

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The global spread of coronavirus disease 2019 (COVID-19) has caused an unprecedented number of infections and deaths. Different types of vaccines have been manufactured, for example, mRNA vaccines (BNT162b2; Pfizer-BioNTech, and mRNA-1273; Moderna), adenoviral vector vaccines (Ad26.COV2-S; Janssen/Johnson & Johnson, and ChAdOX1-nCOV; Oxford-AstraZeneca), and protein subunit vaccine (NVX-CoV2373; Novavax). mRNA vaccines are known to be superior to adenoviral vector vaccines in terms of efficacy, and they have been implemented worldwide.1 All currently available mRNA COVID-19 vaccines in the United States are formulated as a bivalent vaccine based on the wild-type strain of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and the omicron BA.4 and BA.5 (BA.4/BA.5) variants of SARS-CoV-2.2
Similar to other vaccines, COVID-19 vaccines cause mild and transient side effects, but severe and consistent adverse events have rarely been reported.34 Though large-scale clinical trials have shown the safety of these vaccines, cases of myocarditis or glomerulonephritis (GN) have emerged as the period of using the vaccines has increased. Since there are reports of GN occurring after influenza and rabies immunizations, COVID-19 vaccines are speculated to provoke a similar reaction.5 Here, we describe a case of de novo anti-neutrophil cytoplasmic autoantibody (ANCA)-negative pauci-immune crescentic glomerulonephritis (CrGN) after use of the COVID-19 mRNA vaccine, BNT162b2 (Pfizer-BioNTech).
CASE DESCRIPTION
A 48-year-old man without a specific medical history was referred for sudden and persistent worsening of renal insufficiency. He had no underlying disease or history of taking any medications. He was a current smoker (10 pack-years) and a social drinker. He had received the second dose of the COVID-19 mRNA vaccine BNT162b2. The second dose was given 24 days after the first dose of the same vaccine. He stated that arthralgia and skin rash presented a week after the second dose of the vaccination, and those were accompanied by abdominal pain and diarrhea 2 weeks after that. He was treated with antibiotics under the suspicion of enteritis. Upon colonoscopy, multiple ulcerations and petechiae suggestive of vasculitis were observed in the terminal ileum. After taking oral prednisolone (30 mg) for a few weeks, his arthralgia, skin rash, and gastrointestinal (GI) symptoms improved, but his renal function gradually deteriorated on routine weekly assessment.
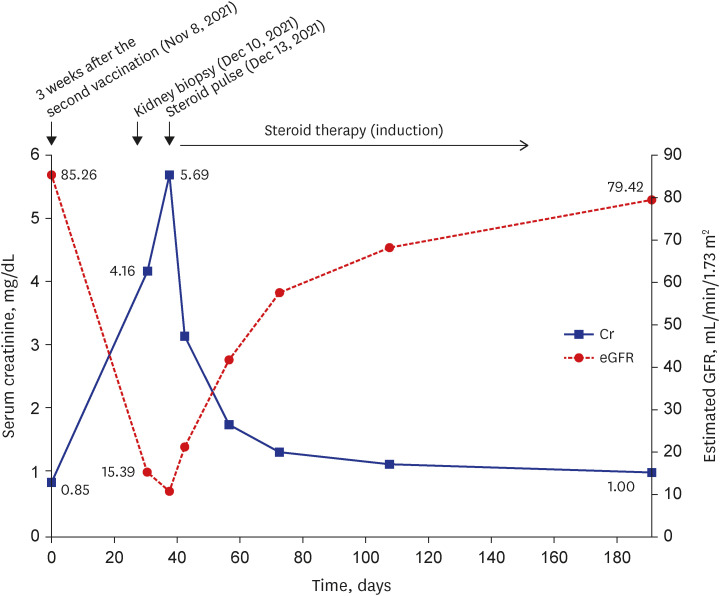
When he presented to our hospital a month and a half after the second dose of the vaccine, he reported generalized edema and foamy urine. Laboratory tests showed a serum creatinine (sCr) level of 4.16 mg/dL and an estimated glomerular filtration rate of 15.39 mL/min/1.73 m2 along with hypoalbuminemia, hematuria, and nephrotic-range proteinuria (5,306 mg/24 hours). His baseline sCr was 0.85 mg/dL a month prior (Fig. 1).
Fig. 1
Major events, the Cr level, and the eGFR during the clinical course.
Cr = creatinine, eGFR = estimated glomerular filtration rate.
Serologic tests were negative, including ANCA, antinuclear antibody, complement components, anti-glomerular basement membrane antibody, immunoglobulins, and viral markers.
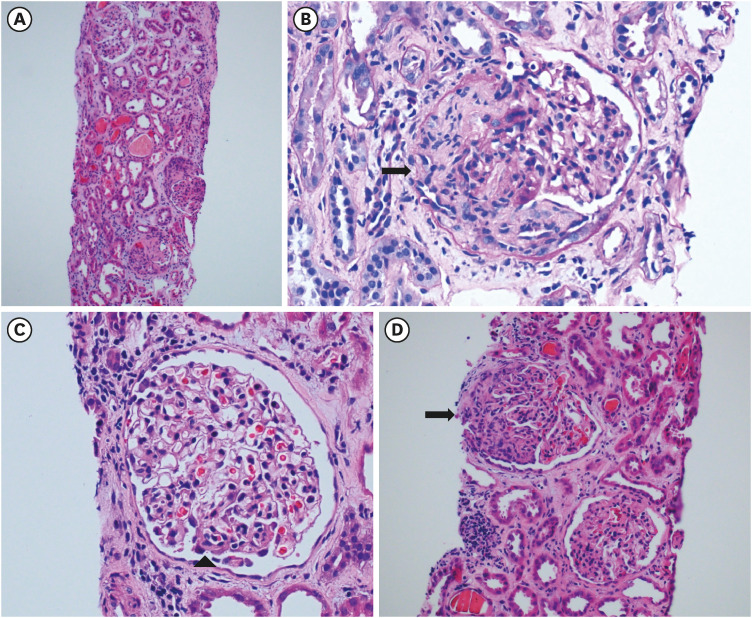
A kidney biopsy revealed diffuse CrGN with fibrocellular crescents in 11 of 14 (79%) glomeruli, focal marked tubular atrophy, and interstitial fibrosis. There was no evidence of immune complex deposits (Fig. 2). Based on these findings, ANCA-negative pauci-immune CrGN was diagnosed.
Fig. 2
Renal pathologic findings confirmed through renal biopsy. (A) Low-power field image of a biopsy specimen. (B) Fibrocellular crescent (black arrow) seen in 79% of glomeruli. (C) Increased size of the glomerulus and mild hypercellular mesangium (arrow head). (D) Fibrocellular crescent (black arrow), focal marked tubular atrophy and loss with infiltration of mononuclear cells, and fibrosis in the interstitium (red asterisk).
He began to receive intravenous methylprednisolone (500 mg) for 3 days, followed by oral methylprednisolone (0.8 mg/kg) daily for a month. He took oral cyclophosphamide (50 mg) twice a day, and the steroid was tapered over 15 weeks at 2-week intervals. His renal function improved over several weeks (sCr 1.14 mg/dL), and urine protein-to-creatinine ratio was 398 mg/gCr 2 months after the biopsy. His laboratory tests performed 3 months after the end of treatment revealed a sCr of 1.00 mg/dL and a urine protein-to-creatinine ratio of 193 mg/gCr, but microscopic hematuria was continued (urine microscopy red blood cell > 100/high-power field, in urine of specific gravity 1.012; Fig. 1). Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
DISCUSSION
To date, several cases of GN suspected to be related to COVID-19 mRNA vaccines have been reported. Minimal change disease and IgA nephropathy were the most common among these, and the others included pauci-immune CrGN, membranous nephropathy, and collapsing GN.67891011121314 To our knowledge, this is the first case report of de novo “ANCA-negative” pauci-immune CrGN with extrarenal involvement after COVID-19 mRNA vaccination in an adult patient, with prominent extrarenal involvement which is unusual in ANCA-negative vasculitis.15
ANCA has been used as a standard serologic marker of pauci-immune CrGN. ANCA might play an essential role in the pathogenesis of pauci-immune CrGN, for example, by stimulating neutrophils, which can activate the alternative complement pathway that results in vascular injury.16 However, ANCA is negative in approximately 10–20% of patients with pauci-immune CrGN, and neutrophils might be the pathogenic factor triggering the reaction even in the absence of ANCA.17 Patients with ANCA-negative pauci-immune CrGN have a greater degree of proteinuria, poorer renal outcome, lower prevalence of extrarenal involvement, and fewer vasculitic manifestations compared with ANCA-positive patients.171819
The present patient experienced skin and GI manifestations as the initial symptoms and showed a rapidly progressive GN feature of a subacute course in the renal aspect. In general, ANCA-negative pauci-immune GN is known to show less extrarenal involvement,17 but this patient showed extrarenal involvement similar to that of Henoch-Schönlein purpura, which was a very unusual presentation. In a recent case series summarizing the main characteristics of ANCA-negative pauci-immune CrGN, extrarenal involvement was reported in 54% of a total of 74 patients, suggesting that this may be more frequent than previous reports. However, among the various causes of ANCA-negative pauci-immune CrGN, only primary, infection-related, and malignancy-related cases were related with extrarenal manifestations, and there were no reports of extrarenal involvement in drug-related cases (two out of 74 patients). In addition, there was no GI manifestations in the extrarenal involvement presented in the case series. In view of this, it can be said that drug related ANCA-negative pauci-immune CrGN is very rare, and extrarenal involvement, especially GI manifestation, is very scarce.18
Previous studies have shown that mRNA vaccines induce humoral and cell-mediated immune responses that can result in de novo or relapsing GN.720 The immune response related to COVID-19 vaccination is similar to that in the COVID-19 infection itself.2122 An mRNA vaccine is composed of lipid nanoparticles as a vehicle to deliver modified mRNA encoding the SARS-CoV-2 spike protein in host target cells.23 The mRNA is released into the cytoplasm of target cells and is translated into the target protein. The target protein is then presented on the surface of helper T-cells. Then, B-cells, macrophages, and dendritic cells recognize the viral antigen and are activated. Molecular mimicry between the SARS-CoV-2 spike protein contained in the vaccine and proteins in specific human tissues, and cross-reactivity are believed to trigger autoimmune diseases including GN.24
In conclusion, we presented a man who was diagnosed with ANCA-negative pauci-immune CrGN after receiving the second dose of the COVID-19 mRNA vaccine, BNT162b2. This patient had a presentation different from that of general ANCA-negative CrGN and recovered on administration of high-dose steroids. Further in-depth studies are needed on the development of de novo GN after vaccination and COVID-19 infection to understand the mechanisms and perceive potential complications.
 XML Download
XML Download