

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Pregnant women are at risk of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection. Compared with pregnant women without SARS-CoV-2 infection, those with coronavirus disease 2019 (COVID-19) are more likely to give preterm births, be admitted to intensive care, and receive mechanical ventilation.123 COVID-19 vaccination in pregnant women effectively reduces the risk of morbidity and has a safety profile comparable to that in non-pregnant women.4 Despite reassuring clinical data, vaccine hesitancy remains in women planning pregnancy, especially with concerns regarding the risk of miscarriage and congenital anomalies in their babies.56 This hinders pregnant women from receiving COVID-19 vaccination, thus missing opportunities to prevent serious SARS-CoV-2 infections. While more than 120 countries and territories have recommended COVID-19 vaccination in pregnant women,7 globally, the estimated vaccination coverage rate among them has staggered at 18.8–37.0%.8
Safety concerns have been cited as a reason for the low COVID-19 vaccination coverage in this population, with most vaccinations occurring before the confirmation of pregnancy or late in pregnancy.910 Although studies from the U.S. and Europe have demonstrated the safety and effectiveness of the COVID-19 vaccine in pregnant women, real-world data from Asian countries are limited.11 Moreover, the findings of prior safety studies on pregnant women suffer from methodological limitations, including differences in the baseline risk of pregnancy outcomes, uncertain fetal status at the time of vaccination, and the sample size required to detect differences across populations and vaccine platforms.12
In South Korea, COVID-19 vaccination has been recommended for pregnant women since October 2021; however, the vaccination rate remains low.1314 Given that a large proportion of pregnant women were vaccinated during the preconceptional period or before the confirmation of pregnancy,15 investigating the effectiveness and safety of COVID-19 vaccination during these periods is crucial. Universal health insurance data linked to the vaccine registry database provides a unique opportunity to provide real-world evidence of COVID-19 and the effectiveness and safety profile of pregnant women in Korea. This study aimed to assess the association between COVID-19 vaccination during preconception and before confirmation of pregnancy and the occurrence of miscarriage or severe maternal SARS-CoV-2 infection using national population data linked to the immunization registry.
METHODS
Data
We used the Korean Disease Control and Prevention Agency-COVID-19-National Health Insurance Service (K-COV-N) cohort data, established by linking the National Health Insurance System (NHIS) data to information on COVID-19 infection and vaccination provided by the Korea Disease Control and Prevention Agency (https://nhiss.nhis.or.kr/). Because the NHIS covers all the essential antenatal care services for 97% of the population of South Korea, these data capture almost all the information on demographics, health check-ups, and medical conditions, including nationwide pregnancy.16 The K-COV-N database provides individual data on SARS-CoV-2 infection cases between October 2020 and December 2021, and on COVID-19 vaccination between December 2020 and December 2021. We retrieved data on women aged 20−44 years with a valid pregnancy eligible for the study based on the presence of both pregnancy and treatment codes for first-trimester obstetric ultrasonography (T1US) from February 1, 2021, to December 31, 2021 (Supplementary Fig. 1). In South Korea, two rounds of T1US are covered by the NHIS when conducted within 11 weeks of gestation17 and the first T1US is commonly conducted at approximately 6 weeks of gestation, following the guidelines.18 We excluded those with the last menstrual period (LMP) between August 2021 and December 2021, when a period of 20 gestational weeks could be incompletely observed. Because we used T1US as a landmark, where the observation of the outcome of interest started, pregnancy loss before T1US and those first vaccinated after T1US were excluded. When we analyzed the incidence of severe COVID-19, patients with a history of COVID-19 infection during the preconceptional and preclinical periods were excluded. To analyze COVID-19 vaccination and early abortive outcomes, including miscarriage, we restricted our analysis to women without documented SARS-CoV-2 infection within the 20th gestational week.
Preconceptional and preclinical COVID-19 vaccination
We divided the vaccinated pregnant women into two groups: 1) a preconceptional vaccination group, defined as those first vaccinated within six months before LMP, and 2) a preclinical vaccination group, defined as first vaccinated between LMP and T1US (no vaccination in the preconceptional period). The vaccination of the preconceptional period was defined as within six months of the LMP based on evidence indicating that COVID-19 vaccine efficacy or effectiveness against severe disease remained for six months.19 Because the presence of an intrauterine pregnancy can be confirmed only after the first T1US, the period between the LMP and the examination was regarded as preclinical. We used information on the type of vaccine (BNT162b2 and mRNA-1273 as mRNA vaccines and ChAdOx1 and Ad26.COV2.S as viral vector vaccines) first administered during the preconceptional and preclinical pregnancy periods to compare the risk of early abortive outcomes per vaccine type.
Severe SARS-CoV-2 infection and early abortive outcomes
We analyzed the effectiveness of preconception and preclinical COVID-19 vaccinations in pregnant women by assessing the risk of severe SARS-CoV-2 infection detected on intensive care unit (ICU) admission within 14 days of SARS-CoV-2 infection. Polymerase chain reaction (PCR) was used to detect COVID-19 infection in South Korea during the study period. The K-COV-N cohort database included all COVID-19-positive cases regardless of their hospitalization status. Severe SARS-CoV-2 infection during pregnancy was defined as admission to the ICU during the clinical pregnancy (between T1US and the end of pregnancy). Patients admitted to the ICU were identified based on their treatment codes.
The safety of preconception and preclinical COVID-19 vaccination was evaluated for early abortive outcomes, defined as the end of pregnancy before 20 weeks of gestation. The early abortive outcomes included miscarriage, ectopic pregnancy, molar pregnancy, and artificial abortion. Miscarriage, ectopic pregnancy, and molar pregnancy were identified based on the diagnostic codes that included ‘O02,’ ‘O03,’ ‘O04,’ ‘O07,’ and ‘O08.’ Artificial abortion was defined as the surgical removal of gestational materials before 20th weeks of gestation with no diagnostic codes for early abortive outcomes and identified with the presence of treatment codes for uterine dilatation and evacuation. Given that ectopic and molar pregnancies and artificial abortions are less likely to be affected by preclinical pregnancy vaccination, we further assessed the association between vaccination and miscarriage, excluding other abortive outcomes.
Covariates
Our model included the age of the women at the time of vaccination, body mass index (BMI), socioeconomic status, and season of conception. We assessed individual socioeconomic status using the information on income decile ranking, employment, presence of disabilities, and residence in the Seoul capital area. The Seoul capital area includes Seoul, Incheon, and Gyeonggi-do, where half of the South Korean residents live and have better social infrastructure than other provinces. Variables were selected based on prior knowledge of the risk factors for severe COVID-19 morbidities, early abortive outcomes, and availability in the K-COV-N database.202122 The employment status of the women was coded based on the NHIS subscription type, which specified employees. The K-COV-N database contains individually linked decile household income data. For analytical convenience, the household income levels of the individual data were divided into four groups (1st [lowest], 10–30%; 2nd, 40–60%; 3rd, 60–80%, and 4th [highest], 80–100%) for analytical convenience. Information on employment (yes or no) and residential area (at the district level) was coded based on the type of insurance subscription.
Statistical analysis
When analyzing early pregnancy outcomes, defining risk exposure simply by vaccination during pregnancy can lead to an erroneous estimation of survival probability.23 Furthermore, in the analysis of pregnancy outcomes, the survival time of patients with early abortive outcomes was not clinically meaningful. Given that the decision to COVID-19 vaccination during pregnancy is affected by gestational age, the probability of COVID-19 immunization during pregnancy cannot be considered consistent over gestational age. To minimize the time-dependency of COVID-19 vaccination during early pregnancy, the date of T1US was used as a landmark from which the outcomes of SARS-CoV-2 infection and early abortive outcomes were examined (Fig. 1).
Fig. 1
Concept of coronavirus disease 2019 vaccination during preconceptional and preclinical pregnancy periods and the first T1US as a landmark. The time of T1US was used as a landmark where the observation of the outcome of interest starts.
T1US = first-trimester obstetric ultrasonography, LMP = last menstrual period.

Women who did not receive any vaccinations during the preconception and pregnancy periods were used as controls. Given the low vaccination rate in pregnant women, we matched the vaccinated groups to unvaccinated controls in a 1:4 ratio based on age, income, BMI, and season of conception. In the effectiveness study, we analyzed the risk of SARS-CoV-2 infection and ICU admission within 14 days of infection. Because the incidence of ICU admission was extremely low in all groups, we calculated the adjusted odds ratios only for SARS-CoV-2 infection. To evaluate safety, we estimated the adjusted relative risks (aRRs) of early abortive outcomes and miscarriage for the first vaccination during preconceptional and preclinical periods, adjusting for individual covariates. We separately analyzed the risk of miscarriage, a subgroup of early abortive outcomes. We then compared the risk of early abortive outcomes and miscarriages between the mRNA and viral vector vaccines for each period. The BNT162b2 and mRNA-1273 vaccines were combined into a single mRNA vaccine because all women under 30 years of age received the Moderna vaccine following the country’s immunization policy. All statistical analyses were performed using the SAS software (version 9.4; SAS Institute, Cary, NC, USA).
RESULTS
The overall COVID-19 vaccination rates during preconceptional and preclinical pregnancy periods were 3.1% (6,662/215,211) and 2.6% (5,702/215,211), respectively. In the eligible population, 24,524 women in the control group were matched with 6,131 (92%) women who were first vaccinated during the preconception period. For the preclinical period analysis, 21,136 controls were matched to 5,284 women who were first vaccinated with LMP and T1US. When comparing cases and matching controls, vaccination during the preconceptional or preclinical period was associated with a higher probability of living in the Seoul capital area (51.5% in preconceptional and 51.2% in preclinical pregnancy vs. 45.2% and 46.8% in matched controls, respectively) and employment (78.5% and 65.5% vs. 61.8% and 56.8%, respectively) during pregnancy (Table 1). Among the vaccinated women, those first vaccinated during the preconceptional period were more likely to receive the ChAdOx1 vaccine and were vaccinated in spring than those first vaccinated during preclinical pregnancy (Supplementary Table 1). Most women were vaccinated with ChAdOx1 (70.6%) during the preconceptional period, whereas the majority were vaccinated with mRNA vaccines (70.7%) during the preclinical pregnancy period.
Table 1
Demographic and clinical characteristics of pregnant women according to COVID-19 vaccination during preconceptional and preclinical pregnancy periods with their matched controls, the Korea Disease Control and Prevention Agency-COVID19-National Health Insurance Service cohort data
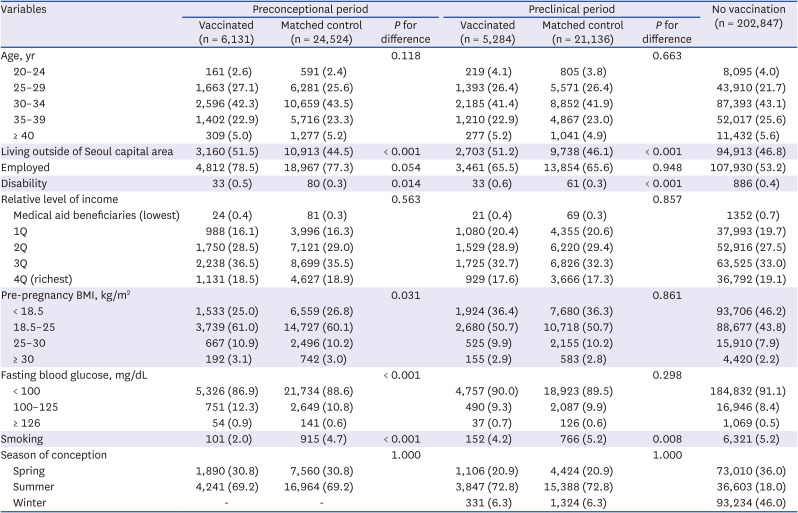
Values are presented as number (%). Preconceptional vaccination was defined as any vaccination during the six months before the LMP. Preclinical vaccination was defined as any vaccination between the LMP and T1US, excluding those vaccinated during the preconceptional period. The Seoul capital area refers to Seoul, Incheon, and Gyeonggi Provinces located in northwestern South Korea. No pregnancies were conceived in the fall because we excluded those with conception dates between August and December.
COVID-19 = coronavirus disease 2019, BMI = body mass index, 1Q = 1st quartile, 2Q = 2nd quartile, 3Q = 3rd quartile, 4Q = 4th quartile, LMP = last menstrual period, T1US = first-trimester obstetric ultrasonography.
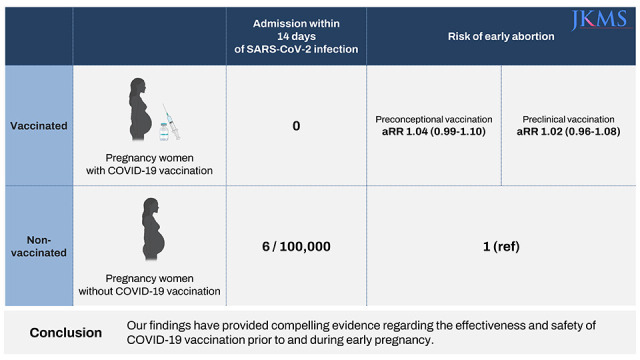
In the analysis of SARS-CoV-2 infection and ICU admission within 14 days of SARS-CoV-2 infection, the cumulative incidences of SARS-CoV-2 infection with no vaccination, preconceptional vaccination, and preclinical vaccination were 157, 210, and 316 per 100,000 pregnant women, respectively (Table 2). The cumulative incidence of ICU admission within 14 days of SARS-CoV-2 infection was 6/100,000 pregnant women who received no COVID-19 vaccination throughout the preconception period and during pregnancy. There were no ICU admission cases in the preconceptional period or the preclinical pregnancy vaccination groups. No deaths occurred within 14 days of SARS-CoV-2 infection in the study population. The odds of SARS-CoV-2 infection were generally lower when vaccinated during the preconceptional or preclinical pregnancy periods, although the differences were not statistically significant (Supplementary Table 2). When comparing the odds of SARS-CoV-2 infection for viral vector vaccines with those for mRNA vaccines, the adjusted risk estimates were generally imprecise because of the extremely low incidence of SARS-CoV-2 infection (Supplementary Table 3).
Table 2
SARS-CoV-2 infection and ICU admission within 14 days of SARS-CoV-2 infection, according to COVID-19 vaccination during the preconceptional period and preclinical pregnancy, and no vaccination, the Korea Disease Control and Prevention Agency-COVID19-National Health Insurance Service cohort data

Early abortive outcomes occurred in 20.7% (5,090/24,524) of the unvaccinated women and 21.6% (1,326/6,131) of the vaccinated women during the preconception period (Table 3). The incidence of miscarriage was similar between the two groups (18.7% vs. 18.9%). The risks of early abortive outcomes (aRR, 1.05; 95% confidence interval [CI], 0.99–1.10) and miscarriage (1.04; 95% CI, 0.98–1.10) were not significantly different between the preconceptional vaccination group and control. When comparing women who received the preclinical vaccination with their matched controls, the early abortion rates were 20.8% (4,406/21,136) in the unvaccinated control group and 21.3% (1,128/5,284) in the vaccinated group. The risk of abortive outcomes (1.02; 95% CI, 0.96–1.08) and miscarriage (1.01; 95% CI, 0.95–1.07) for preclinical vaccination were close to null. When comparing the risk of early abortive outcomes among vaccinated women, those first vaccinated with mRNA, ChAdOx1, and Ad26.COV2.S during the preconception period experienced early abortion outcomes in 20.7%, 21.5%, and 22.9% of the cases, respectively. For the first vaccination during preclinical pregnancy, the early abortion rates in women receiving mRNA, ChAdOx1, and Ad26.COV2.S were 20.8%, 22.0%, and 20.8%, respectively. The miscarriage rates were 18.0%, 20.4%, and 18.9% for mRNA, ChAdOx1, and Ad26.COV2.S vaccines, respectively. When compared with mRNA vaccines, ChAdOx1 and Ad26.COV2.S showed similar risks of early abortive outcomes and miscarriage in both periods.
Table 3
Adjusted relative risk of early abortive outcomes and miscarriage by coronavirus disease 2019 vaccination and the type of vaccine during the preconceptional and preclinical periods
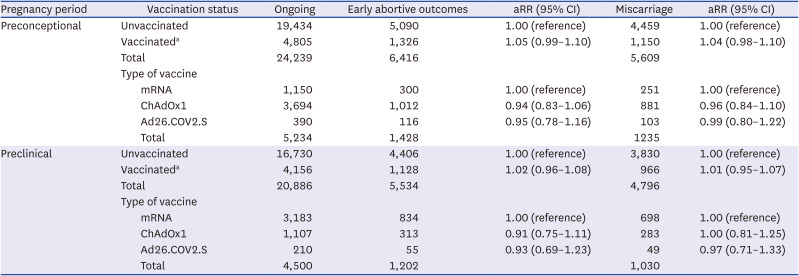
RRs were adjusted for age, income, body mass index, the season of conception, and employment at the time of pregnancy. mRNA denotes BNT162b2 and mRNA-1273 vaccines.
aRR = adjusted relative risk, CI = confidence interval.
aThe sum of vaccinated women does not equate to the column sum of each vaccine type due to the fact that only those individuals matched with the unvaccinated group were included in the matched analyses concerning vaccination status.
DISCUSSION
In a national population cohort of Korean women, we observed that the risk of SARS-CoV-2 infection during pregnancy was comparable between women who were vaccinated during the preconceptional or preclinical pregnancy period and those who were never vaccinated. Although this event was rare, there were no cases of ICU admission after SARS-CoV-2 infection in the vaccinated group. The risks of early abortive outcomes and miscarriage were not significantly different between the vaccinated and never-vaccinated groups. The risks were similar across the types of vaccines, regardless of preconceptional or preclinical pregnancy periods. Although the findings are limited by the low number of severe SARS-CoV-2 infections to analyze the risk, our study provides reassuring evidence of the effectiveness and safety of COVID-19 vaccination in pre- or early pregnancy, which are likely inadvertent vaccinations.
The protective effect of COVID-19 vaccination against SARS-CoV-2 infection during pregnancy has been reported previously. The pooled effectiveness of the vaccine against PCR-confirmed SARS-CoV-2 infections after the second dose was 89.5%.24 A recent meta-analysis showed a reduction of SARS-CoV-2 infection and COVID-19-related hospitalization among fully vaccinated pregnant women.25 The close-to-null association between SARS-CoV-2 infection and COVID-19 vaccination in our study could be due to the substantially lower incidence of ICU admission and vaccination rates in early pregnancy in South Korean pregnant women than in other populations.
Our finding of a comparable risk of early pregnancy loss is consistent with previous reports. Despite methodological heterogeneity, studies have shown that miscarriage, ectopic pregnancy, and stillbirth risks in vaccinated pregnant women are not higher than those in non-vaccinated.262728 Notable differences in methodologies between the previous study and our study include the inclusion of preconceptional vaccination and a considerable proportion of vaccinations with AstraZeneca. If we had included only those who were vaccinated during pregnancy, including in the second trimester, our estimation of vaccine effectiveness could have been higher. Furthermore, risk estimates would have moved toward null because of the potential disadvantages of viral vector vaccines.29 Given that uncertainties remain regarding the timing of pregnancy loss and bias determination from the self-selection of vaccinated groups, more reproducible methodologies to assess vaccination safety during pregnancy would need to be developed.
Despite the current guidance from leading health organization recommendations requiring COVID-19 vaccination during pregnancy and growing evidence of the effectiveness and safety of vaccination,30313233 the reported COVID-19 immunization rate among pregnant women remains low compared with other high-risk populations, ranging from 6.8% to 68.7%.8 In a sample of pregnant women in the United States, 61.0% received at least one dose of the COVID-19 vaccine, and 54.3% completed their primary series as of April 2022.34 In 2021, 32.7% of pregnant women in a UK cohort received at least one COVID-19 vaccine during pregnancy.35 Considering the global disparities in COVID-19 vaccination rates, especially in pregnant women,36 further research should focus on strategies to improve COVID-19 vaccination uptake during pregnancy.
The interpretation of our findings requires caution owing to some limitations. First, using the NHIS claims data, pregnancy outcomes based on the diagnostic and treatment codes might have been misclassified in some of our populations. Because the overall incidence of miscarriage was reported to be 10–20%, the comparable incidence of miscarriage in our study population supports the validity of our estimation. Second, we could not delineate the impact of partial and complete vaccination in the population because the general incidence of SARS-CoV-2 infection and vaccination rates were extremely low to conduct a stratified analysis. When the database was extended to a more recent timeframe, where the vaccination rate during pregnancy was higher than ours, we would be able to analyze vaccine effectiveness against severe SARS-CoV-2 infection.
We observed a comparable risk of early abortive outcomes in women exposed to COVID-19 vaccination during pre- and early pregnancy with women who were never vaccinated. Further research is required to determine the long-term safety and effectiveness of COVID-19 vaccines for pregnant women and their offspring.
 XML Download
XML Download