

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
A central venous catheter (central line) inserted directly into the right atrium through large veins is one of the most fundamental techniques in modern medical procedures. Central lines are commonly used to inject medicines directly into the heart or for blood sampling. Various methods for this technique are widely used, depending on the patient’s condition or treatment methods and period, and type of medication. There are three cases in which a central venous catheter is needed during treatment: chronic patients who need consistent injection of medicines, such as patients with cancer; patients who patients who need complete nutritional supplementation due to unconsciousness or problems with the digestive system or food intake; and patients who need repeated checkups through blood tests.12 For these patients, it is highly inefficient to set a new line for every injection or blood sampling; therefore, a tube is inserted into the central vein for a certain period, and various important treatments are administered through this line.
For this, central lines are the most used conventional method. They have different advantages depending on the insertion site, and their use varies according to the type. Catheters are commonly inserted through the subclavian or internal jugular veins. The advantage of using the subclavian vein is that it is easier to dress and is stable even with a change in the patient’s posture. The advantage of using the internal jugular vein is that it has a high success rate in insertion and is easier to access the right atrium.34 There are various types of central lines, including non-tunneled infusion catheters, non-tunneled dialysis catheters, tunneled infusion catheters, tunneled dialysis catheters, and implantable ports. Currently, two representative central lines are most commonly used in the clinical field. The Hickman catheter, included in the tunneled infusion catheters, is connected outside of the body and is used for hematopoietic stem cell transplantation or blood sampling. The Chemo port, included in the implantable ports, plants the opening of the catheter hypodermically to lower the risk of infection. The central line is a clinically significant technique, but current studies have reported complications triggered during procedures and maintenance. Basically, the access region of the central line is the neck and shoulder, where large vessels, nerves, and pleura are complexly intertwined; thus, approaching this location is accompanied by high risks. In addition, the incidence of complications, such as pneumothorax, hemothorax, air embolism, phlebitis, and nerve and artery injury is high,5 and a high risk of infection makes long-term maintenance difficult,6 placing a burden on both practitioners and patients by having to repeat the procedure continuously.7
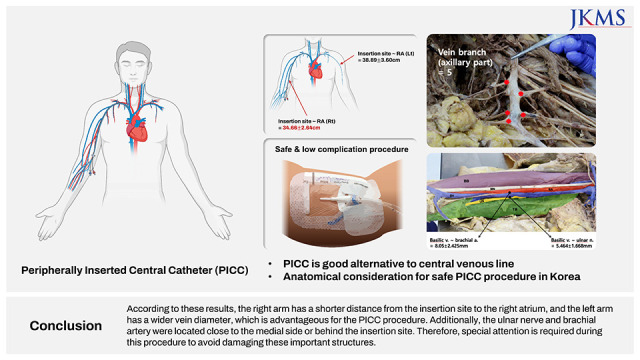
To utilize the advantages of the central line and overcome its limitations, a peripherally inserted central line (PICC) was introduced. This technique was first developed for chemotherapy in pediatric patients with cancer in 1960 and was first published by Hoshal8 in 1975; its usage was trivial before 1990, but is currently widely used in clinical practice.9 This is fundamentally the same procedure as the central line; however, the main difference is that it uses the peripheral veins of the arm instead of the large vein. Usually, the basilic vein, the largest deep vein of the arm, is used because the course is straight and the risk of arterial puncture is low. PICC has been known to have a higher possibility of causing deep vein thrombosis,1011121314 because of the long length the catheter travels, and its surface area exposure to blood is wider15; however, many studies have shown that this can be solved with plenty of practice and support from ultrasound or electrocardiogram.161718192021 Compared to the central line, PICC can be used safely even on neonates and children,22232425 does not require anesthesia or sedation, can be inserted without surgery,26 can be sustained for a long period of time, from 3 months to as long as an year,2728 is cost efficient,29 has low rates of complications and infection,303132 and can be performed by a professionally trained nurse, making it highly time efficient and cost effective for inpatients and patients cared for at home.3334 In addition, patients with a very high body mass index have a thick subcutaneous tissue in the neck, making it difficult to insert the central line. In this case, the PICC can be inserted through the peripheral vein of the arm using ultrasound guidance.35 PICC is a useful alternative for patients who have had renal transplants with neck vein thrombosis or multiple punctures that can cause chronic anemia or patients who are unable to be in a lying position due to severe pain or breathing difficulties.3637
Owing to these advantages, there has been a rising trend in the use of PICC in many hospitals. More than 2.5 million PICC procedures had been performed in the United States and more than 5 million around the world by 2008; by 2011, 15 million had been performed.6 Training programs for nurses started around 1970–80 and became pervasive during the 1990s; nowadays, 60% of the procedures are performed by professionally trained nurses.38 In Korea, several studies have been conducted on PICC, mainly summarizing basic procedures and precautions,39 or large-scale follow-up studies in hospitals, revealing the average duration and complication rates.404142 More specifically, there have been retrospective analyses of PICC procedures performed by well-trained nurse practitioners,43 safety studies of PICC in patients with burns, trauma, and chemotherapy,4445464748 and outcomes analyses of PICC performed at the bedside in critically ill patients who cannot be transported to an interventional radiology suite.4950 Other studies have devised formulas to optimize catheterization length and tip placement using patient height, weight, and ultrasound-determined anatomical features.5152
Despite this, there is a lack of research providing guidelines for PICC based on the position-relationship between anatomical structures, although guidelines for the central line have been mostly established.62053
Current studies have mainly focused on comparison analysis of complications and infections between central line and PICC that have been clinically proven, or established via medical imaging of anatomical structures56101112131617181920; therefore, this study was conducted to provide anatomic knowledge for safe PICC procedures through cadaver dissection.
METHODS
Study group
We used 40 arms from 20 fixed cadavers donated to Korea University College of Medicine (men: 10, women: 10, and mean age: 76.75 [48–94]).
Cadaveric study
Both arms of the cadavers were dissected to make the veins, arteries, and nerves clearly visible, and the parameters, which might be helpful when performing PICC procedures in the clinical field, were measured (Fig. 1). To determine the parameters, we consulted a radiologist with considerable practical experience.
Fig. 1
Vessel and nerve structures in the arm. Total length of the arm (greater tubercle–lateral epicondyle) (↔); Distance from the medial epicondyle to the splitting point of the brachial vein from the basilic vein (<--->); Insertion site (midpoint of total arm length, ▼); Distance from the basilic vein to the brachial artery and the ulnar nerve (◆); Vein branches in the axillary region (★).
LE = lateral epicondyle, ME = medial epicondyle, GT = greater tubercle.

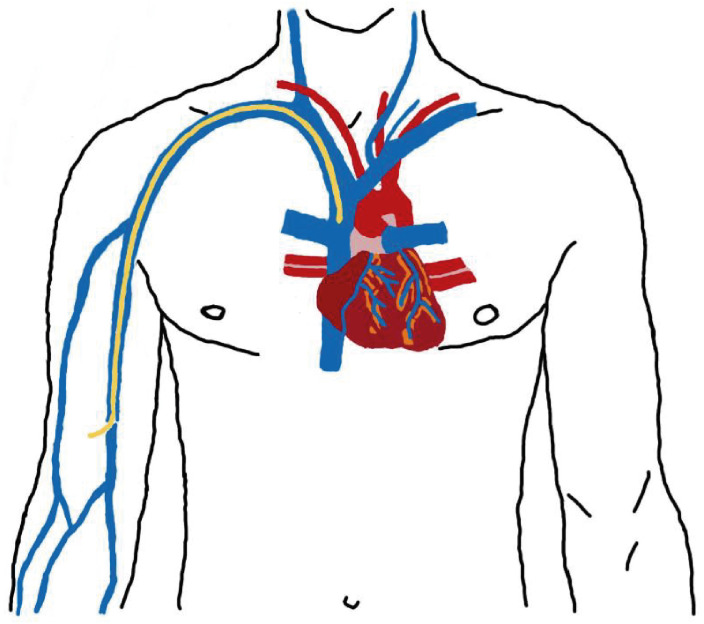
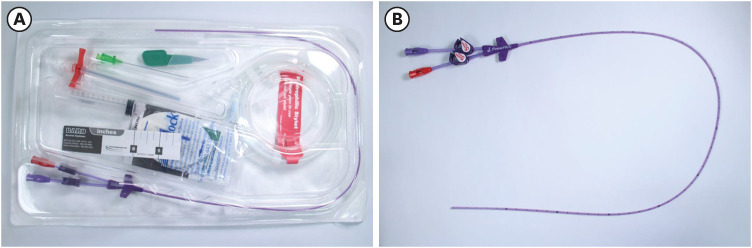
First, the total length of the arm and the distance from the greater tubercle to the lateral epicondyle of humerus were measured. The midpoint of the total arm length was designated as the insertion site. The length from the insertion site to the transition point from the superior vena cava to the right atrium was measured by inserting the catheter used in the actual PICC procedure into the basilic vein (Fig. 2). We used a Power PICC® Catheter (BARD Access Systems, Inc., Salt Lake City, UT, USA) for this procedure (Fig. 3). In addition, the distance from the basilic vein to the nearby structures such as median and ulnar nerves, and brachial artery was measured at the insertion site, and the diameter was measured using thinly sliced veins extracted at the same point. To set the upper limit of the insertion site, the location of brachial vein splitting from the basilic vein was confirmed, and the number of vein branches with diameters and paths that could prevent the catheter from progressing in the axillary region was also confirmed. Each parameter was measured after dissection, using a measuring tape and digital calipers, while trying to maintain the original position of every structure. To determine its diameter, a thin part of the basilic vein near the insertion was sampled, photographed, and measured using digital calipers.
RESULTS
After determining the insertion site based on bony landmarks and the distance from the greater tubercle to the lateral epicondyle as the standard arm length, the anatomical relationship of the close structures was checked after dissection. Consequently, the nerve and vascular structures around the basilic vein were very close to each other. In particular, the brachial artery and ulnar nerve were located closer to each other than anticipated on both sides. When looking at the actual measured value, the brachial artery was situated on the deep lateral side of the basilic vein with a mean distance of 8.05 ± 2.42 mm, and the ulnar nerve was located on the medial side of the basilic vein with a mean distance of 5.46 ± 1.67 mm (Fig. 4).
Fig. 4
Dissected arm. Purple (BB) is the biceps brachii muscle, green (TB) is the triceps brachii muscle, yellow (UN) is the ulnar nerve, red (BA) is the brachial artery, blue (BV) is the basilic vein, and MN is median nerve. Based on the basilic vein, the brachial artery is located on the deep lateral side with a mean distance of 8.05 ± 2.43 mm, the ulnar nerve is located on the medial side with a mean distance of 5.46 ± 1.67 mm.

Mean values of all the measured parameters: the distance from the greater tubercle to the lateral epicondyle was 28.87 ± 1.94 cm, from the insertion site to the right atrium was 36.56 ± 3.56 cm, from the medial epicondyle to the meeting point of brachial and basilic veins was 192.81 ± 24.48 mm; the number of vein branches in the axillary region was 5.00 ± 1.21; and the diameter of the basilic vein was 4.55 ± 1.39 mm. (Fig. 5) When the results were analyzed considering sex and sides, the distance from the insertion site to the right atrium showed a significant difference with sex (P = 0.032); however, considering the natural difference based on sides due to the position of the heart, both sex and sides were considered in the calculation, thus showing insignificance (P = 0.059, left side and P = 0.198, right side). When comparing the distance from the insertion site to the right atrium based on the sides, there was a significant difference (P < 0.001) (Table 1).
Fig. 5
Vein branch observed in the axillary region and basilic vein extracted from the insertion site. (A) Vein branches in the axillary region that are wide enough for a catheter to pass through, which are divided by travel direction, upward or downward. (B) The thinly sliced basilic vein from the insertion site was placed under the measurement device, then a photo was taken and the precise diameter was measured using digital calipers.
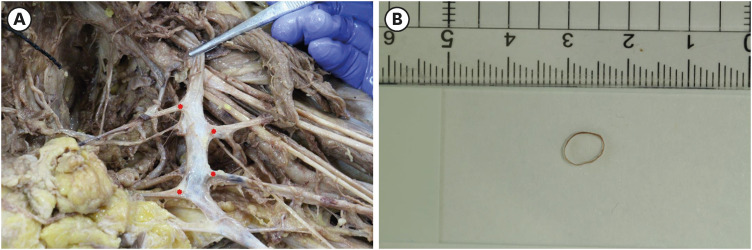
Table 1
Measured value by side and sex
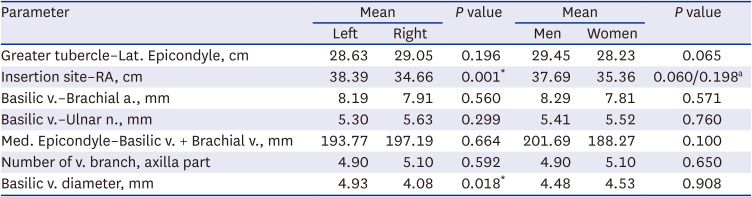
a. = artery, lat. = lateral, n. = nerve, v. = vein.
*P < 0.05.
aSignificance comes from the inevitable difference from the positioning of heart; therefore, re-analysis based on both sex and sides showed P ≥ 0.05, resulting in insignificance (men and women left side, P = 0.059 and men and women right side, P = 0.198). Compare with only sex, the P value was 0.032.
DISCUSSION
First, a parameter with significant difference was the distance from the insertion site to the right atrium, which was 3.73 cm longer on the left side than on the right side. This was hypothesized before the study, since the right atrium is located to the right.54 This result is expected to help determine the catheter length in clinical settings. In addition, the diameter of the basilic vein was not significantly different between the sexes, but it was larger on the left side than on the right side. The reason for this is unknown, but previous studies have speculated that doctors inserting central venous catheters prefer the right arm for convenience, and thus there is a possibility that the veins could have atrophied due to frequent injection of toxic drugs in the preferred right arm of patients with chronic diseases.55 This result could show the benefits of using the left arm for patients who cannot receive injections in the right arm for various reasons. Another advantage is that venous thrombosis, the most frequent side effect of inserting a PICC, has been reported to occur more frequently in thin blood vessels; therefore, this probability may be reduced when performed on the left arm.1556
In the axillary region, an average of five vein branches was thick enough for the catheter to pass through. Among these veins, the mean of 1.62 branches had an upward tendency, similar to the progress direction of the catheter, and the mean of 3.44 branches had a downward tendency (Fig. 5A).
Even though there was no significant correlation, these vein branches could interfere with the catheter pathway, and it would be helpful to know the number, location, and direction of these veins in advance.
It is important to note that the two closest structures, the brachial artery and ulnar nerve, were situated very close to the basilic vein, where the catheter was inserted. When performing the PICC procedure in the clinical setting, it is important to be careful not to damage major structures; thus, the distance and positional relationship found in this study will benefit in doing so.
The reason this study focused solely on the basilic vein is because the cephalic vein, an alternative, is too thin, has a high possibility of thrombosis, goes through the shoulder, causing movement of the catheter to increase, resulting in phlebitis56; axillary vein is an option with a large diameter but is close to the brachial artery and is covered with a thick subcutaneous fat layer57; the brachial vein, another alternative, has a higher possibility of damaging the median and anterior interosseous nerves or the brachial artery when injecting a needle,38585960 thus the basilic vein is most commonly used. However, depending on the state of the patient’s basilic vein, the cephalic or brachial veins are sometimes used; therefore, further research on these veins is needed.
 XML Download
XML Download