

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Hospital-acquired pneumonia (HAP) is a common cause of nosocomial infections and is associated with high morbidity and mortality rates. The high morbidity and mortality rates of HAP are due to comorbidities and multidrug-resistant (MDR) bacteria.12 Common causes of HAP are Staphylococcus aureus, Klebsiella pneumoniae, Pseudomonas aeruginosa, and Acinetobacter baumannii.3 The 2016 Infectious Diseases Society of America (IDSA)/American Thoracic Society (ATS) guidelines recommend the use of a single empiric agent against methicillin-sensitive S. aureus and P. aeruginosa. In patients with HAP who have a history of antibiotic use within 90 days or have a high risk of death, such as septic shock or the need for mechanical ventilation, and patients with ventilator-associated pneumonia (VAP) with acute respiratory distress syndrome, renal replacement therapy, septic shock, or a hospital stay of five days or more, combination therapy with two classes of anti-pseudomonal antibiotics is recommended, and if necessary, with coverage against methicillin-resistant S. aureus to increase the appropriateness of initial empiric antibiotics and reduce the mortality rate.4
However, the IDSA/ATS guideline expert panel recommended empiric dual anti-pseudomonal combination therapy targeting MDR gram-negative bacteria, despite the insufficient evidence of survival benefit of combination therapy; this is because the analyzed studies excluded patients with MDR pathogen colonization or severe comorbidities.4 The proportion of MDR pathogens identified in the recent Korean multicenter HAP/VAP cohort study was high (70.4%). Combination therapy was administered in nearly half (47.3%) of the patients, and the most frequently used drugs were piperacillin/tazobactam (59.3%) and respiratory fluoroquinolones (32.1%). Perhaps because of their nephrotoxicity, aminoglycosides were much less used (2.5%) as secondary combination agents than fluoroquinolones in the cohort.5
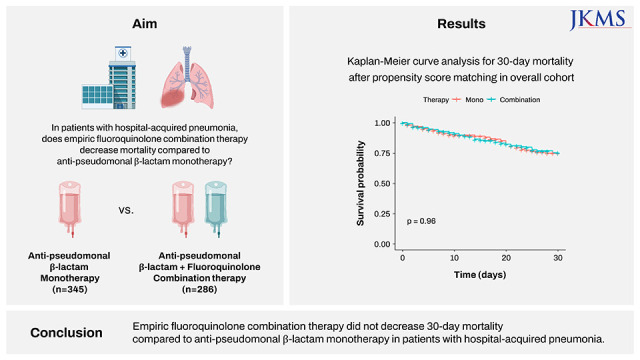
Fluoroquinolones are generally not nephrotoxic and are commonly prescribed for various infectious diseases in outpatient, general ward, and intensive care unit (ICU) settings. Therefore, resistance to fluoroquinolones is expected to be substantial among MDR pathogens. Many clinicians choose fluoroquinolone combination therapies for patients with one of risk factors following the IDSA/ATS guidelines. However, it is unknown whether combination therapy with fluoroquinolones improves the appropriateness of initial empiric antibiotics and survival rates, as the degree of MDR has become more severe in recent years. Thus, we investigated whether anti-pseudomonal non-carbapenem β-lactam plus fluoroquinolone combination therapy reduces mortality compared with β-lactam monotherapy in a Korean multicenter cohort.
METHODS
Study design and patients
This multicenter, retrospective, observational cohort study was conducted by the Korean HAP/VAP Study Group.5 This study was an extended cohort of the primary study. Between January 1 to December 31, 2019, data on eligible patients were collected from 16 tertiary and general hospitals in Korea. Adult patients (≥ 19 years) hospitalized for at least three days who had never received antibiotics for > 72 hours before hospitalization and those who had pneumonia-related International Classification of Diseases-10 code (J13–J18, J85) at discharge were recruited. Based on the 2016 IDSA/ATS guidelines,4 HAP/VAP is defined as a new lung infiltrate with clinical evidence related to infection, such as a new onset of fever, purulent sputum, leukocytosis, and decline in oxygenation after 48 hours of admission or mechanical ventilation. We included patients with HAP/VAP who received empiric anti-pseudomonal non-carbapenem β-lactam therapy (piperacillin/tazobactam or cefepime). We excluded the following patients: 1) those who did not have one of the risk factors requiring combination therapy, such as prior antibiotic use within 90 days, septic shock, mechanical ventilation, or late-onset HAP (≥ 5 days); 2) those who received empiric antibiotics other than piperacillin/tazobactam or cefepime; 3) those who received empiric piperacillin/tazobactam or cefepime, but concurrently with carbapenem, aminoglycoside, or colistin; and 4) patients transferred to a step-up center. Finally, we divided the enrolled patients into β-lactam monotherapy and fluoroquinolone combination therapy groups.
Data collection
Electronic medical records were carefully reviewed by trained study coordinators at each center. Through a comprehensive review, the following information were collected: 1) demographic data, such as age, sex, and body mass index; 2) clinical data, including comorbidities, Charlson comorbidity index, clinical frailty scale, prior antibiotic use within 90 days, late-onset HAP (≥ 5 days), location of diagnosis (general ward vs. ICU), risk of aspiration, artificial airway, VAP, classification of infection (microbiologically documented vs. clinically documented), Sequential Organ Failure Assessment (SOFA) score, and septic shock; 3) microscopically documented pathogens and MDR organisms; 4) data related to treatment, including empiric antibiotics, appropriateness of initial empiric antibiotics, adjunctive steroid use, mechanical ventilation, renal replacement therapy; and 5) clinical outcome data, including 30-day, 90-day, and hospital mortality, the interval between initiation of antibiotics and discharge, ICU admission, ICU length of stay, clinical responses, and discharge destination. Further details of the study protocol were described in a previous epidemiologic study.5
Definitions
Primary outcome was 30-day mortality. Pneumonia in patients with an artificial airway in the ICU was considered as VAP. Based on the third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3), septic shock was defined as patients with sepsis (SOFA score ≥ 2 points) requiring vasopressors due to persisting hypotension and having a serum lactate level > 2 mmol/L.6 The risk of aspiration was defined as having at least one among impaired swallowing, impaired consciousness, an increased chance of gastric contents reaching the lungs, or an impaired cough reflex.7 Except for colonizers or contaminants, microorganisms collected within two days of antimicrobials were considered cultured pathogens. Multi-drug resistant pathogens are defined as microorganisms resistant to agents of three or more antimicrobial categories.8 Initial empiric treatment was defined as an initially administered antimicrobial agent in the absence of microbiological isolates. Based on the drug susceptibility test results, inappropriateness was considered when the confirmed pathogens were resistant to the antibiotics used initially for empiric therapy.9 Clinical responses were divided as follows: clinical cure (an improvement in all pneumonia symptoms and signs) versus clinical failure (the persistence or worsening of symptoms or signs of pneumonia) or recurrence (the occurrence of new pneumonia three days after antibiotic discontinuation).5
Statistical analysis
The Pearson’s χ2 test was used to compare categorical variables, and the Student’s t-test was used to compare continuous variables. Propensity score matching (PSM) was performed to mitigate confounders between the monotherapy and combination therapy groups. Propensity scores were matched at a ratio of 1:1 (using the nearest neighbor matching algorithm with a caliper of 0.2) based on significantly different variables (chronic neurological disease, Clinical Frailty Scale, classification of infection, prior antibiotic use within 90 days, late-onset HAP, VAP, and combination with glycopeptide). The McNemar’s χ2 test was used for categorical variables, and a paired t-test was used for continuous variables for paired data after the PSM. Subgroup analyses were performed for patients with microbiologically and clinically documented infections. Before and after the PSM, a Kaplan–Meier analysis was performed for 30-day survival. Kaplan-Meier curves between monotherapy and combination therapy were compared using the log-rank test. Cox proportional hazards regression analysis was used to determine the effect of the combination therapy on 30-day mortality after adjusting for confounding variables. All statistical analyses were performed using Statistical Package for the Social Sciences (SPSS) software (version 26; IBM Corp., Armonk, NY, USA). All P values of less than 0.05 were considered statistically significant.
Ethics statement
This study was approved by the Institutional Review Board (IRB) of Soonchunhyang University Bucheon Hospital (approval No. 2020-03-037-003) and the local IRB of all other participating centers. The requirement for informed consent was waived due to the observational nature of the study.
RESULTS
Patient characteristics
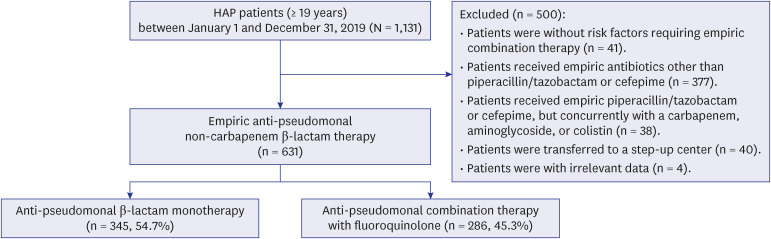
Electronic medical data of 1,131 adult patients with HAP were analyzed (Fig. 1). After excluding 500 patients based on the above exclusion criteria, 631 patients who received either piperacillin/tazobactam or cefepime as the sole β-lactam agent were enrolled. Of the 631 patients, 345 (54.7%) received empiric β-lactam monotherapy, and 286 (45.3%) received empiric β-lactam plus fluoroquinolone combination therapy.
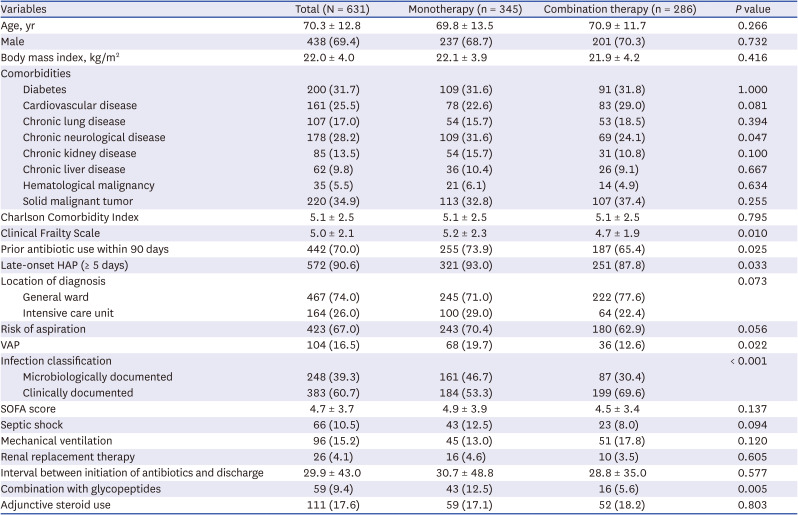
The mean age was 70.3 years (standard deviation [SD], 12.8), which was similar in both groups (69.8 vs. 70.9 years, P = 0.266) (Table 1). Sex, body mass index, and Charlson Comorbidity Index scores were comparable between the groups. The severity of HAP in both groups was comparable, with a mean SOFA score of 4.7 (SD, 3.7), which was similar in the two groups (4.9 vs. 4.5, P = 0.137, respectively). The proportions of patients with septic shock, mechanical ventilation, and renal replacement therapy were comparable between the groups. However, the proportions of patients with chronic neurological disease, microscopically documented patients, prior antibiotic use within 90 days, late-onset HAP, VAP, combination with glycopeptide, and clinical frailty scale scores were higher in the monotherapy group than those in the combination therapy group.
Table 1
Baseline characteristics of HAP patients in the overall cohort
Microscopically documented pathogens
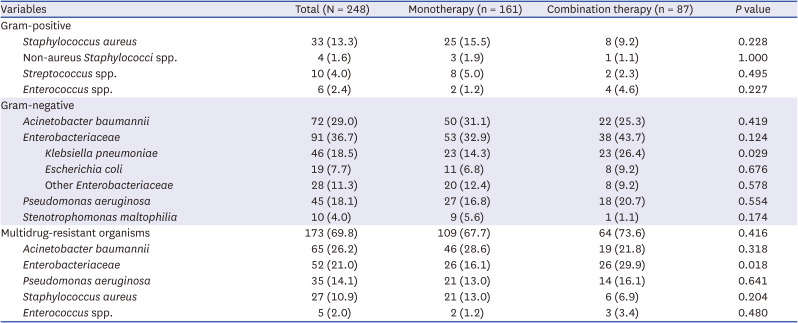
There were 248 (39.3%) patients who had microscopically documented pathogens (Table 2). The most common gram-positive pathogen was S. aureus (13.3%). The three most common gram-negative bacteria were A. baumannii (29.0%), K. pneumoniae (18.5%), and P. aeruginosa (18.1%). The proportion of MDR pathogens was 69.8% (173/248) among the microscopically documented patients. Methicillin resistance was detected in 81.8% of S. aureus (27/33) infected individuals. The MDR rates for A. baumannii, Enterobacteriaceae, and P. aeruginosa were 90.3% (65/72), 57.1% (52/91), and 77.8% (35/45), respectively. Pathogen distribution and MDR rates (67.7% vs. 73.6%, P = 0.416) were comparable between the two groups, except for the proportions of K. pneumoniae (14.3% vs. 26.4%, P = 0.029) and MDR Enterobacteriaceae (16.1% vs. 29.9%, P = 0.018), which were higher in the combination therapy group.
Table 2
Microscopically documented pathogens in patients with HAP
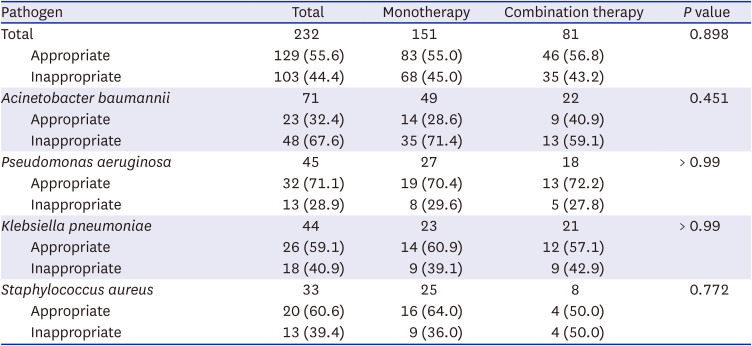
Of the 232 (36.8%) patients with available data, the appropriateness of the initial empiric antibiotics was similar between the monotherapy and combination groups (55.0% vs. 56.8%, P = 0.898) (Table 3). In the A. baumannii subgroup, the appropriateness of the initial empiric antibiotics was fulfilled only in 32.4% of the patients. In the P. aeruginosa subgroup, 71.1% of the patients were appropriately treated. In the K. pneumoniae subgroup, 59.1% of the patients were eligible for empiric antibiotics. No subgroup showed any difference in the appropriateness of initial empiric antibiotics between the monotherapy and combination therapy groups.
Table 3
Appropriateness of initial empiric antibiotics in microscopically documented HAP patients
Treatment outcomes
The 30-day mortality was 17.4%, with no difference between the monotherapy and combination therapy groups (16.8% vs. 18.2%, P = 0.729) (Table 4). Even after the PSM (Supplementary Table 1), there was no significant difference in the 30-day mortality rates between the two groups (17.5% vs.18.2%, P = 0.913) (Table 5). Moreover, other treatment outcomes, such as 90-day mortality, ICU admission, ICU or hospital length of stay, and clinical responses showed no differences between the two groups (Table 4). In the A. baumannii (22.0% vs. 18.2%, P = 0.958) and Pseudomonas aeruginosa (7.4 vs. 11.1%, P = 1.000) infection subgroups, the 30-day mortality rate was not different between the monotherapy and combination therapy groups (Supplementary Table 2).
Table 4
Clinical outcomes of HAP patients in the overall cohort before PSM
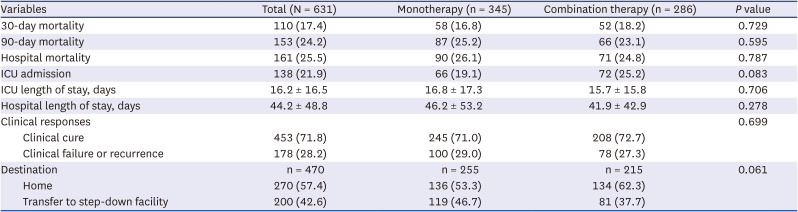
Table 5
Clinical outcomes of HAP patients in the propensity score-matched overall cohort

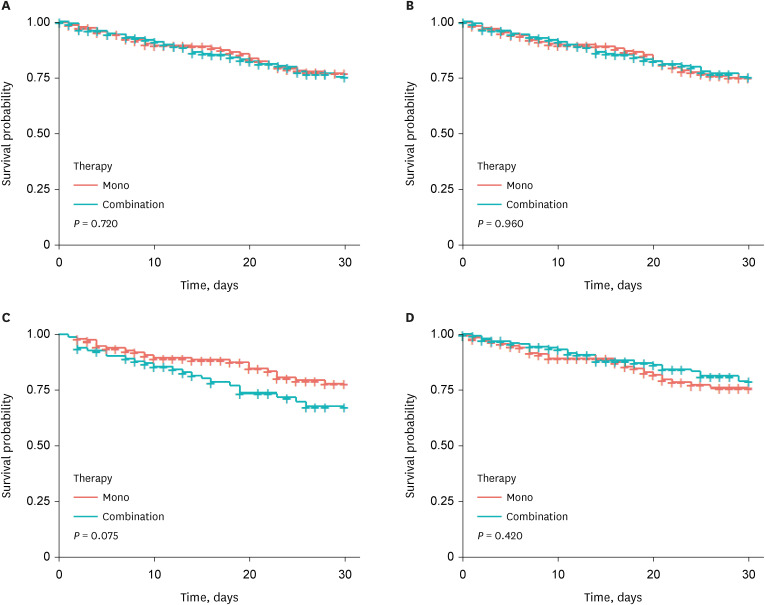
The Kaplan-Meier curves for 30-day mortality showed no significant differences between the two groups before (log-rank P = 0.720) and after the PSM (log-rank P = 0.960) (Fig. 2A and B). Moreover, there was no significant difference in the 30-day mortality between the microscopically (log-rank P = 0.075) and clinically (log-rank P = 0.420) documented patients (Fig. 2C and D). In the A. baumannii (log-rank P = 0.800) and P. aeruginosa (log-rank P = 0.780) infection subgroups, there was no significant difference in the 30-day mortality (Supplementary Fig. 1).
Fig. 2
Kaplan-Meier curve analysis for 30-day mortality. (A) Before PSM in the overall cohort (log-rank P = 0.720). (B) After PSM in the overall cohort (log-rank P = 0.960). (C) Microbiologically documented patients (log-rank P = 0.075). (D) Clinically documented patients (log-rank P = 0.420).
PSM = propensity score matching.
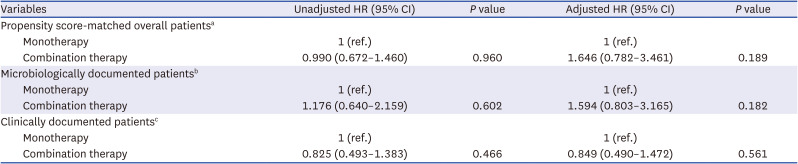
Multivariable Cox proportional hazards regression analysis revealed that the 30-day survival rate did not differ between the monotherapy and combination therapy groups after the covariate adjustment. The adjusted hazard ratio (HR) for the 30-day mortality of the combination therapy was 1.646 (95% confidence interval [CI], 0.782–3.461; P = 0.189) in the propensity score-matched overall cohort (Table 6). For the microbiologically and clinically documented patients, the adjusted HRs of the combination therapy were 1.594 (95% CI, 0.803–3.165; P = 0.182) and 0.849 (95% CI, 0.490–1.472; P = 0.561), respectively.
Table 6
Multivariable Cox proportional hazards regression models for 30-day mortality of patients with HAP
HAP = hospital-acquired pneumonia, HR = hazard ratio, CI = confidence interval, CCI = Charlson Comorbidity Index, CFS = Clinical Frailty Scale, SOFA = Sequential Organ Failure Assessment, VAP = ventilator-associated pneumonia.
aAdjusted for age, sex (male), chronic neurological disease, CCI, CFS, SOFA score, classification of infection, prior antibiotic use within 90 days, risk of aspiration, late-onset HAP, VAP, combination with glycopeptides, mechanical ventilation, renal replacement therapy, A. baumannii, Enterobacteriaceae, and P. aeruginosa.
bAdjusted for age, sex (male), chronic neurological disease, CCI, CFS, SOFA score, prior antibiotic use within 90 days, aspiration risk, late-onset HAP, VAP, combination with glycopeptides, mechanical ventilation, renal replacement therapy, A. baumannii, Enterobacteriaceae, and P. aeruginosa.
cAdjusted for age, sex (male), chronic neurological disease, CCI, CFS, SOFA score, prior antibiotic use within 90 days, aspiration risk, late-onset HAP, VAP, combination with glycopeptides, mechanical ventilation, and renal replacement therapy.
DISCUSSION
This multicenter study included patients with HAP with one of the risk factors requiring combination therapy. The patients were classified into the anti-pseudomonal β-lactam monotherapy or fluoroquinolone combination therapy groups. The identified pathogen distribution and MDR rates were similar between the two groups. However, we found no significant differences between the groups' appropriateness of initial empiric antibiotics or 30-day mortality. The Cox proportional hazards regression model in the propensity score-matched cohort showed no significant effect of the combination therapy on 30-day mortality after adjusting for covariates.
Antimicrobial inappropriateness for gram-negative organisms is a growing problem because it can increase mortality and financial burden with more extended hospital stays.51011121314 Conceptually, combination therapy among the two classes could increase the chance of appropriate empiric therapy for drug-resistant gram-negative infection.4 However, in our HAP cohort, adding fluoroquinolone to anti-pseudomonal β-lactam did not improve survival. This is because adding fluoroquinolones did not increase the appropriateness of the initial antibiotics, which may be due to the decreased fluoroquinolone susceptibility of nosocomial gram-negative bacteria.
Although the HAP/VAP guidelines recommend fluoroquinolone or aminoglycoside as an alternative combination agent,4 previous studies have demonstrated that combination of β-lactam with fluoroquinolone is less susceptible than that with aminoglycoside in P. aeruginosa infection.1516 Furthermore, a systematic review of P. aeruginosa infections in the Asia-Pacific region showed that susceptibility to fluoroquinolone was lower than aminoglycoside in all included countries.11 According to a study of antimicrobial susceptibility trends for P. aeruginosa bacteremia over 12 years, the susceptibility rate of ciprofloxacin against P. aeruginosa decreased from 80.5% to 68.4% during the period.17 Whereas, the susceptibility rates of piperacillin/tazobactam (65.5% to 63.2%) and amikacin (88.5% to 90.4%) have remained stable. Therefore, combining β-lactams and fluoroquinolones with low susceptibility would not increase antibiotic efficacy or survival in a setting of high MDR rate. To increase the appropriateness of the high risk of MDR P. aeruginosa infection, local epidemiology-based recommendations using combination susceptibility to fluoroquinolones and aminoglycosides should be considered.18
In recent years, A. baumannii, with a high MDR rate, has become the most common pathogen in patients with HAP.51920 Although we excluded patients treated empirically with carbapenem, colistin, or aminoglycosides, the most common pathogen was still A. baumannii, and the MDR rate was as high as 90.3%. The appropriateness of initial empiric antibiotics for A. baumannii was only 32.4%, and there were no significant differences in the appropriateness of initial antibiotics or 30-day mortality between the two groups. This suggests that the β-lactam plus fluoroquinolone combination is no longer an appropriate empiric option for prevalent MDR A. baumannii infections. Bae et al.21 reported that the susceptibility rate of ciprofloxacin against A. baumannii decreased from 30.7% to 17.5% over the last 20 years in Korea. Recently, colistin and tetracycline derivates have remained highly susceptible to A. baumannii.2223 The latest guideline on the carbapenem-resistant A. baumannii recommended a combination therapy with high-dose ampicillin/sulbactam, tetracycline derivates, colistin, or extended infusion of meropenem in a definitive treatment setting.24 Therefore, surveillance cultures of carbapenem-resistant A. baumannii
25 and the development of prediction models are warranted to aid the selection of these medications as empiric treatment.26
Fluoroquinolones are safe drugs that are usually well tolerated.27 However, adding ineffective fluoroquinolones may result in unnecessary and sometimes severe adverse drug events. Although any antimicrobial class might increase the chance of Clostridium difficile infection (CDI), fluoroquinolone is one of the leading causes of CDI among antibiotics.28 In the guideline for CDI management, fluoroquinolone restriction was suggested in terms of antimicrobial stewardship.29 Other adverse events are rare, but can be severe, including aortopathy, tendinopathy, and cardiac arrhythmias,30 which increased the length of stay and costs.
Unnecessary fluoroquinolone use may exacerbate antimicrobial resistance in individuals and in nosocomial environments. It is well known that increased fluoroquinolone use is associated with increased fluoroquinolone resistance in gram-negative bacilli.31 Additionally, fluoroquinolone exposure increases multidrug resistance. Kang et al.17 demonstrated that previous exposure to fluoroquinolones was associated with carbapenem-resistant (odds ratio [OR], 2.7; 95% CI, 1.3–5.7), MDR (OR, 2.4; 95% CI, 1.2–4.8), and extensively drug-resistant (OR, 3.5; 95% CI, 1.7–7.5) P. aeruginosa bacteremia.17 Paramythiotou et al.32 revealed that ciprofloxacin use increased the emergence of MDR (OR, 11.0; 95% CI, 1.27–32.9) P. aeruginosa. Moreover, Kopterides et al.33 showed that prior exposure to fluoroquinolone was the only independent risk factor for carbapenem-resistant A. baumannii bacteremia (OR, 11.6; 95% CI, 2.4–55.9). They speculated this phenomenon as fluoroquinolone use resulting in selective pressure of resistant strains or simulating the intrinsic antimicrobial efflux mechanisms.
The strength of our study is that we obtained consistent results in both microbiologically and clinically documented patients. The antibiotic appropriateness results correspond to the recent epidemiological trend of antibiotic susceptibility in P. aeruginosa and A. baumannii. However, our study has several limitations. First, patients with less severe disease might have been enrolled by excluding patients empirically treated with carbapenem, aminoglycosides, or colistin to evaluate the pure effect of non-carbapenem β-lactam monotherapy plus fluoroquinolone combination therapy. Second, data regarding subsequent definite antibiotics that could affect outcomes were not analyzed. These selection biases may preclude the generalizability of the results. Third, we did not compare crucial outcomes other than survival, such as side effects or costs. Fourth, we did not reveal each microorganism's susceptibility to β-lactams and fluoroquinolones. If the pathogens identified in the combination therapy group were susceptible to both agents, this might indicate unnecessary overuse of fluoroquinolones.
In conclusion, empiric fluoroquinolone combination therapy showed no benefit on survival or initial antibiotic efficacy compared with anti-pseudomonal β-lactam monotherapy in patients with HAP. Caution is needed regarding the routine combination of fluoroquinolones in the empiric treatment of HAP patients with a high risk of MDR. A local epidemiology-based approach is warranted to guide the selection of appropriate empiric agents for MDR gram-negative bacteria.
 XML Download
XML Download