

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Live birth is the final goal of in vitro fertilization-embryo transfer (IVF-ET). As in natural conception, unsuccessful pregnancy, including early pregnancy loss, ectopic pregnancy, molar pregnancy, fetal death in utero, or stillbirth, can occur after IVF-ET. In addition to the physical and financial burden, any abortive outcome has a devastating emotional impact on couples undergoing IVF-ET cycles.
Socioeconomic status (SES), whether measured by education, income, or other indices of social position, has a significant impact on health.12 Epidemiological associations between socioeconomic disadvantages and increased adverse feto-maternal outcomes have been previously reported.3 When SES is low, medical care is inadequate,45 and certain lifestyle factors can adversely affect health outcomes.26 In pregnant women, low SES can increase the risk of adverse pregnancy outcomes, such as abortion, preterm delivery, preeclampsia, eclampsia, gestational diabetes, and low birth weight or small-for-gestational-age.789 A recent study suggested that low SES is related to stressors, and inflammation is a pathway for adverse birth outcomes.10
In October 2017, the South Korean government started universal health insurance coverage for IVF-ET procedure for people experiencing infertility.1112 Consequently, from October 2017 to December 2019, approximately 100,000 cycles benefited from health coverage for IVF-ET cycles.1314 This change enabled the study of outcomes of individuals who became pregnant after IVF-ET cycles by considering socioeconomic factors and underlying medical conditions. We explored the association between socioeconomic factors and pregnancy-risk outcomes in women with clinical pregnancy after IVF-ET.
METHODS
Data
This retrospective observational study used data from the National Health Information Database of the National Health Insurance (NHI) Service of South Korea. Over 95% of all Korean nationals living in South Korea have been covered by the NHI since 1989. The National Insurance database holds demographics, including employment status, household income in percentile-ranking, residential district information, and clinical information on diagnoses, prescribed medications, procedures, and treatments covered by the NHI for every visit to a health facility. We constructed a national cohort of pregnant women with diagnostic codes of pregnancy (starting with ‘O’) and having undergone health examinations at least once, using the NHI data available up to December 2019. We then ascertained clinical pregnancy after ET by pinpointing the emergence of diagnostic codes for pregnancy within 8 weeks of the treatment code for ET, which began in October 2017. According to the governmental policy of Korea, it is mandatory to report all outcomes of ET cycles supported by the NHI, supplying reliable estimates of pregnancy outcomes after ET cycles. To find pregnancy outcomes, including delivery, which is obtainable almost 10 months after ET, our analyses were restricted to 44,038 clinical pregnancy episodes of 29,847 women who underwent ET between October 2017 and February 2019. Given that the total number of women who have undertaken ET cycles was 92,105, and the clinical pregnancy rate after IVF-ET was 35.4% during the same period,15 our study population corresponds to 91.5% of all nationwide clinical pregnancy cases after IVF-ET. In the analyses of probabilities of IVF treatment among those diagnosed with female infertility, we retrieved all women diagnosed with infertility aged 25–45 years (n = 37,764) during the study period based on the International Classification of Diseases 10th Revision code (‘N97’, female infertility). This study was carried out in accordance with the REporting of studies Conducted using Observational Routinely-collected Data guidelines.
Socioeconomic factors
We assessed individual SES using the information on income percentile ranking, employment, living in the Seoul capital area (Seoul, Incheon, and Gyeonggi-do), where half of the South Korean residents and 47% of nationally registered IVF centers, as well as social infrastructure, are found. Variables were selected based on prior knowledge and availability in the NHI database. The employment status of women is coded based on the NHI subscription type, which specifies employees. The Korean NHI cohort database includes individually linked household income decile data. The household income levels of individual data were divided into four groups (1st [lowest]: 10–30%, 2nd: 40–60%, 3rd: 60–80%, and 4th [highest]: 80–100%) for analytical convenience. Information on employment (yes, no) and residential area (at the district level) was coded based on the type of insurance subscription.
Pregnancy outcomes
We classified live births based on the co-presence of diagnosis codes for pregnancy and treatment codes for delivery within 273 days (39 weeks) of ET, which corresponds to 41 weeks of gestation. Abortive pregnancy outcomes, including abortion (both miscarriage and termination of pregnancy), ectopic pregnancy, and molar pregnancy, were defined as presence of diagnostic codes within 20 weeks of ET to show valid pregnancy outcomes (Supplementary Table 1). Stillbirth was defined as the stillbirth or fetal death in utero codes within 42 weeks of ET. When there are two or more diagnostic codes for different pregnancy outcomes, conditions are likely to require laboratory or histological confirmation. For example, if diagnostic codes for both ectopic pregnancy and abortive pregnancy outcomes are present, ectopic pregnancy is assigned.
Statistical analysis
Descriptive statistics of baseline demographic information, relevant obstetric history (parity, fresh ET, year, and month of ET), and clinical characteristics, including body mass index (BMI), anemia, fasting glucose level, and history of smoking, were calculated for all ET cycles. To assess the association between socioeconomic factors and the risk of abortive outcomes, we used log-binomial regression models to calculate the adjusted relative risk (RR) of abortive pregnancy outcomes after ET. Covariates included relevant obstetric history (parity, fresh ET, year, and month of ET), and clinical characteristics, including BMI, anemia, fasting glucose level, and history of smoking. Because the incidence of each specific abortive outcome is as low as less than 5%, we aggregated the outcomes to ‘any abortive outcomes’ in calculating adjusted risk estimates. To analyze the origin of socioeconomic disparity in the abortive outcomes in IVF pregnancies, the probabilities of IVF treatment per medical beneficiaries, employment status, and residential region among those diagnosed with female infertility were examined. For the adjusted odds ratio (OR) of each adverse pregnancy outcome according to socioeconomic gradient, we applied multinomial logistic regression model including the covariates. We further explored the effect modification by women’s advanced age in the association between socioeconomic factors and the risk of abortive outcomes. All statistical analyses were performed using SAS software (version 9.4; SAS Institute, Cary, NC, USA) and R version 4.0.2 (R Foundation, Vienna, Austria).
RESULTS
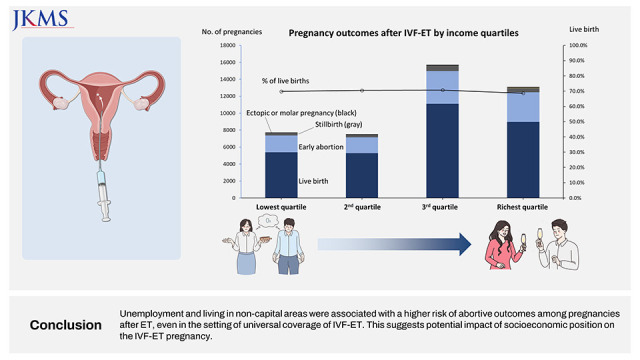
A total of 29,839 women were identified from 44,038 clinical pregnancies after ET. The majority were aged 35–39 years (45.8%) and with higher-than-national median income (65.1%) (Table 1). Sixty percent of the pregnancies were in paid employment, and 57.6% lived in Seoul capital area. While 93.4% had normal or low body weight, and anemia (46.9%) were prevalent in the study population. A majority of women (89.5%) had no prior history of childbirth. Fifty-two percent (n = 22,896) of pregnancies occurred after fresh ET, and 66.0% (n = 26,706) involved intracytoplasmic sperm injection. Most pregnancy outcomes were live births (30,783, 69.9%). Among the rest of the cases, 11,215 (25.5%) cycles ended with abortion or early pregnancy loss, 1,779 (4.0%) cycles were ectopic pregnancy, 45 (0.1%) were coded as molar pregnancy, and 224 (0.5%) were fetal death in utero or stillbirth (Supplementary Table 1). Miscarriage increased with increasing age groups and was notably increased in women aged ≥ 40 (43.2%). The proportion of ectopic pregnancy, molar pregnancy, and fetal death were consistent regardless of age group. Advanced age, unemployment, disability, and frozen ET were associated with a higher risk of abortive outcomes. Linear trends across income levels were not clear. BMI < 18.5 and ≥ 30 kg/m2 were to some extent associated with miscarriage.
Table 1
Characteristics of 29,839 women with 44,038 clinical pregnancies after ET between November 2017 and February 2019, the National Health Information Database of South Korea
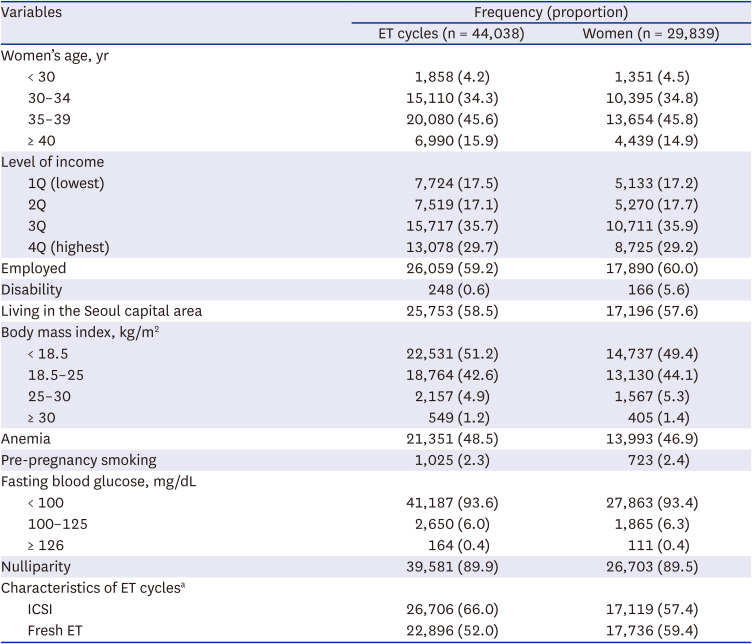
1Q = 1st quartile (the lowest), 2Q = 2nd quartile, 3Q = 3rd quartile, 4Q = 4th quartile (the highest), ICSI = intracytoplasmic sperm injection, ET = embryo transfer.
aFor women who had more than one ET cycles, those underwent the procedure at least once were classified as ICSI or fresh ET, respectively.
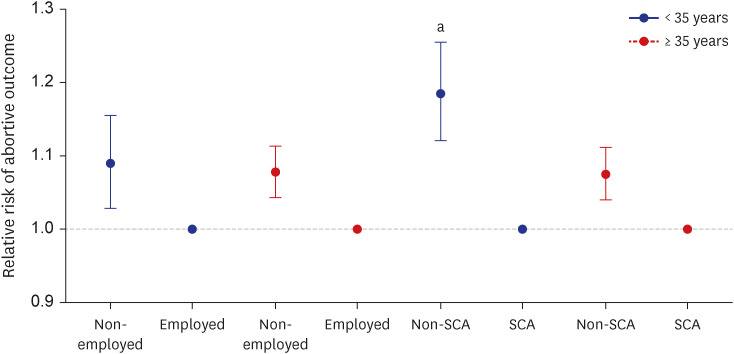
In pooled ET cycles, crude risks of miscarriage, ectopic pregnancy, and stillbirth for medical aid beneficiaries were higher when the women were in non-employed position. For risk of miscarriage living in the non-Seoul capital area was associated with higher risk. Those risks were close to null for medical aid beneficiaries (Supplementary Table 2). Adjusted RR for abortive outcomes was higher when a woman was unemployed (adjusted RR, 1.08; 95% confidence interval [CI], 1.05–1.11), lived in a non-Seoul capital area (1.11; 95% CI, 1.08–1.14) (Table 2). The association between relative income level and the risk of abortive outcomes was close to null. This pattern of association was consistent in the stratified analysis of fresh or frozen ET, with a stronger association for unemployed women in fresh cycles (1.11; 95% CI, 1.06–1.15) compared with those in frozen cycles (1.05; 95% CI, 1.01–1.10). When we categorized the population into medical aid beneficiaries and NHI subscribers, the risks of abortive outcomes were similar between the two groups (Supplementary Table 3). For each of adverse pregnancy outcome, the adjusted OR was consistently higher when the woman is non-employed and living outside of Seoul capital area. The risk estimates of living outside of Seoul were generally imprecise for ectopic or molar pregnancy and fetal death due to low incidence of these outcomes (Supplementary Table 4). In further tests of effect modification, the association between living in the non-Seoul capital area and the high-risk abortive outcome was stronger when a woman’s age was less than 35 years (1.19; 95% CI, 1.12–1.25) than when 35 years or older (1.08; 95% CI, 1.04–1.11; Fig. 1). In the analyses of probabilities of receiving IVF treatment according to medical aid or NHI subscription, the lower probability of having IVF after the diagnosis of female infertility was observed in the medical aid beneficiaries than in the NHI subscribers (Supplementary Table 5).
Table 2
Adjusted RR of any type of abortive outcomes in 44,038 clinical pregnancies after ET between November 2017 and February 2019, the National Health Information Database of South Korea
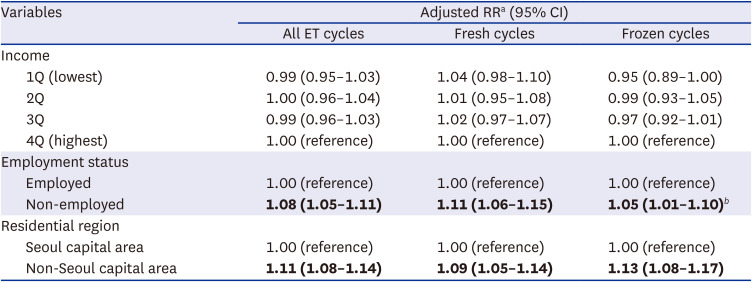
Abortive outcomes include miscarriage or molar pregnancy, ectopic, and fetal death, or stillbirth. Estimates with P < 0.05 were bolded.
ET = embryo transfer, RR = relative risk, CI = confidence interval, 1Q = 1st quartile (the lowest), 2Q = 2nd quartile, 3Q = 3rd quartile, 4Q = 4th quartile (the highest).
aAdjusted for relevant obstetric history (parity, fresh ET, year, and month of ET), and clinical characteristics, including body mass index, anemia, fasting glucose level, and history of smoking.
bEstimates are different between fresh and frozen cycles with statistical significance (P < 0.05).
Fig. 1
Effect modification by women’s age (< 35 or ≥ 35 years) in the association of employment status and living in the SCA with risk of abortive outcomes in 44,038 clinical pregnancies after embryo transfer between November 2017 and February 2019.
SCA = Seoul capital area.
aP for heterogeneity < 0.05
DISCUSSION
Being unemployed and living outside the Seoul capital area were associated with a higher risk of abortive outcomes in both fresh and frozen ET cycles. These findings were consistently observed regardless of adverse pregnancy outcomes. We observed a close-to-null association between the relative level of income and the risk of abortive pregnancy outcomes in South Korean women after ET procedures. When controlling for the effect of covariates, a relatively lower income level may not be a risk factor for adverse pregnancy outcomes once clinical pregnancies are achieved after ET. Using national insurance data from the first two years of IVF coverage, this study provides real-world evidence of the association between SES and pregnancy outcomes among infertile patients.
The lower risk of abortive outcomes in our study in employed women contradicts reports showing a generally higher abortion risk in working women.16 Occupational exposure to physical or psychological stress and hazards has been suggested to cause adverse pregnancy outcomes.1718 Since there was no information about the type of occupation of the women, we could not establish an occupational hazard that might have affected pregnancy outcomes. Furthermore, healthy workers may have a positive lifestyle, such as regular work and sleep. Adequate work may increase blood flow to the placenta, even though physically demanding work during pregnancy is associated with an increased risk of adverse pregnancy outcomes.19 When comparing with women who are out of labor market, employed women may have better access to health care and more likely to show healthy pregnancy-related behaviors.20 Notably, there also can be a risk of reverse causation in this study because women who had several unsuccessful IVF pregnancies or repeated miscarriages are more likely to leave their jobs.
Many studies have shown a higher risk of spontaneous abortion among those in more deprived socioeconomic positions, such as low income or below upper secondary education.16 In general Korean women, abortion and stillbirth rates were higher in women in the lowest income quartile.21 Low-income infertility patients showed lower probability of live birth than their counterparts.22 This inconsistency could be due to the higher educational and economic levels of pregnant women underwent the IVF-ET procedure. Given the lower probability of having IVF after the diagnosis of female infertility of medical aid beneficiaries than NHI subscribers, our finding would have attributed to the generally better condition of those who received IVF treatment among medical aid beneficiaries. Compared to natural pregnancies, IVF pregnancies tend to receive frequent antenatal check-ups. The women take folic acid and other vitamins from preconception and regularly exercise. Thus, factors associated with adverse pregnancy outcomes in low SES, such as inadequate antenatal check-ups or an unhealthy lifestyle, would be minimized in pregnancies after ET. Living outside highly urbanized capital areas, on the other hand, could mean limited access to optimal antenatal treatment or longer travel distance to medical care because of physician shortages in rural areas.
The positive association between adverse pregnancy outcomes and woman’s non-employment is not consistently observed in prior studies of general population.23 Working status has been considered to be a source of selection bias which may negate the harmful impact of working environment.24 Since we included only those with IVF pregnancy, the non-employed women of our study population would be more likely to be less optimal condition than those in general population leading to higher risk of abortive pregnancy outcomes than employed women. This finding remained significant for ectopic pregnancy and fetal death, and this can be explained by their less healthy behavior than their counterparts.25
This study should be interpreted with caution. There is potential misclassification of pregnancy outcomes because our analysis was based on administrative data. Some cases within 8 weeks of the ET procedure might have been spontaneous pregnancies. Given that the spontaneous pregnancy rate immediately after an IVF-ET cycle in infertile patients is presumed to be exceptionally low, we believe that the impact of this misclassification would have been minimal. Secondly, there may be residual confounding effects due to unmeasured factors. For example, we did not consider the cause and duration of infertility, which are important predictors for abortive outcomes. To confirm our findings, an analysis of individual data linked to further medical history is necessary. Lastly, the unfavorable outcomes in women living in non-Seoul capital area cannot be delineated from the impact of location of the IVF providers. Given there is a substantial gap in the quantity and quality of the service related to the IVF treatment, identifying the source of geographical disadvantage would be important. Because our customized database did not contain the information of IVF providers, however, we could not conduct the analysis. We propose future studies that can address this issue.
In conclusion, we report socioeconomic risk factors for abortive outcomes in pregnancies after ET. This would assist further studies on the non-medical determinants of a live birth after IVF-ET in the general population.
 XML Download
XML Download