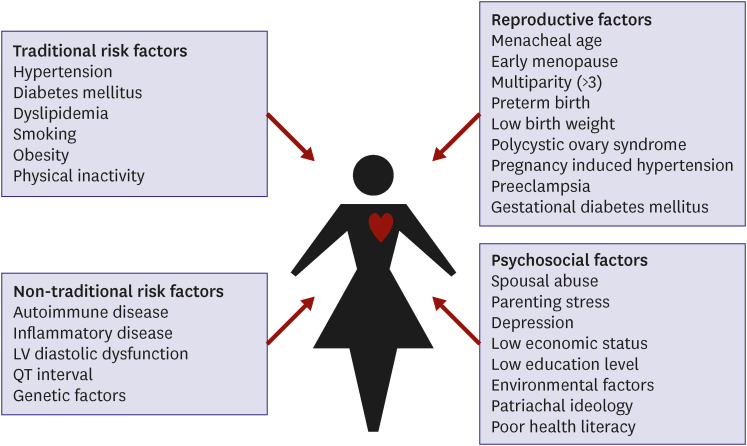
As the age of patients with CAD increases, the prevalence of cardiovascular risk factors also tends to increase. Therefore, it might be expected that women have more cardiovascular risk factors than men due to their older age. When looking at the prevalence of risk factors in CAD patients, it is notable that hypertension, diabetes and dyslipidemia are more common in women, while men tend to have higher rates of smoking and prior history of ischemic heart disease. This observation is consistent with both foreign and domestic data.23)24)25)26)27)28) Moving forward, we will provide a more detailed examination of the differences between men and women in terms of traditional and non-traditional risk factors.
Traditional risk factors
1) Hypertension
Hypertension is more prevalent in men under 65 years of age, whereas in women over 65 years of age, the prevalence is higher.29) In women, the increase in systolic blood pressure is more pronounced after menopause.30)31) This may be due to the loss of vasodilatory effect of endogenous estrogen, atherosclerosis, increased salt sensitivity, decreased endothelial nitric oxide production, and increased expression of angiotensin II receptors.30) As a result, the frequency of isolated systolic hypertension in women is higher than in men, which is a major risk factor for the development of cardiovascular complications. Several studies suggest that hypertension may have a stronger impact on CAD risk in women than in men, and may be associated with a higher prevalence of non-obstructive CAD and diffuse atherosclerosis in women.32) In a study of 1,254 patients with stable chest pain who had elective ICA in the suspicion of CAD from the KoROSE database, the prevalence of hypertension was similar between sexes (50.2% for men and 51.1% for women) but hypertension was one of risk factors for obstructive CAD only in women but not in men.33)
2) Diabetes mellitus
Sex differences in diabetes mellitus as a cardiovascular risk factor have been widely studied. For instance, a study comprising nondiabetic and type 2 diabetic subjects found that diabetes increased the risk for coronary heart disease more substantially in women than in men over a 13-year follow-up period.34) This was reinforced by a systematic review and meta-analysis showing that women with type 2 diabetes had a 46% higher risk of coronary heart disease mortality compared to men.35) Another comprehensive study found that diabetes roughly doubled the risk of occlusive vascular mortality in men and tripled the risk in women.36) Consistent with these findings, KoROSE data found that the presence of diabetes was an independent risk factor for obstructive CAD in women but not in men.33) These findings underline the need for more intensified management of cardiovascular risk in women with diabetes.
3) Dyslipidemia
Women tend to have higher levels of high-density lipoprotein (HDL) cholesterol, whereas, men tend to have higher levels of low-density lipoprotein (LDL) cholesterol.37)38)39) However, after menopause, women tend to have an increase in LDL cholesterol levels and a decrease in HDL cholesterol levels, which can increase their risk of CVD.40) The impact of dyslipidemia on CVD may differ between men and women, but the available data on sex differences in this regard is limited. It has been reported that the effect of low HDL cholesterol on cardiovascular risk is greater in women than in men.41) Additionally, a study of acute myocardial infarction demonstrated that the influence of lipoprotein (a) was more significant in women than in men in the young age group.37)
4) Cigarette smoking
Studies have consistently shown that smoking is a significant risk factor for CVD including CAD, stroke, and peripheral artery disease.6) Interestingly, women appear to be more susceptible to the detrimental effects of smoking, with female smokers showing a higher risk of developing CVD compared to their male counterparts, even after adjusting for other risk factors.42)43)44)45)46) In a prospective cohort study, female smokers had a relative risk of 2.24 for myocardial infarction, compared to 1.43 for male smokers.45) Similar findings were echoed in several meta-analyses.43)44) In a Korean study analyzing 12,565 patients with acute myocardial infarction, it was observed that the clinical outcomes were more unfavorable for women who are currently smoking, when compared to their male counterparts who are also smokers.46) Although a positive effect of smoking cessation on cardiovascular risk is observed in both men and women, the extent of sex differences remains inconsistent.47)48) The precise reason for this sex difference in smoking-related cardiovascular risk is unknown, but it underscores the urgency for smoking cessation education, particularly for women.
5) Obesity
The escalating global obesity epidemic, with its related complications, poses a significant threat to public health.49) Obesity is a significant risk factor for ischemic heart disease and stroke.4) In menopausal women, fat tends to accumulate in the abdominal area, similar to men, which heightens cardiovascular risk by inducing insulin resistance and inflammation.50) Abdominal obesity is well-known to increase cardiovascular risk by inducing insulin resistance and an inflammatory response.51) The KoROSE data showed that the association between abdominal obesity, as measured by waist circumference, and obstructive CAD in menopausal women was more pronounced than that measured by body mass index.52) Although obese men and women are at increased risk for CVD, a closure analysis of the data suggests that the relative risk of obesity is slightly higher in men than in women.4)53) However, most of this data uses body mass index as the measure of obesity, and further research using measures of abdominal obesity such as waist circumference or waist-to-hip ratio is needed.
Nontraditional risk factors
1) Chronic inflammation
Chronic inflammation is linked to an increased risk of CVD due to its destructive effects on blood vessels, such as promoting atherosclerosis, oxidative stress, and endothelial dysfunction.54)55) Inflammatory markers such as interleukin-6, tumor necrosis factor-alpha, and C-reactive protein (CRP) have been linked to an increased risk of CVD events such as heart attacks and strokes.54) Given that the prevalence of rheumatic diseases, which can cause chronic inflammation and increase cardiovascular risk,56) is higher in women than in men, it is essential to better understand this relationship when assessing cardiovascular risk, especially in women.57) The KoROSE data revealed that increased CRP levels predicted obstructive CAD in men, but not in women.58) This finding is consistent with other studies.59)60) While anti-inflammatory therapies have been used to reduce cardiovascular risk, their effectiveness remains uncertain.61)
2) Left ventricular diastolic dysfunction
Left ventricular (LV) diastolic dysfunction, identified as an independent predictor of poor cardiovascular outcomes,62) is associated with an increased risk of CAD.63)64) It results from myocardial ischemia, often caused by disturbed coronary blood flow,65) and shares risk factors with CAD.66) A study using KoROSE data found low septal e′ velocity to be an independent risk factor associated with obstructive CAD.67) Women are reported to be more susceptible to developing LV diastolic dysfunction in response to risk factors, although data on sex differences in its association with CAD is scarce.68)69)70)71) In a study with 1:1 matched samples from KoROSE data, the correlation between LV diastolic dysfunction and significant coronary artery stenosis was confirmed only in women.72) In another study that analyzed the KoROSE data, CRP was highly associated with CAD in men, while LV diastolic dysfunction was highly associated with CAD in women.58) Hence, more attention is warranted in evaluating CAD, especially in women with LV diastolic dysfunction.
3) Psychological stress
Psychological stress is one of the important risk factors for CVD.73)74)75) Chronic stress leads to increased release of stress hormones, such as cortisol and adrenaline, resulting in elevated blood pressure, heart rate, and inflammation. Over time, this response can damage blood vessel walls and contribute to the formation of blood clots and atherosclerotic plaques.74) Stressful condition can also induce lifestyle habits, such as overeating, excessive drinking, and smoking, which increase cardiovascular risk. Chronic job strain is associated with increased risk of recurrent coronary events.76) Stress impacts cardiovascular risk in both sexes, but the effect appears more pronounced in women.77)78)79) A study utilizing KoROSE data found a significant association between depression scores and obstructive CAD in women.80) However, some studies report inconsistent findings,81) highlighting the need for further research into the relationship between stress and cardiovascular health.
4) Pregnancy and reproductive factors
Pregnancy and reproductive factors may affect a woman’s cardiovascular risk.82) Studies suggest early or late menarche might increase CVD occurrence.83)84) A study using KoROSE data from 687 Korean women showed late menstrual age as an independent factor for significant coronary artery stenosis.85) Polycystic ovary syndrome, characterized by irregular menstrual cycles and hyperandrogenism, is linked with hypertension, dyslipidemia, and hyperglycemia, significantly escalating CVD incidence.86) Conditions such as hypertensive disorder of pregnancy87)88) and gestational diabetes89) are notable risk factors for later-life CVD development. Preterm birth and low birth weight also increase maternal cardiovascular risk, although the underlying reasons are unclear.88)90) A J-shaped correlation exists between the number of pregnancies and cardiovascular risk, with women experiencing over 5 pregnancies having higher rates of future cardiovascular events.91) In the analysis of KoROSE database, an increased number of pregnancies (odds ratio, 1.223, 95% confidence interval, 1.026–1.457, p=0.025, per pregnancy) were the independent predictors of obstructive CAD even after controlling for conventional risk factors.85) This connection could be due to repeated physical stress, metabolic abnormalities, and weight gain during pregnancies.92)
Clinical presentations
There are sex differences in the clinical presentation of CAD. Studies have shown that women may experience different types of chest pain compared to men, such as more dull or burning pain rather than the classic squeezing or pressure-like chest pain associated with CAD.93)94)95) Additionally, it has been reported that women with CAD were more likely to present with atypical symptoms such as fatigue, shortness of breath, and weakness, compared to men who are more likely to present with chest pain.93)94)95)96)97)98)99) Also, throat, jaw, shoulder and neck discomfort were more frequently reported by women than in men.94)95)97)99)100) The way chest pain is expressed, or the way language is used differs between men and women, and in particular, ambiguous expressions in women make diagnosis more difficult.101) KoROSE study investigating 1,549 patients found that men experienced more squeezing-type pain on the left side of the chest, while women demonstrated more dull quality pain in the retrosternal and epigastric area.93) Additionally, in the same study, palpitations and headaches were more frequently observed in women than in men as associated symptoms.
The sensation of chest pain is controlled by various complex factors. Although it is not fully understood why men and women exhibit different symptoms of myocardial ischemia, there are various suggested reasons, such as differences in coronary anatomy, sympathetic innervation, hemodynamic factors, and stress response thresholds. These complex factors may contribute to the observed differences in chest pain symptoms between men and women.102)
The first step for the accurate diagnosis of CAD depends on the proper recognition of chest pain.103) However, women often present with atypical symptoms, leading to potential delays or misdiagnosis of CAD. To address this challenge, it is essential for healthcare providers to acknowledge these sex differences in chest pain manifestations. By doing so, they can ensure accurate diagnosis and appropriate treatment for both men and women.
Go to :
SEX DIFFERENCES IN DIAGNOSTIC TESTS FOR CORONARY ARTERY DISEASE
Cardiac biomarkers
Cardiac biomarkers can vary between males and females.104) For example, troponin is a protein released into the bloodstream when there is heart muscle damage. Cardiac troponin is an important biomarker used to diagnose and manage CAD. Studies have demonstrated that women usually have lower levels of troponin than men.105) Similarly, B-type natriuretic peptide (BNP) or N-terminal proBNP (NT-proBNP) are hormones released by the heart when it’s under stress. BNP or NT-proBNP play an important role in the diagnosis, management, and monitoring of CAD, particularly in relation to heart failure and myocardial ischemia.106) Women tend to have higher levels of BNP than men in heart failure and CAD.25)107)108)
It’s critical to consider sex differences when interpreting cardiac biomarkers since these differences can have clinical implications for the diagnosis and treatment of heart disease. For instance, using the same cutoff values for troponin in men and women could result in underdiagnosis of heart disease in women due to their typically lower troponin levels.109)
Noninvasive tests
Noninvasive tests play a crucial role in identifying patients who may require further evaluation with ICA.110) Sex differences in the noninvasive test results for the diagnosis of CAD have been well documented. Women tend to have a higher incidence of false-positive electrocardiogram (ECG) results,111)112) potentially due to differences in heart size and shape and interference from breast tissue. Research has indicated important differences in various ECG parameters between men and women, such as faster heart rate and longer QTc duration in women.113) It has been suggested that the QTc interval can be an important variable in diagnosing CAD.114)115) KoROSE data from 1,741 patients with suspected angina showed that a longer QTc interval was associated with more severe CAD.115) Furthermore, the authors indicated that the diagnostic value of QTc interval was stronger in women than in men.
Women may be less likely to achieve target heart rates during exercise stress testing, which can lead to false-negative results.116) KoROSE data analyzing 335 women who underwent ICA demonstrated that treadmill exercise test (TET) had a lower sensitivity (16.7–42.9%) and positive predictive value (37.0–61.8%), but it has high positive predictive value (85.4–95.1%) in the detection of obstructive CAD.117)
Studies have shown that in echocardiography, women usually have smaller heart and thinner LV walls,118) and a higher incidence of diastolic dysfunction than men.58) LV diastolic dysfunction in women diagnosed by echocardiography has been found to be a valuable tool in diagnosing CAD. In a study analyzing 1,307 patients with suspected CAD from KoROSE database, low septal e′ velocity was identified as an independent risk factor associated with obstructive CAD, and significantly increased diagnostic value of TET in the detection of obstructive CAD.67)
Another study using KoROSE data found that CRP was the most powerful CAD risk factor in men, while low e′ velocity was the most powerful risk factor in women.58) In a 1:1 matching analysis of 295 men and women from KoROSE data, the association between LV diastolic function and obstructive CAD was observed only in women, suggesting that LV diastolic function in women is valuable for diagnosing CAD.72) Various studies have suggested that stress echocardiography provides valuable prognostic and diagnostic information in patients with CAD or suspected CAD.119) A multi-center registry analysis has suggested that exercise stress echocardiography could be more cost-effective than TET.120) Analysis using KoROSE data (n=202) showed that dobutamine-stress echocardiography was more useful in diagnosing obstructive CAD than TET in women.121) Additionally, an analysis of 102 women who underwent dobutamine-stress echocardiography revealed that obstruction of the LV outflow tract that occurred during the stress test was associated with LV hypertrophy, LV diastolic dysfunction, decreased exercise capacity and dyspnea, but not associated with coronary artery stenosis.122) This finding suggests that labor dyspnea or chest discomfort during exercise in women can be caused by obstruction of the LV outflow tract, even if it is not caused by coronary artery stenosis.122) Although diagnostic accuracy or prognostic value of stress echocardiography were similar between men and women in general, it is still recommended that exercise stress echocardiography should be used with caution in women due to insufficient data.123)
Overall, these sex differences in noninvasive test results can have significant implications for the diagnosis and management of CAD in women. It is important for healthcare providers to be aware of these differences and to tailor their diagnostic and treatment strategies accordingly. For example, women may require different exercise stress test protocols or imaging techniques to achieve accurate results. Furthermore, studies have suggested that sex-specific diagnostic criteria may be necessary to improve the accuracy of noninvasive tests for the diagnosis of CAD in women.
Invasive coronary angiogram findings
Numerous studies have examined sex differences in ICA findings, identifying several notable differences. For instance, women have been found to be less likely to have obstructive CAD on ICA when compared to men. Analysis of the KoROSE database found men had a higher prevalence of obstructive CAD and high-risk angiographic findings like left main disease or 3-vessel disease.23) This could be attributed to the fact that men usually have a higher prevalence of CAD risk factors such as smoking, hypertension, and high cholesterol.23) Further, men develop CAD at a younger age than women, allowing more time for disease progression.23)24) Estrogen, higher in women, protects the cardiovascular system, possibly contributing to differences in CAD prevalence.124) Lifestyle behaviors, such as diet and exercise, could also affect the earlier onset of CAD in men, as men typically have higher rates of physical inactivity and unhealthy eating habits.125)
The pathophysiology of CAD may also differ between men and women.32) Women tend to have a higher prevalence of microvascular disease, characterized by abnormalities in small heart-supplying blood vessels, which traditional diagnostic methods like ICA may not easily detect. Women with CAD often exhibit non-obstructive disease, characterized by the presence of plaque without significant narrowing or occlusion, likely due to higher prevalence of diffuse and non-calcified plaque. Furthermore, women with CAD often have more diffuse disease, indicating the presence of plaque in multiple coronary artery segments, which can make diagnosing and treating CAD in women more challenging.
Go to :
SEX DIFFERENCE IN CLINICAL OUTCOMES OF CORONARY ARTERY DISEASE
In-hospital outcomes
Many studies on in-hospital outcomes after PCI have been reported, but the results are inconsistent. While there is some evidence to suggest that women may have higher rates of in-hospital complications after PCI compared to men,24)28) but some studies have not observed this effect.126)127) For example, a Korean study24) found that women had 1.2 times higher rates of in-hospital composite events but not in-hospital mortality compared to men in multivariable analysis, while a Western study127) found no difference between sexes with respect to the composite efficacy endpoint in patients undergoing primary PCI due to ST-elevation myocardial infarction after adjusting for potential confounders. However, it is a relatively consistent finding that post-PCI bleeding complications are more common in women than in men.24)127) Further research is needed to fully understand the potential sex differences in outcomes in patients undergoing PCI.
Long-term outcomes
There is ongoing debate about whether sex differences exist in the long-term prognosis of patients with CAD. Several studies have explored this topic, providing varying findings. For instance, an analysis of 67,534 patients found worse long-term outcomes in women, especially among those undergoing PCI.128) A meta-analysis of over a million patients found males had significantly lower mortality rates at 1 and 2 years post-PCI.129) Women also displayed poorer clinical outcomes after PCI for left main disease130) and had higher rates of cardiovascular events post-coronary artery bypass grafting.131) However, contradictory results exist. A study involving 28,924 PCI patients showed women had a lower 5-year death risk than men.132) Similarly, a multicenter study with 23,604 patients indicated that although short-term or mid-term prognosis was worse for women, long-term prognosis was better.133) Other studies have reported no sex differences in long-term prognosis for CAD patients.134)135)136) Therefore, considering other variables, such as race, age, and risk factors, is crucial for understanding these differences. Further research is needed for comprehensive insight into the subject, with the results of the ongoing KoROSE study expected to add valuable data.
Go to :
PATHOPHYSIOLOGY OF SEX DIFFERENCES
Genetic factors
Sex-specific gene expressions play an important role explaining the sex differences observed in CAD. It has been suggested that women tend to accumulate more subcutaneous fat, while men tend to accumulate more visceral fat, and these patterns are mainly determined by genetic factors.137) In addition, renin-angiotensin system associated genes in males compared to females may contribute to increased cardiac fibrosis in males.138) Researchers have identified several sex-specific single nucleotide polymorphisms associated with CAD or CAD risk factors.139)140) Variants on the Y chromosome have also been associated with elevated blood pressure,141) and it has been found that a father’s blood pressure status can influence blood pressure in male offspring.142) In an experimental study, the administration of androgens to macrophages derived from healthy males resulted in increased expression of genes associated with atherosclerosis compared to females.143) Recently, there have been attempts to utilize these genetic factors for predicting the occurrence of CVD.144) While the genetic predispositions associated with CAD are complex and involve multiple intertwined genes, understanding the expression and impact of sex-specific genetic factors can provide valuable insights into CAD.
Body size
Women typically have a smaller body size than men, which can be associated, at least partially, with a higher incidence of side effects from cardiovascular medications145) and complications related to procedures, such as bleeding.24) Due to their shorter stature and faster wave reflection, women may experience increased augmentation pressure.146) However, the relationship between height and CVD is still a topic of debate,147) and further research is needed to reach a consensus.
Psychosocial factors
Sex differences in CAD can be influenced by various psychosocial factors. Different stress levels according to the traditional sex role expectations may contribute to the development of CAD or its associated risk factors. For example, men may face work-related stress and pressures of raising a family, while women may experience stress related to caregiving and household responsibilities. In addition, it is known that women react sensitively to stress arising from relationships with people, and men react sensitively to stress in the workplace. Anxiety or depression, which are more common in women than in men, can also contribute to increased cardiovascular risk in women. Several studies have reported such a link.79)80)148)149)
Hormonal factors
Estrogen, a primary female hormone, exhibits cardiovascular effects by promoting angiogenesis, inhibiting fibrosis, preserving endothelial cell function, and inhibiting reactive oxygen species and inflammatory responses.124) Additionally, as stated above, estrogen depletion can lead to abdominal obesity50) and elevated blood pressure30) in older women. Cardiovascular risk escalates rapidly in postmenopausal women, which is closely related to a decline in blood estrogen levels.150)
Pregnancy and reproductive factors
The effects of pregnancy and reproductive factors on CAD have already been previously detailed in the section on “nontraditional risk factors.”
Go to :
SEX DISPARITY
Delayed diagnosis or misdiagnosis of CAD is more common in women than in men.151)152) Truong et al.153) have reported that the improvement of cardiovascular outcome via intensive statin therapy in patients with acute coronary syndrome was comparable between men and women. In this study, the benefit of statins appeared to be numerically higher in women. However, in the actual clinical practice, several studies have noted that cardiovascular protective drugs, such as statins, aspirin and renin-angiotensin system blockers, are prescribed less frequently to women than to men.154)155)156) PCI and coronary artery bypass grafting were also found to be conducted less frequently in women.155)157) In clinical studies, it can be seen that the participation rate of women is much lower than that of men.14) This disparity in treatment eventually results in suboptimal control of risk factors and poor prognosis.158) Such sex disparity needs to be well acknowledged and corrected.
Go to :
FUTURE DIRECTIONS
As detailed above, women have more CAD risk factors to consider than men (Figure 1). Particularly in women, many risk factors are not widely recognized in clinical practice, underscoring the importance of awareness. Furthermore, acknowledging the presence of sex disparities in CAD is critical. In the US, a campaign titled “Go Red for Women” has significantly increased awareness of women’s heart disease,15) concurrently contributing to a substantial reduction in women’s cardiovascular risk.16) In contrast, awareness of female heart disease in Korea may be notably lower among both the general public and medical professionals. The Women’s Heart Disease Research Working Group recently conducted a telephone survey with 1,050 middle-aged or elderly Korean women and found that awareness of women’s heart disease was strikingly low.159) Therefore, it is imperative to undertake systematic and multifaceted efforts to boost awareness of women’s heart disease. Additionally, current guidelines for CAD worldwide may not adequately account for sex differences. It’s crucial to increase women’s participation in clinical research to gather robust data. Based on this data, guidelines should underscore the distinctions between sexes. Furthermore, there could be a need for separate guidelines for men and women.160) Sex disparity and solutions for overcoming it is displayed in Figure 2.

Go to :
CONCLUSIONS
There are significant sex differences in the clinical characteristics and risk factors for CAD (Table 1), which were also confirmed in the KoROSE data for Korean population. These differences between men and women, which play a crucial role in the onset of CAD, often appear to be insufficiently recognized in clinical practice. Specifically, factors related to pregnancy, childbirth, and socio-psychological aspects are frequently overlooked as significant contributors to the occurrence of CAD in women. Instead, a sex disparity persists, where women tend to receive less CVD treatment than men. Medical professionals must first understand these sex differences and incorporate them into their diagnostic and treatment approaches. Additionally, clinical researchers should encourage more female participation in clinical research to generate robust evidence specific to women. This approach could potentially lead to improved patient outcomes, enhance the quality of life, and even save lives. Furthermore, an accurate recognition of these sex differences can assist in developing sex-specific diagnostic and treatment guidelines for CAD.
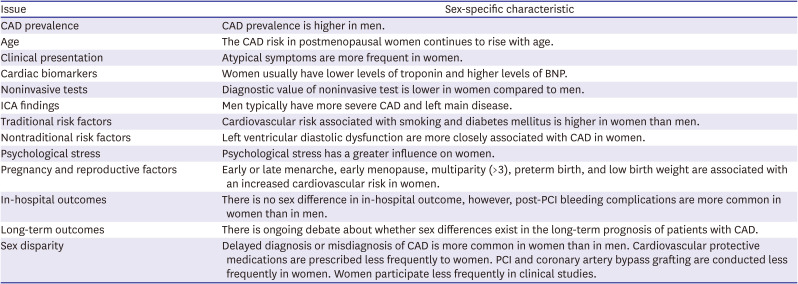
Table 1
Summary of major sex differences in CAD
BNP = B-type natriuretic peptide; CAD = coronary artery disease; ICA = invasive coronary angiography; PCI = percutaneous coronary intervention.
![]()
Go to :
 XML Download
XML Download