

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Paroxysmal nocturnal hemoglobinuria (PNH) is a rare hematologic disorder characterized by uncontrolled activation of the terminal complement pathway, resulting in intravascular hemolysis, a risk of thromboembolic events (TEs), and organ damage (e.g., kidney impairment and pulmonary hypertension).123 The clinical symptoms of PNH are debilitating, reduce health-related quality of life, and can be fatal if left untreated.34
Eculizumab, a first-in-class complement component 5 (C5) inhibitor, was the first disease-specific treatment to be approved for patients with PNH; it has been the standard treatment for PNH in most countries since its approval in 2007.56 Eculizumab therapy has been associated with significantly improved rates of survival compared with historical controls receiving supportive care.78 PNH symptoms and disease-related complications are reduced with eculizumab treatment, and survival improved to a level near that of the general population.5
In Korea, reimbursement for eculizumab therapy by the Health Insurance Review and Assessment Service (HIRA) is limited to patients who have at least one PNH-related complication alongside elevated serum lactate dehydrogenase (LDH) levels of at least 1.5 × upper limit of normal (ULN). Despite the high disease burden in this PNH population, previous studies have reported survival benefits during eculizumab treatment in patients with PNH in Korea.910 However, these earlier studies were limited because of a lack of detailed prognostic clinical data to assess treatment response over time. For the continued prescribing of eculizumab treatment in Korea, a monitoring report must be submitted every 6 months to the special committee of HIRA. The monitoring reports contain detailed clinical information for each patient with PNH treated with eculizumab in Korea.
The objective of this study was to evaluate the long-term efficacy and safety of eculizumab in patients with PNH with a high disease burden and severe PNH-related complications in real-world clinical practice. The study also evaluated differences of response in PNH-related complications after eculizumab treatment and the incidence and clinical characteristics of extravascular hemolysis (EVH) and breakthrough hemolysis (BTH) in this patient population.
METHODS
Study design
This retrospective, multicenter, observational study enrolled adult patients with PNH receiving eculizumab treatment from December 1, 2009 to January 31, 2020. Participants were recruited from 14 institutions in Korea. Clinical information (including death) was collected from the time of PNH diagnosis to the end of eculizumab treatment or July 31, 2020 (data cut-off date). Data were entered by the investigator (or delegate) based on the patient’s electronic medical records through an electronic case report form. The results of laboratory tests were collected before eculizumab treatment, at 6, 12, and 24 months after the start of eculizumab treatment, and every 12 months thereafter.
Patient population
Patients aged 18 years or above with a diagnosis of PNH, confirmed by flow cytometry, who started eculizumab treatment in accordance with the drug label before January 31, 2020 were included in the study. Patients who had started eculizumab as part of a clinical trial or an expanded access program/compassionate use program prior to 2012 were also eligible.
Patients were required to have been vaccinated against Neisseria meningitidis at least 2 weeks prior to starting eculizumab treatment. If eculizumab therapy was initiated within 2 weeks post-vaccination, they must have been treated with appropriate prophylactic antibiotic therapy. Patients were excluded if they were aged under 18 years, had hypersensitivity to the active ingredients of eculizumab, had an untreated meningococcal infection (N. meningitidis), or had received other complement inhibitor therapy for PNH before or during eculizumab treatment.
Outcome measures
Patient demographics and clinical characteristics were reported at baseline. The primary endpoint was eculizumab efficacy assessed by intravascular hemolysis, occurrence of PNH-related complications and clinical symptoms, severity of anemia (including the required units of packed red blood cell [pRBC] transfusions), and investigator-assessed effectiveness evaluation at the last follow-up based on the comprehensive judgment of clinical features such as hemolysis, anemia, and improvement of PNH-related complications.
Hemolysis after eculizumab treatment was evaluated using LDH levels and the severity of anemia using hemoglobin (Hb) levels. Occurrence and the types of PNH-related complications were based on the investigator’s judgment (captured from 6 months before eculizumab administration to the end of the administration or last follow-up). TEs were defined as thrombosis or embolism requiring anticoagulant therapy. Pulmonary hypertension was defined as chest pain and shortness of breath leading to the limitations of normal activity (New York Heart Association Class III or above) and medically confirmed pulmonary arterial hypertension11; laboratory tests for N-terminal pro-B-type natriuretic peptide (NT-proBNP) and pro-B-type natriuretic peptide (proBNP) were also collected. Renal failure was defined as an estimated glomerular filtration rate (eGFR) less than 60 mL/minute/1.73 m2 or a history of dialysis due to PNH-related acute kidney injury. Smooth muscle spasm was defined as episodes of severe, recurrent pain requiring hospitalization or narcotic analgesics. The effectiveness evaluation of the treatment was based on the investigator’s judgment for the entire observation period and classified as improved, unchanged, or worsened.
Additional endpoints included incidence of EVH, BTH, and overall survival. EVH was assessed by investigator judgment based on a positive direct antiglobulin test (direct Coombs test) along with decreased Hb and increased reticulocytes, and/or presence of transfusion.12 BTH was defined as at least one new or worsening sign or symptom of intravascular hemolysis (fatigue, hemoglobinuria, abdominal pain, dyspnea, anemia [Hb < 10 g/dL], major adverse vascular events [MAVEs] including thrombosis, dysphagia, or male erectile dysfunction), and LDH levels of at least 2 × ULN (ULN for each study site was based on each site’s laboratory reference range) after prior reduction of LDH levels to less than 1.5 × ULN on treatment.13 MAVEs included TEs, pulmonary embolism, amputation (nontraumatic, nondiabetic), myocardial infarction, cerebral artery occlusion/transient ischemic attack, unstable angina, and gangrene (nontraumatic, nondiabetic).
Safety, including infection, adverse drug reactions leading to discontinuation of eculizumab administration, and fatal events related to eculizumab administration, were assessed up to 3 months after the end of eculizumab administration or data cut-off.
Statistical analysis
Considering the low prevalence and incidence of PNH, all possible cases that fit the inclusion/exclusion criteria were enrolled in the study and there was no planned statistical sample size. Means, standard deviations (SDs), medians, and ranges were reported for continuous variables; frequencies and percentages were reported for categorical variables. Categorical and continuous variables were summarized using descriptive statistics for patients measured before and after eculizumab treatment, and data were analyzed by paired t-tests or Wilcoxon signed-rank tests. Time-to-event data, including EVH, BTH, and overall survival, were estimated using the Kaplan–Meier curve method (censored: last follow-up date).
RESULTS
Patient demographics and clinical characteristics
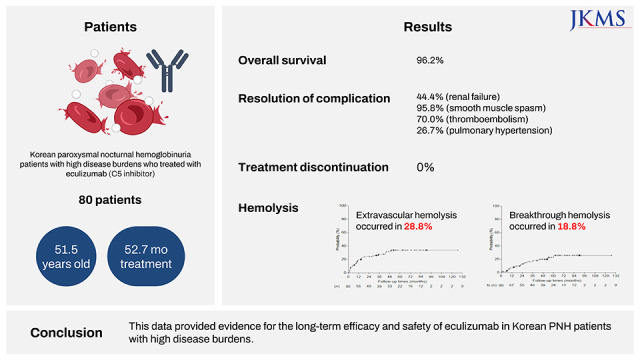
In total, 80 patients were enrolled in the study, of whom 62.5% (n = 50) were male (Table 1). The median (range) age at the time of eculizumab initiation was 51.5 (18.0, 88.0) years and the median (range) length of time from PNH diagnosis to the start of eculizumab treatment was 68.5 (2.0, 456.0) months. At diagnosis, 75.0% of patients (n = 60) were classified as having classical PNH and 25.0% (n = 20) as having aplastic anemia (AA) or myelodysplastic syndromes (MDS). The median (range) LDH level at treatment initiation was 6.8 (0.6, 29.8) × ULN and the median (range) granulocyte clone size was 93.0% (15.4%, 100.0%). Renal failure was the most common PNH-related complication reported by clinicians that led to the initiation of eculizumab treatment (n = 36), followed by smooth muscle spasm (n = 24), TEs (n = 20), and pulmonary hypertension (n = 15). The median (range) duration of eculizumab treatment was 52.7 (1.0, 127.3) months and the total treated patient-years (PYs) was 338.6 PYs. Among the 80 patients included in the study, 67.5% (n = 54) continued to receive eculizumab treatment, while 32.5% (n = 26) discontinued eculizumab. Participation in a clinical trial was the main reason for discontinuing eculizumab treatment (n = 19), and there were no cases that lack of response or deterioration from eculizumab therapy was the reason for participating in clinical trials. Other reasons included other life-threatening diseases (n = 2), investigator judgment (n = 2), deterioration of renal function (n = 1), undergoing a hematopoietic stem cell transplantation (n = 1), and childbirth (n = 1). No cases of treatment discontinuation related to eculizumab were observed. In addition, there were no cases of treatment discontinuation due to inadequate responses or loss of responses to eculizumab in this study.
Table 1
Demographics and clinical characteristics
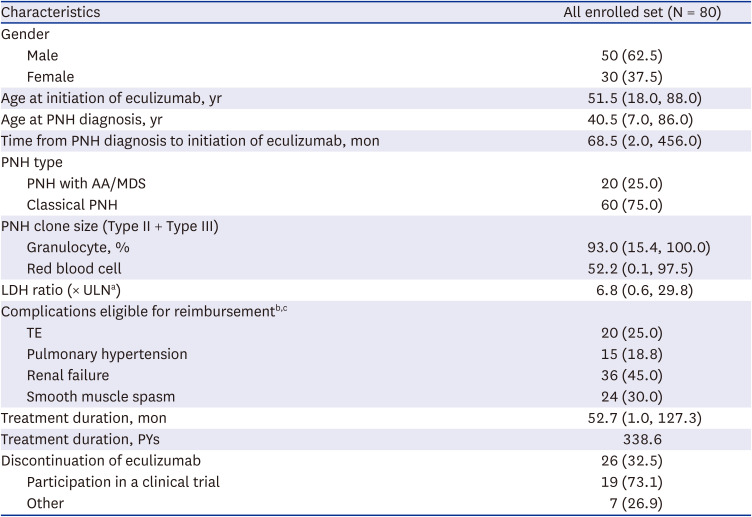
Values are presented as number (%) or median (range).
PNH = paroxysmal nocturnal hemoglobinuria, AA = aplastic anemia, MDS = myelodysplastic syndrome, LDH = lactate dehydrogenase, ULN = upper limit of normal, TE = thromboembolic event, PY = patient-year.
aBased on each site’s laboratory reference range.
bComplications described for the reimbursement review committee of the Health Insurance Review and Assessment Service – description of multiple complications was allowed.
cOne patient started eculizumab treatment owing to pregnancy without specific complications; two patients who were reimbursed during the first review committee (in 2012) have no record of specific complications.
Primary endpoint: efficacy
Hemolysis
The mean ± SD change in LDH (× ULN) from baseline to the last follow-up after eculizumab administration was −6.5 ± 4.7-fold (Fig. 1). LDH levels were stabilized in the majority of patients: 95.0% (n = 76) achieved LDH levels of below 1.5 × ULN and 61.3% (n = 49) achieved LDH levels within the normal range.
Fig. 1
Rapid and sustained control of intravascular hemolysis by eculizumab, and the cumulative incidence of extravascular hemolysis and breakthrough hemolysis during eculizumab treatment. Changes in (A) LDH over time, (B) incidence and time to first occurrence of EVH, and (C) incidence and time to first occurrence of BTH.
LDH = lactate dehydrogenase, EVH = extravascular hemolysis, BTH = breakthrough hemolysis, PY = patient-year, SD = standard deviation, ULN = upper limit of normal.
aTwo patients were excluded for the following reasons: one patient who was pregnant with no complications at initiation of eculizumab and LDH (301 U/L) within the normal range (ULN = 480 U/L) at baseline; and one patient with LDH that was not collected at baseline.
bOne patient had three BTH events.

PNH-related clinical symptoms and complications
There was a decrease in the incidence of some clinical symptoms of PNH after the initiation of eculizumab treatment, including fatigue, anemia, and dyspnea (Supplementary Table 1). It should be noted that the PNH symptoms experienced were collected for only 6 months prior to initiation of eculizumab and compared with the entire follow-up period after eculizumab initiation; if a patient experienced an event at least once during this period it was recorded.
Among 20 patients with reported TEs before eculizumab administration, 14 achieved complete resolution of TEs during eculizumab treatment (Table 2). Cases of deep vein thrombosis were all resolved with eculizumab treatment and there were fewer cases of residual hepatic and portal vein thrombosis, cerebral venous occlusion, and arterial thromboembolism even after eculizumab treatment (Supplementary Table 2). Prior to administration of eculizumab, 75.0% of patients (n = 15/20 with TEs) received anticoagulation therapy; during eculizumab treatment, 60.0% of patients (n = 9/15 with TEs) continued to receive anticoagulation therapy.
Table 2
PNH complications experienced prior to initiating eculizumab and during eculizumab treatment
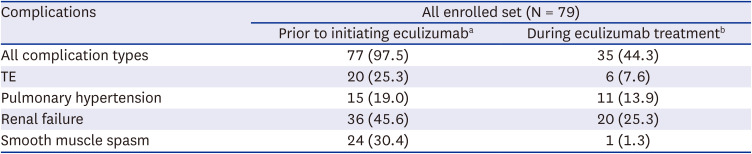
Values are presented as number (%).
PNH = paroxysmal nocturnal hemoglobinuria, TE = thromboembolic event.
aComplications that existed before eculizumab administration.
bComplications that existed before eculizumab administration that were not resolved after administration of eculizumab (if a patient had two or more complications before eculizumab administration, it is included when one persisted after administration).
Of the 24 patients with smooth muscle spasm prior to eculizumab administration, 23 were symptom-free after eculizumab treatment (Table 2). PNH-related complications were resolved with eculizumab treatment in 4 of 15 patients with pulmonary hypertension and 16 of 36 patients with renal failure (Table 2). Among the 15 patients who reported pulmonary hypertension, NT-proBNP (n = 5) and proBNP (n = 4) values were available at both baseline and the last follow-up. The median (range) changes in NT-proBNP and proBNP were −19.9 (−1,060.0, 214.0) pg/mL and −228.0 (−620.1, 31.2) pg/mL, respectively (Supplementary Table 3). Of the 36 patients who reported renal failure prior to eculizumab administration, the eGFR value was recorded in 32 patients. The mean ± SD change in eGFR after eculizumab administration was 28.6 ± 43.2 mL/minute/1.73 m2 (n = 32). The mean ± SD change in eGFR was 6.4 ± 18.6 mL/minute/1.73 m2 in patients with chronic kidney disease (CKD, n = 18) and 57.1 ± 49.3 mL/minute/1.73 m2 in patients with acute kidney injury (AKI, n = 14). When stratified by eGFR levels, CKD improved in 4 patients, was maintained in 12 patients, and worsened in 2 patients; AKI improved in 11 patients, was maintained in 2 patients, and worsened in 1 patient (Supplementary Fig. 1).
Anemia
The mean ± SD Hb level was 9.5 ± 1.7 g/dL at baseline and increased to 10.4 ± 1.9 g/dL at the last follow-up (P < 0.001). In total, 75 patients received a pRBC transfusion within one year prior to eculizumab administration compared with 52 patients after eculizumab administration to the last follow-up. When converting the results into PY, patients received 9.5 units/PY prior to eculizumab initiation compared with 6.8 units/PY during eculizumab treatment (P = 0.008). Transfusion avoidance was achieved by 35.0% of patients (n = 28).
Additional endpoints
EVH events were reported in 28.8% of patients (n = 23; incidence of 0.09 per PY); the median time to the first occurrence of EVH was not reached owing to the small number of events (Fig. 1). Although there were no significant differences in mean LDH levels from the assessment that preceded the occurrence of EVH to occurrence of EVH (1.3 vs. 1.2 × ULN), mean Hb levels decreased slightly from 9.0 to 8.4 g/dL (Supplementary Table 4). The clinical intervention was required in 9 of 23 (39.1%) patients with EVH: 2 received steroid treatment, 6 received blood transfusions, and 1 received both steroids and transfusion. AA was an underlying hematologic condition in 1 of 9 (11.1%) patients with EVH who required intervention and 1 of 14 (7.1%) who did not require intervention.
BTH events were experienced by 18.8% of patients (17 events in 15 patients; 0.06 incidence per PY); the median time to the first occurrence of BTH was not reached owing to the small number of events (Fig. 1). When compared with data from the assessment that preceded the occurrence of a BTH event, BTH was accompanied by a change in LDH of 1.4 × ULN increase (P < 0.001) and a 1.9 g/dL decrease in Hb (P < 0.001) (Supplementary Table 5). Intervention was required in 11 of 15 (73.3%) patients with BTH: 6 patients received blood transfusions, 5 patients received antibiotics to treat infection, and 1 patient received steroids.
The median duration of follow-up was 52.7 months and the 5-year overall survival during eculizumab administration was 96.2% (median not reached owing to the small number of events) (Supplementary Fig. 2).
Safety
Infection occurred in 22.5% of patients (41 events in 18 patients: 0.2 incidence per PY) (Table 3). No infections were caused by N. meningitidis, Neisseria gonorrhoeae, Streptococcus pneumoniae, or Haemophilus influenzae. One case of severe aspergillosis infection was reported during the study period. No cases of infection related to eculizumab were observed.
Table 3
Summary of AEs
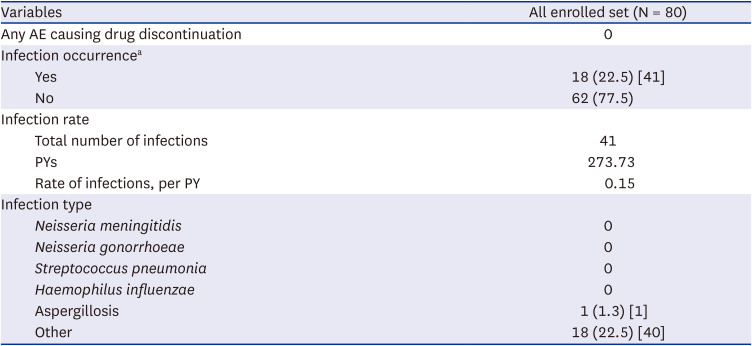
No patients discontinued eculizumab treatment owing to adverse events (AEs). Two deaths were reported within 3 months after eculizumab discontinuation; the deaths were unrelated to eculizumab. One patient died owing to bladder cancer and one died of septicemia/infection (fungal sepsis).
DISCUSSION
In this study of 80 patients with PNH with a high disease burden, eculizumab showed sustained efficacy with control of intravascular hemolysis and PNH-related complications during long-term treatment. Overall survival was 96.2% with eculizumab treatment and only two deaths were reported, both deemed unrelated to eculizumab. Eculizumab was well tolerated, and no AEs led to treatment discontinuation. Among patients who discontinued treatment, participation in a clinical trial was the reason in most cases. No cases of treatment discontinuation related to eculizumab were observed.
Patients enrolled in this study had a high disease burden at eculizumab treatment initiation (median LDH was 6.8 × ULN and median granulocyte clone size was 93.0%) and severe, life-threatening PNH-related signs and symptoms in accordance with the Korean reimbursement criteria. TEs were identified at potentially fatal locations in many cases prior to the administration of eculizumab. Identified TEs included pulmonary embolism, hepatic/portal vein thrombosis, cerebral venous occlusion, and cerebrovascular accidents. Following the administration of eculizumab, most TEs were resolved, and 6 patients were able to discontinue anticoagulation therapy without any new TEs. eGFR data indicated that in patients with AKI, renal function was improved in many cases with eculizumab; however, restoration of renal function was not prominent in patients whose condition had already progressed to CKD.
EVH events were experienced by 23 patients in the study during eculizumab treatment. However, only nine of these patients required therapeutic intervention suggesting that the symptoms were not severe in most cases. In total, there were 15 patients in the study who experienced a BTH event during eculizumab treatment with the incidence of BTH in this study comparable to previously reported data.14 More clinically meaningful changes in LDH and Hb were reported in patients with BTH than in those with EVH, and more patients with BTH required therapeutic intervention than those with EVH.
Although an increased risk of meningococcal infection has been reported in recipients of eculizumab,15 no such infections were observed in this study among 80 patients on long-term eculizumab therapy. It should be noted that prophylactic antibiotics are not used in Korea for the prevention of meningococcal infection during eculizumab treatment, whereas guidelines in some countries recommend their use. The lack of meningococcal infections without prophylactic antibiotics use in this study is an important finding because there are concerns with the emergence of resistant mycobacterium and gastrointestinal side effects associated with long-term use of prophylactic antibiotics with a compliance issue.
One of the strengths of this study is that detailed clinical information for each patient should be reported to the Korean health authority every 6 months for continued eculizumab treatment, ensuring data are collected at consistent intervals for each patient over time. Furthermore, all patients who required red blood cell transfusions had additional blood tests, including a direct Coombs test; as such, and similar to a prospective study, the incidence of EVH and BTH were well documented.
The retrospective nature of these analyses has inherent limitations owing to confounding factors, and results cannot be used to determine cause-and-effect relationships. A notable number of patients discontinued eculizumab during the study period owing to participation in a clinical trial. The data are restricted to patients with PNH in Korea and therefore may not be generalizable to the wider PNH population. As blood levels of free C5 were not evaluated in the study, we could not assess the association of BTH events with free C5 at or above 0.5 µg/mL (the threshold for complete C5 inhibition). PNH symptoms were collected only for 6 months prior to initiation of eculizumab and compared with the entire follow-up period after treatment; this likely contributed to the small differences in the number of symptoms experienced prior to and during eculizumab treatment. NT-proBNP and proBNP data were collected only for a small number of patients with pulmonary hypertension. Despite the small sample size, there was a trend toward improvement in pulmonary hypertension following initiation of eculizumab. Although assessment of the health-related quality of life using the Functional Assessment of Chronic Illness Therapy-Fatigue Scale questionnaire was planned for this study, data were only collected from a small sample (n = 36) and therefore were not presented here.
Eculizumab showed sustained effectiveness during long-term treatment in patients with PNH with a high disease burden and severe PNH-related complications. Eculizumab treatment improved complications and related symptoms in patients with PNH, and overall survival was 96.2% during the study period. Eculizumab was well tolerated over long-term treatment and no treatment-emergent AEs led to discontinuation. Collectively, the data confer the long-term efficacy of eculizumab in patients with PNH who have high disease activity.
 XML Download
XML Download