

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
ADVANCED HEART FAILURE
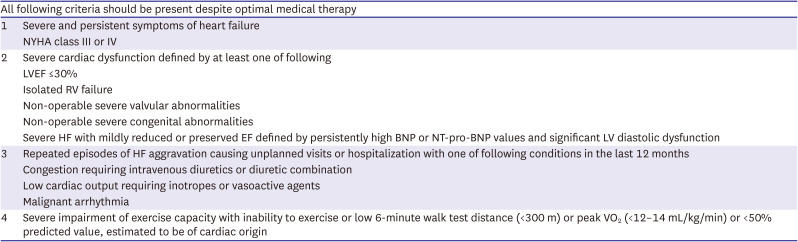
Definition
Table 1
European Society of Cardiology criteria defining stage of advanced HF
Classification
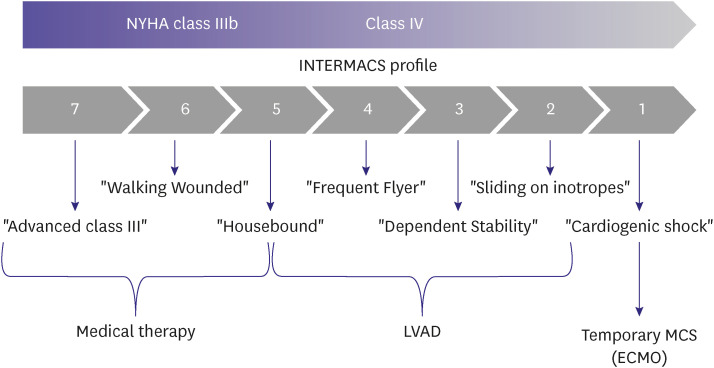
Table 2
Interagency for Mechanically Assisted Circulatory Support profiles
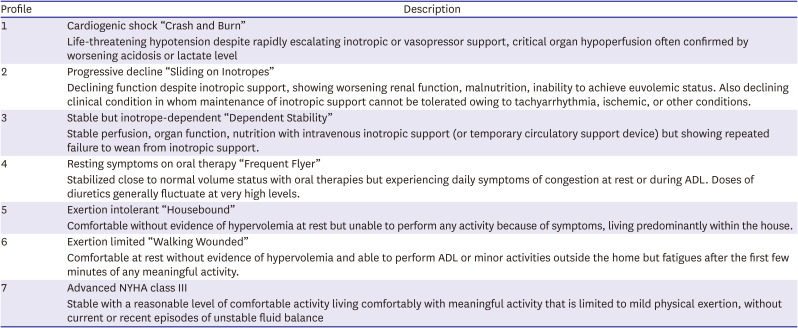
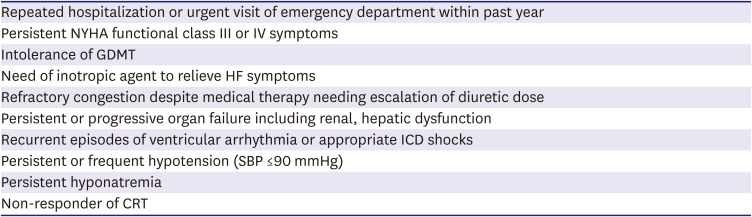
Table 3
Clinical criteria of referral for advanced HF
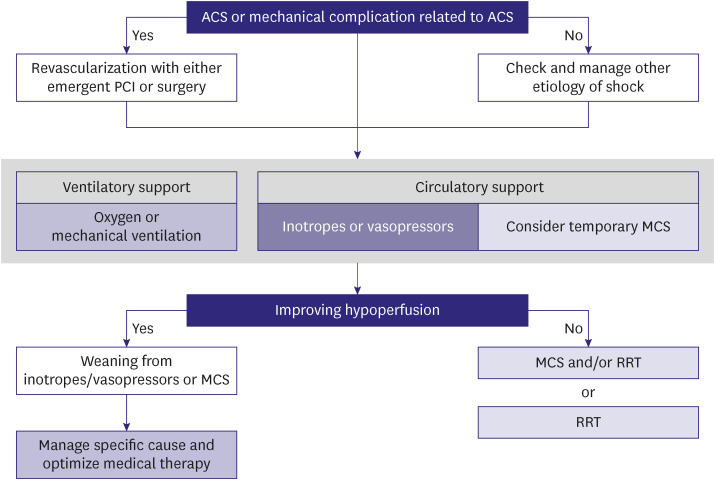
CARDIOGENIC SHOCK
1. For patients with cardiogenic shock, the Society for Cardiovascular Angiography and Interventions classification may be used to assess individual risk and predict prognosis. (Class IIb, Level of Evidence C)
2. Supplemental oxygen is recommended for patients with cardiogenic shock and hypoxemia. (Class I, Level of Evidence C)
3. Mechanical ventilation should be considered for patients with cardiogenic shock and persistent respiratory failure despite supplemental oxygen or non-invasive ventilation. (Class IIa, Level of Evidence C)
4. Adequate support with vasoactive agents may be considered for patients with cardiogenic shock to maintain end-organ perfusion. (Class IIb, Level of Evidence C)
Figure 1
Stages of cardiogenic shock. Adapted from Baran et al.9) with the permission of the Society for Cardiovascular Angiography & Interventions.

TEMPORARY CIRCULATORY SUPPORT DEVICES
1. Routine use of intraaortic balloon pump (IABP) is not recommended for cardiogenic shock. (Class III, Level of Evidence B)
2. Use of IABP can be considered for cardiogenic shock resulting from acute mitral regurgitation or ventricular septal defect. (Class IIa, Level of Evidence C)
3. Use of extracorporeal membrane oxygenation (ECMO) should be considered for cardiogenic shock refractory to medical therapy. (Class IIa, Level of Evidence C)
4. Extracorporeal cardiopulmonary resuscitation using ECMO is not recommended for patients with unwitnessed, out-of-hospital cardiac arrest, and signs of irreversible neurologic impairment. (Class III, Level of Evidence C)
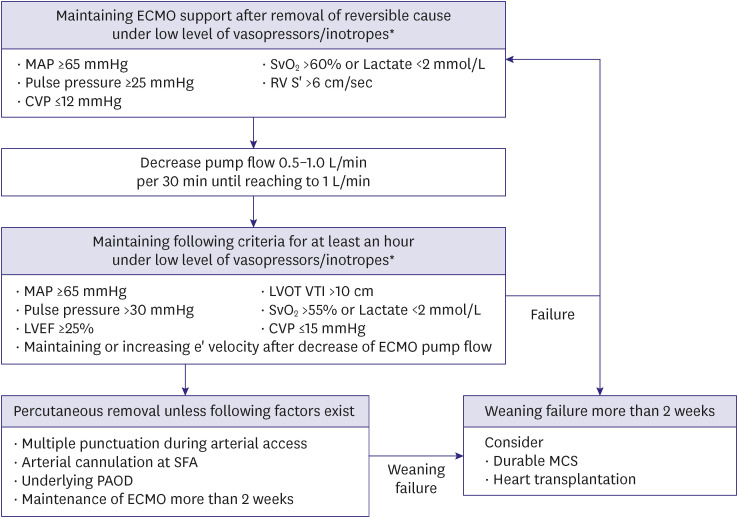
5. Evaluation of cardiac function recovery to determine adequacy for weaning from ECMO should be assessed by echocardiography, hemodynamic (e.g., central venous pressure, mean arterial blood pressure [BP]), and biochemical parameters (e.g., lactate). (Class IIa, Level of Evidence C)
Figure 3
Temporary circulatory support for drug-refractory cardiogenic shock.
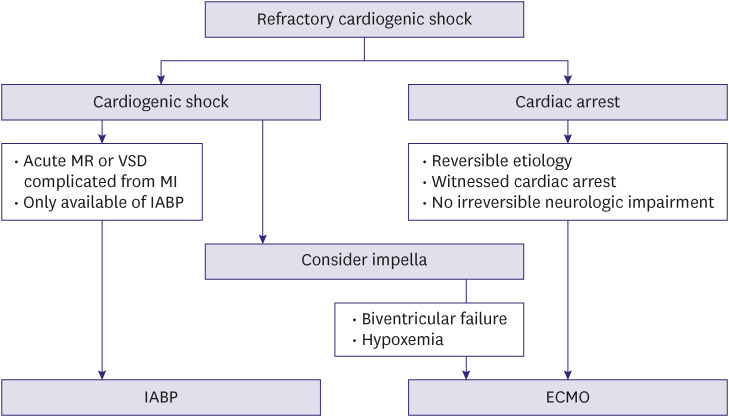
Figure 4
Weaning of percutaneous ECMO.
LEFT VENTRICULAR ASSIST DEVICE
HEART TRANSPLANTATION
1. HT is recommended to improve survival and quality of life for selected patients with advanced HF. (Class I, Level of Evidence C)
2. Cardiopulmonary exercise test is recommended in patients with advanced HF to guide HT listing. (Class I, Level of Evidence B)
3. Annual evaluation of right heart catheterization is recommended to evaluate hemodynamic status in patients listed for HT. (Class I, Level of Evidence C)
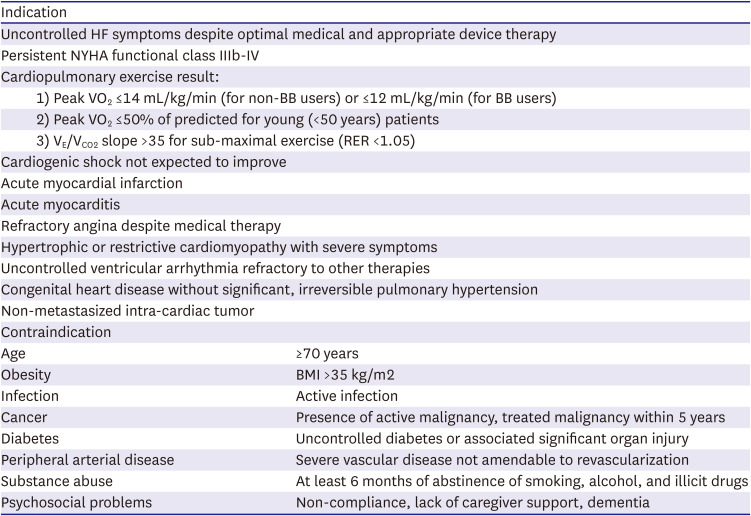
Table 4
Common indications and contraindications of heart transplantation
PALLIATIVE AND END-OF-LIFE CARE
1. Patients with advanced HF refractory to medical therapy and not indicated for HT or LVAD can benefit from palliative and end-of-life care. (Class IIa, Level of Evidence C)
2. Morphine, antiemetics, diuretics, and oxygen therapy may be considered for palliative care in patients with severe pain and congestive symptoms; GDMT, which lower BP without immediate effect, prescribed for long-term benefit may be continued at a reduced dose or discontinued. (Class IIb, Level of Evidence C)
3. Physician Orders for Life Sustaining Treatment may be prepared after multidisciplinary discussion and review. (Class IIa, Level of Evidence C)
ACUTE HEART FAILURE
Definition and aggravating factors
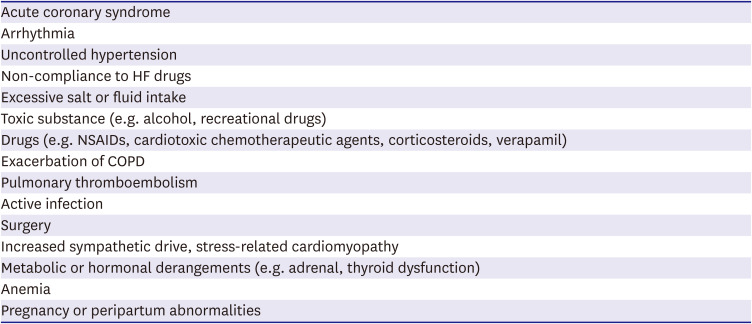
Table 5
Common aggravating factors of acute HF
Prognosis

Diagnosis
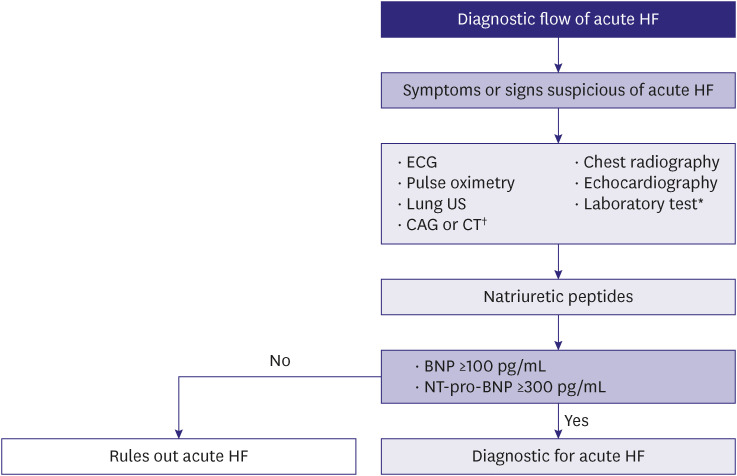
Figure 6
Diagnostic approach to suspected acute HF.
Classification
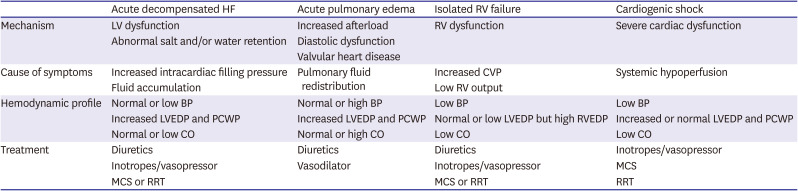
Table 7
Subtypes of acute HF
MONITORING ACUTE HEART FAILURE
1. Vital signs and oxygen saturation should be continuously monitored in patients with acute HF. (Class I, Level of Evidence C)
2. Volume status and fluid balance should be assessed by symptoms (orthopnea) and signs (jugular venous distention, peripheral edema, and body weight gain). (Class I, Level of Evidence C)
3. Renal function and serum electrolytes should be assessed frequently when initiating treatment with intravenous diuretics or renin-angiotensin-aldosterone system blockers. (Class I, Level of Evidence C)
4. Hemodynamic assessment using pulmonary artery catheter can be considered for refractory symptoms despite standard therapy with uncertainty of volume or perfusion status, low systolic BP, worsening renal function, and need for inotropes or MCS or HT. (Class IIa, Level of Evidence C)
5. Measurement of brain natriuretic peptide (BNP) or N-terminal pro-B-type natriuretic peptide (NT-pro-BNP) and/or cardiac troponin levels is recommended to predict prognosis and assess HF severity. (Class I, Level of Evidence A)
DIURETICS
1. Intravenous loop diuretics should be used to improve symptoms for all patients admitted for acute HF with symptoms or signs of volume overload. (Class I, Level of Evidence C)
2. The recommended initial doses of intravenous loop diuretics are 20–40 mg of furosemide for non-users of diuretics and an equivalent dose or more for those already on diuretics for acute exacerbation of pre-existing HF. (Class I, Level of Evidence B)
3. Measurement of urine sodium and urine output can be helpful to assess diuretic response. (Class IIa, Level of Evidence C)
4. Combination therapy of loop diuretics and thiazides can be considered for those with inadequate response to loop diuretics. (Class IIa, Level of Evidence C)
VASODILATORS AND OTHER DRUGS
1. Intravenous nitroglycerin or nitroprusside may be considered in patients with acute HF and systolic BP >110 mmHg to help improve symptoms and congestion. (Class IIb, Level of Evidence B)
2. Prophylactic anticoagulation therapy is recommended to prevent deep vein thrombosis and pulmonary thromboembolism in patients not on anticoagulants and where it is not contraindicated. (Class I, Level of Evidence A)
3. Routine use of opiates is not recommended to control symptoms except in selected patients with severe pain or anxiety. (Class III, Level of Evidence C)
Intravenous vasodilators
Venous thromboprophylaxis
Opiates
Digoxin
INOTROPES AND VASOPRESSORS
1. Inotropes may be considered to maintain systemic perfusion in patients with hypotension and evidence of end-organ hypoperfusion despite standard therapy and adequate fluid resuscitation. (Class IIb, Level of Evidence C)
2. Routine administration of inotropes is not recommended unless symptomatic hypotension and evidence of systemic hypoperfusion are observed. (Class III, Level of Evidence C)
3. Vasopressors may be used to maintain hemodynamics and end-organ perfusion for patients with cardiogenic shock. (Class IIb, Level of Evidence B)
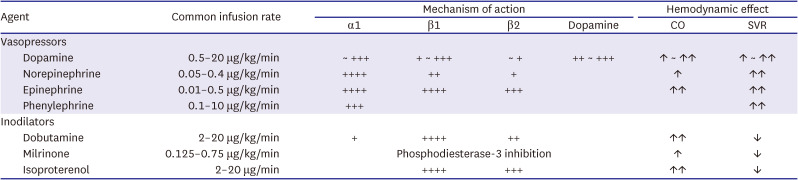
Table 8
Hemodynamic properties of common inotropes and vasopressors
Inotropes
Vasopressors
PRE- AND POST-DISCHARGE MANAGEMENT
1. Patients admitted for HF should be evaluated for the achievement of adequate decongestion before discharge. (Class I, Level of Evidence C)
2. GDMT should be initiated and preferably optimized before discharge. (Class I, Level of Evidence C)
3. Early follow-up evaluation within 1–2 weeks after discharge is recommended to assess volume status and drug tolerance. (Class I, Level of Evidence C)
 XML Download
XML Download