

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The demand for companion animals in South Korea is increasing because of ongoing social and demographic changes, including a low birth rate and an increasing prevalence of nuclear families and one-person households. Based on a survey conducted in 2017,1 29.4% or 5.74 million out of 19.52 million households in the country were raising pets. Results from a survey indicated that 59.9% of respondents expressed an intention to utilize pet funeral facilities when their companion animals pass away.2 This indicates the emergence of a culture where the death of a companion animal is regarded as a significant loss.2 The loss of a companion animal is often regarded as a major life event and a challenging time for individuals, akin to the death of a loved one and the associated grieving process, which is considered a significant life crisis.34 Following the loss of a companion animal, individuals commonly experience various psychological symptoms, including changes in sleep and appetite, feelings of distrust, longing, loneliness, self-blame, anxiety, anger, depression, sadness, and emptiness.456
Complicated grief (CG) is a prolonged and maladaptive response to loss that exceeds the culturally accepted mourning norms. In the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), Prolonged Grief Disorder (PGD) is defined as grief that is intense, lasting, and interferes with daily functioning for at least one year.7 Due to the nature of the relationship where pet owners are solely responsible for the care of their pets, the loss of a pet can lead to heightened feelings of guilt compared to the loss of a human companion.8910 The unique characteristics of pet loss make individuals more vulnerable to experiencing CG or PGD.61112 Furthermore, the experience of pet loss is often marginalized and lacks sufficient social support. Despite the growing awareness of the significance of psychological interventions in response to mental health crises stemming from pet loss, research on the prevalence of those who require clinical intervention is limited.
Numerous studies have shown that variables such as cognitive attachment to the pet, duration of the relationship with the pet, unexpected loss, and type and duration of the pet's illness are related to grief after pet loss.6131415 These variables may influence the degree and impact of grief after the loss of a pet.314 In previous studies, childhood trauma experiences are proposed to increase sensitivity to stress in adulthood, thereby exerting ongoing negative effects on mental and physical health.16 Adults with a history of childhood trauma tend to exhibit heightened emotional responses to everyday life stressors compared to those without such experiences.17 Adults who have experienced such trauma were found to have increased sensitivity to recent stressful life events,18 and they are at risk of developing CG following the death of a close person, such as a spouse or friend.19 Recent studies have shown that adults with a history of childhood trauma exhibit higher levels of grief reactions following the loss of a spouse.20 However, the relationship between a history of childhood trauma and the presence of psychiatric symptoms in the context of pet loss remains unexplored in the current literature.
This study investigated the rates of clinically significant psychological distress after pet loss and examined the association between childhood trauma and these psychological symptoms in adults who have experienced pet loss.
METHODS
Participants
A cross-sectional questionnaire survey of a random sample of the general Korean population was conducted via online contact. Participants were recruited through online platforms and promotional posters at the Kyungpook National University Hospital. Participants were selected based on the following criteria: healthy adults aged 20 years and above without any history of psychiatric disorders. Participants without pet loss or under 20 years of age were excluded from the study. Among the initial-327 participants, 218 (66.6%) consented and completed all questions. Eighty-one participants who exhibited low response reliability, such as consistently providing identical responses or displaying a narrow range of responses, were excluded from the analysis. Participants who scored 41 or higher on the Korean version of the Childhood Trauma Questionnaire (CTQ) were assigned to the trauma group, while those with a total score below 41 were assigned to the non-trauma group.21 Participants were further categorized according to the DSM-57 definition of PGD using one year after pet loss as a criterion.
Measures
Demographic variables, including sex, age, marriage, level of education, type of pet, and time since death, were collected. Participants also completed the CTQ, the Inventory of Complicated Grief (ICG), the Patient Health Questionnaire-9 (PHQ-9), the Generalized Anxiety Disorder-7 (GAD-7), and the Insomnia Severity Index (ISI).
The CTQ, a self-report measure assessing childhood trauma experiences developed by Bernstein and Fink in 1997.21 The CTQ consists of 28 items rated on a 5-point Likert scale (1 = never true to 5 = very often true) and assesses five types of neglect and abuse experiences (physical abuse, physical neglect, emotional abuse, emotional neglect, and sexual abuse) through five subscales, each with a score range of 5–25 points. A total score of 25–40 indicates no or minimal childhood trauma experiences, while a score of 41 or higher indicates significant trauma experience.21 This study used the Korean version of the CTQ for assessment.22
The ICG is a measure designed by Prigerson et al.23 in 1995 to assess pathological grief reactions that extend beyond normal and culturally accepted levels of bereavement and result in sustained psychological maladaptation. The measure consists of a 19-item self-report questionnaire to assess pathological grief reactions. Each item is rated on a 5-point scale ranging from “not at all (0)” to “always (4)”.23 The original developers reported high internal consistency (Cronbach's alpha = 0.94). There is one validation study about the Korean version of ICG in Korean adolescents.24 Prigerson et al.23 have previously suggested a threshold of 25 points to identify individuals at a higher risk of requiring treatment. In this study, we adopted the same cut-off of 25 points for identifying individuals at higher risk.
The PHQ-9, developed by Spitzer et al.25 in the late 1990s, is a 9-item questionnaire corresponding to the diagnostic criteria for major depressive disorder presented in the DSM-IV. The Korean version of the PHQ-9, translated and adapted by Han et al.26 has good psychometric properties. The Cronbach's α value of all items was 0.852. The sensitivity and specificity of the Korean version of PHQ-9 were 81.8% and 89.9%, respectively.27 In a meta-analysis, a cut-off score of 8 to 11 was suggested as a threshold for major depressive disorder.28 We considered a cut-off score of 10 as the threshold for major depression.
The GAD-7 was developed by Spitzer et al.29 in 2006 to screen for generalized anxiety disorder, and was later validated by Kroenke et al.30 in 2007 for use in screening for other anxiety disorders such as panic disorder, social anxiety disorder, and post-traumatic stress disorder. It consists of seven questions rated on a 4-point scale (0–3, not at all to nearly every day) to assess anxiety symptoms in the past two weeks, with a total score range of 0 to 21.29 The total score was calculated by summing the scores assigned to each item based on the symptom frequency. The cutoff score for clinical significance is 10 or above, and the internal consistency (Cronbach's α) is 0.92.31 In a cut-off study targeting the general population, scores of 5 or higher were classified as mild anxiety, 10 or higher as moderate anxiety, and 15 or higher as severe anxiety.32 In this study, we analyzed the data using a cutoff score of 10.
Data analysis
The psychological characteristics of the 137 participants who completed the survey were analyzed using descriptive statistics, including means and standard deviations (SD). We classified our study participants into two groups based on the time since pet loss, specifically whether the grief reaction persisted for at least one year after pet loss, in accordance with the diagnostic criteria for PGD, as outlined in the DSM-5.7
To investigate the effect of childhood trauma on psychological outcomes after pet loss, we categorized 137 participants into two groups: a non-trauma group, defined as those with a total score on the CTQ scale of less than 41 points, and a trauma group, defined as those with a total score of 41 points or higher. Categorical variables such as demographic data, were compared between the two groups using the χ2 test, and continuous variables were compared using the independent t-test. Pearson’s correlation analysis measured the relationship between the CTQ and the ICG among the trauma group with pet loss for more than one year. Partial correlation analysis was used to control for the PHQ-9. All statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS) version 21.0 (IBM Corp., Armonk, NY, USA).
RESULTS
Cross-sectional comparison of psychological characteristics
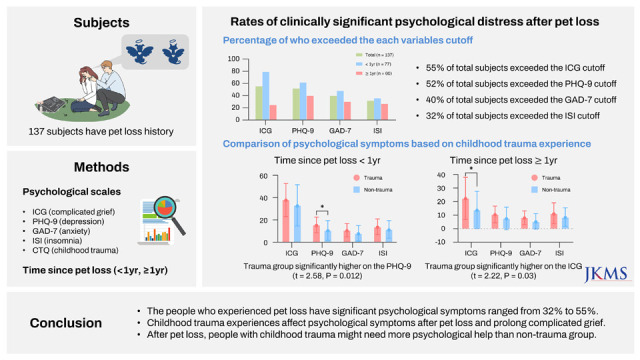
Of the 137 participants who experienced pet loss, 55% (76 participants) exceeded the cut-off score of 25 points on the ICG (28.24 ± 18.18), 52% (72 participants) exceeded the cut-off score of 10 points on the PHQ-9 (11.58 ± 8.13), 40% (55 participants) exceeded the cut-off score of 10 points on the GAD-7 (8.04 ± 6.27), and 32% (44 participants) exceeded the cut-off score of 16 points on the ISI (11.6 ± 7.54) (Table 1).
Table 1
Psychological characteristics in total subjects, pet death less than one-year and pet death over one-year groups

Among the group of 77 participants who had pet loss within one year, 79% (61 participants) reported exceeding the cutoff for the ICG (36.00 ± 16.55), 62% (48 participants) on the PHQ-9 (13.64 ± 8.18), 48% (37 participants) on the GAD-7 (9.81 ± 6.52), and 36% (28 participants) on the ISI (13.05 ± 7.40) (Table 1).
Among the group of 60 participants who had pet loss more than one year ago, 25% (15 participants) reported exceeding the cutoff on the ICG (18.28 ± 15.15), 40% (24 participants) on the PHQ-9 (8.93 ± 8.18), 30% (18 participants) on the GAD-7 (6.58 ± 5.46), and 27% (16 participants) on the ISI (9.75 ± 7.37) (Table 1).
Demographic and psychological differences between trauma and non-trauma groups
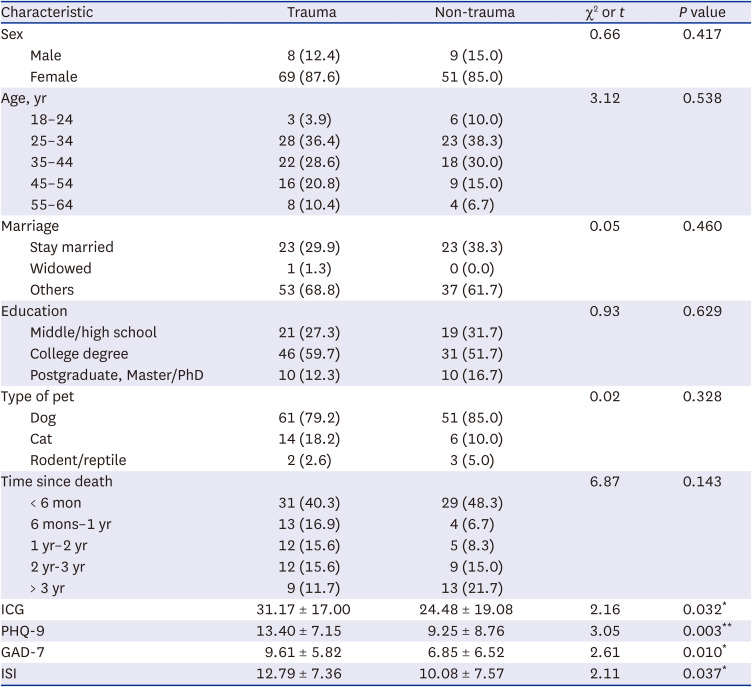
This study analyzed two groups of individuals based on 41 points on the CTQ: those who reported a history of trauma (8 males and 69 females) and those who did not (9 males and 51 females). The mean score on the CTQ was 56.42 (SD, 14.67) for the trauma group and 31.93 (SD, 4.76) for the non-trauma group. The two groups had no significant differences regarding sex, age, marital status, or education level. Moreover, no significant difference was observed between the two groups regarding the type of lost pet and duration of pet loss (P > 0.05, Table 2). The trauma group showed significantly higher scores on the ICG (t = 2.16, P = 0.032), the PHQ-9 (t = 3.05, P = 0.003), the GAD-7 (t = 2.61, P = 0.010), and the ISI (t = 2.11, P = 0.037) than the non-trauma group (Table 2).
Table 2
Epidemiological and psychological characteristics between the trauma group and non-trauma group
Comparison of psychological variables between trauma and non-trauma groups for pet loss less than one year
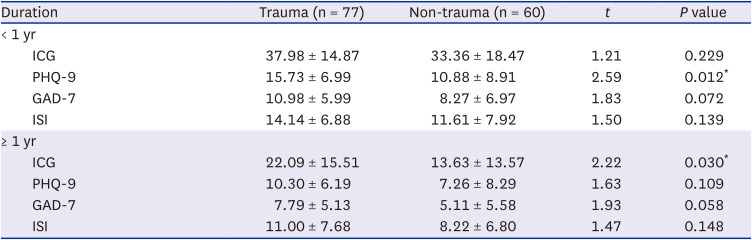
A total of 77 participants, with 8 males and 69 females, who experienced pet loss less than one year ago and were divided into trauma and non-trauma groups. The ICG scores were reported as high, exceeding the cutoff score in both groups, with a mean of 37.98 (SD, 14.87) and 33.36 (SD, 18.47) in the trauma and non-trauma groups, respectively. However, there was no significant difference between the two groups regarding the ICG (t = 1.21, P = 0.012). The PHQ-9 scores were both above the cutoff in both groups, with a mean of 15.73 (SD, 6.99) in the trauma group and 10.88 (SD, 8.91) in the non-trauma group, and there was a significant difference between the two groups (t = 2.59, P = 0.012). The results showed no significant differences in GAD-7 and ISI scores between the trauma and non-trauma groups. The trauma group had a mean GAD-7 score of 10.98 (SD, 5.99), whereas the non-trauma group had a mean score of 8.27 (SD, 6.97). Similarly, the mean ISI score was 14.14 (SD, 6.88) for the trauma group and 11.61 (SD, 7.92) for the non-trauma group (Table 3).
Table 3
Psychological characteristics between the trauma and non-trauma group based on time since pet loss (< 1 yr or ≥ 1 yr)
Comparison of psychological variables between trauma and non-trauma groups for pet loss more than one year
For a group of 60 participants, 9 males and 51 females, who experienced pet loss more than one year ago, divided into trauma and non-trauma groups, the trauma group had the mean ICG score of 22.09 (SD, 15.51). In contrast, the non-trauma group had a significantly lower score of 13.63 (SD, 13.57), resulting in a statistically significant difference between the two groups (t = 2.22, P = 0.030). The mean PHQ-9 score for the trauma group was 10.30 (SD, 6.19) and 7.26 (SD, 8.29) for the non-trauma group, with no significant difference between the two groups (t = 1.63, P = 0.109). There was no significant difference in the GAD-7 and ISI scores between the trauma and non-trauma groups. The mean GAD-7 score for the trauma group was 7.79 (SD, 5.13) and 5.11 (SD, 5.58) for the non-trauma group, and the mean ISI score was relatively low in both groups, with 11.00 (SD, 7.68) for the trauma group and 8.22 (SD, 6.80) for the non-trauma group (Table 3).
Correlation between the CTQ and the ICG scores in individuals experiencing pet loss for more than one year
A correlation analysis was conducted on 33 individuals who reported experiencing childhood trauma and pet loss for at least one year. The results showed a significant positive correlation between the total CTQ and the ICG scores (r = 0.594, P < 0.001). This trend persisted even after adjusting for depression scores, particularly for physical abuse (r = 0.455, P = 0.009), emotional abuse (r = 0.620, P < 0.001) and sexual abuse (r = 0.351, P = 0.049) (Table 4).
Table 4
Relationship between the ICG, the CTQ and abuse subtypes of the CTQ for the trauma group of pet loss more than 1 year (n = 33)

DISCUSSION
The present study, conducted with a sample of 137 adults, aimed to investigate psychiatric symptoms in adults who experienced pet loss, while exploring the association between childhood trauma experiences and such symptoms. Four main findings emerged: First, the loss of a pet can result in significant stress, with symptoms that may require psychological intervention, such as CG, depression, anxiety, and sleep disorder, particularly prevalent within the first year following the loss. Second, individuals with a history of childhood trauma were more likely to experience CG, depression, anxiety, and insomnia in response to the loss of pets. Third, individuals with a history of childhood trauma exhibited higher levels of depression symptoms within the first year following pet loss, and higher levels of CG reaction one year after a loss than individuals without trauma experience. Fourth, regarding the evaluated trauma group over one year since pet death, childhood trauma positively correlates with PGD.
A previous study found that 20% of subjects who experienced spousal bereavement exceeded the cutoff for the ICG.23 The study found that the mean ICG score for the 137 respondents who had lost a pet exceeded the cutoff point, with 55% (76 respondents) reporting scores indicating the need for treatment. Furthermore, more than half of the respondents self-reported scores on the PHQ-9 indicating major depressive disorder, 40% reported experiencing moderate to severe anxiety on the GAD-7, and 32% reported experiencing moderate to severe insomnia. This suggests that pet loss can cause significant psychological stress, leading to CG, depression, anxiety, and sleep disorder, regardless of childhood traumatic experience.
However, the significant psychological stress caused by pet loss is often not understood or empathized within social and cultural contexts, resulting in a lack of social support such as bereavement leave or condolence payments. Our results suggest that many individuals experience psychological distress following the loss of a pet, underscoring the need for psychological support and a social understanding-of pet loss. Specifically, our study emphasizes the critical need for psychological and social support within the first year after the loss of a pet, as indicated by the significantly higher mean scores on measures of psychological symptoms during this period.
Additionally, the group with childhood trauma experiences showed statistically significantly higher scores on the ICG, the PHQ-9, the GAD-7, and the ISI than the group without childhood trauma. While research on the relationship between childhood trauma experiences and grief reactions to pet loss is scarce, one study has reported that adults with childhood trauma experiences showed higher scores on the depression scale after experiencing the loss of a spouse compared to a control group.20 The results of this study and previous research1635 support the hypothesis that individuals who have experienced childhood trauma are more sensitive to stressful events in life, both psychologically and physically. Considering that childhood trauma is an important predictor of negative mental health outcomes, medical professionals should pay more attention to recent life stressors, such as pet loss, in patients with such experiences.
Specifically, when analyzed by dividing based on one year after the loss of a pet, if pet loss occurred within one year, the ICG score was high regardless of the presence of childhood trauma, showing no significant difference. However, the PHQ-9 score was significantly higher in the trauma group than in the non-trauma group, indicating the need for clinical evaluation and management of depressive symptoms within one year of pet loss. Conversely, if pet loss occurred more than one year ago, the PHQ-9 score decreased, resulting in no significant difference between the two groups. However, the ICG score remained high in the trauma group, suggesting the need for evaluation and intervention for PGD in patients who have experienced childhood trauma.
To explore further, a positive correlation was found between the CTQ and the ICG for the childhood trauma group with pet loss more than one year ago, even when controlling for depressive symptoms. Among these correlations, physical, emotional, and sexual abuse were correlated with the ICG scores. Previous studies have suggested that physical, emotional, and sexual abuse during childhood may result in insecure attachment styles in adulthood.3637 Therefore, the current study suggests that adults with insecure attachment to people after childhood trauma may become more attached to their pets and subsequently develop excessive preoccupation, thoughts about the pet, and a greater sense of emptiness following pet loss.
This study has a few limitations. First, most participants (87.6%) were female, which may have affected the generalizability of the findings to a larger population. Females are sensitive not only to depression and anxiety but also at high risk of developing CG after major bereavement.383940 Therefore, the reported results of depression, anxiety disorders, and CG following the loss of a companion animal in this study may have been exaggerated. Additionally, since this study was conducted using anonymous internet surveys, there is a possibility that people who have experienced psychological distress after losing their pets are more likely to respond, which could introduce a sampling bias. Second, the study did not measure pre-existing depression, anxiety, or insomnia before pet acquisition, which could have confounding effects on the relationship between pet loss and CG. Future research could benefit from considering these psychological factors both before and after pet loss to better understand their potential impact on the occurrence of CG. Third, the level of attachment between the pet owner and the pet is a factor that can affect the occurrence of CG,14 but this was not controlled for in this study. It should also be noted that the reason for the pet's death was not examined. How a pet dies, whether through euthanasia or natural death, can affect pet owners’ emotions. Research has shown that caregivers tend to exhibit more anger when euthanasia is involved, and less anger when cancer is involved.6 Therefore, the lack of investigation of the cause of death is a limitation of this study.
To the best of our knowledge, this is the first study to report the prevalence of those who require clinical intervention after pet loss and to verify the relationship between childhood trauma and psychiatric symptoms responses following pet loss. It is crucial to recognize the need for psychological support following the loss of a companion animal, as many individuals experience psychological symptoms within one year. Specifically, those who had experienced childhood trauma were more likely to report symptoms. However, the childhood trauma group tended to report more severe depressive symptoms within one year and more severe CG symptoms after one year. Therefore, it is important to provide psychological assistance in consideration of these findings.
Additional research is needed to explore the longitudinal interactions between childhood trauma and pet loss-induced psychiatric distress in subjects with adequate demographic control.
 XML Download
XML Download